White blood cell count levels are associated with inflammatory response and constitute independent outcome predictors in adult patients with acute myeloid leukemia aged <60 years
Michael Ozga, Deedra Nicolet, Krzysztof Mrózek, Christopher J. Walker, James S. Blachly, Jessica Kohlschmidt, Shelley Orwick, Andrew J. Carroll, Richard A. Larson, Jonathan E. Kolitz, Bayard L. Powell, Richard M. Stone, John C. Byrd, Ann-Kathrin Eisfeld, Alice S. Mims
{"title":"White blood cell count levels are associated with inflammatory response and constitute independent outcome predictors in adult patients with acute myeloid leukemia aged <60 years","authors":"Michael Ozga, Deedra Nicolet, Krzysztof Mrózek, Christopher J. Walker, James S. Blachly, Jessica Kohlschmidt, Shelley Orwick, Andrew J. Carroll, Richard A. Larson, Jonathan E. Kolitz, Bayard L. Powell, Richard M. Stone, John C. Byrd, Ann-Kathrin Eisfeld, Alice S. Mims","doi":"10.1002/ajh.27465","DOIUrl":null,"url":null,"abstract":"<p>Acute myeloid leukemia (AML) is a biologically and clinically heterogenous disease with diverse genetic abnormalities<span><sup>1-6</sup></span> and a wide-ranging white blood cell counts (WBC) at diagnosis.<span><sup>1</sup></span> The 2022 European LeukemiaNet (ELN) genetic-risk classification incorporates cytogenetic and selected molecular alterations to define Favorable, Intermediate, and Adverse genetic-risk groups providing valuable prognostic information.<span><sup>1</sup></span> Pretreatment WBC levels are also a main prognostic factor for patients with AML;<span><sup>7, 8</sup></span> however, there are no standardized WBC-associated groups that improve prognostication for younger patients. de Jonge et al.<span><sup>9</sup></span> first investigated the impact of WBC on outcome of AML patients harboring <i>NPM1</i> mutations and <i>FLT</i>3 internal tandem duplications (<i>FLT3</i>-ITD) that were divided into three WBC groups: <20 000/μL, WBC 20 000/μL–100 000/μL, and ≥100 000/μL. We decided to build upon this previous work by analyzing a larger, clinically and molecularly well-characterized cohort of 1121 younger (aged <60 years) adults with de novo AML to define clinically relevant WBC level groups and determine their potential independent prognostic impact and associations with gene-expression profiles.</p><p>We defined three WBC groups: <i>low</i> (<10 000/μL, <i>n</i> = 298 patients), <i>intermediate</i> (10 000–49 999/μL, <i>n</i> = 488), and <i>high</i> (≥50 000/μL, <i>n</i> = 335). These groups were chosen because there was no correlation with an observable steady decrease in any analyzed outcome endpoint, including disease-free (DFS), event-free (EFS), or overall (OS) survival, with WBC increasing above 50 000/μL by 10 000/μL increments, nor were there any linear changes in endpoints associated with WBC decreasing below 10 000/μL in 1000/μL increments across the entire cohort (Figure S1A,B). All patients were similarly treated with a cytarabine/anthracycline based induction on frontline Cancer and Leukemia Group B (CALGB)/Alliance for Clinical Trials in Oncology (Alliance) protocols, with details of CALGB treatment protocols provided in the Data S1. No patient included in the analysis received an allogeneic hematopoietic stem-cell transplantation (HSCT) in first complete remission (CR), and patients who underwent an allogeneic HSCT off-study were not included because of incomplete or missing follow-up information. All patients were enrolled on CALGB 8461 (cytogenetic studies), CALGB 9665 (leukemia tissue bank), and CALGB 20202 (molecular studies) companion protocols, with further treatment details provided in the Data S1. The mutational status of 80 total protein-coding genes was determined centrally at The Ohio State University by targeted amplicon sequencing using the MiSeq platform (Illumina)<span><sup>6</sup></span> and further detailed in the Data S1. Analysis of differentially expressed genes within each WBC group was done on peripheral blood samples via total transcriptome RNAseq with subsequent gene set enrichment analyses (GSEA) via Hallmark/Kegg pathways of 40% of our entire cohort. Clinical endpoints were defined according to generally accepted criteria.<span><sup>1</sup></span> Baseline characteristics were compared using the Fisher's exact and Wilcoxon rank-sum tests for categorical and continuous variables, respectively.<span><sup>10</sup></span> Estimated probabilities of DFS and OS were calculated using the Kaplan–Meier method,<span><sup>11</sup></span> and the log-rank test evaluated differences between survival distributions. Multivariable logistic regression models were generated for attainment of CR, and multivariable proportional hazards models were constructed for DFS and OS using a limited backward elimination procedure, with variables significant at α = 0.2 from the univariable analyses considered for multivariable analyses. All analyses were performed by the Alliance Statistics and Data Center on a database locked on June 9, 2020 using SAS 9.4 and TIBCO Spotfire S + 8.2.</p><p>Pretreatment patient characteristics are shown in Table S1. The median age for the three WBC groups (<i>low</i>, <i>intermediate</i>, and <i>high</i>) was similar (46, 44, and 43 years, respectively), and 55% of patients were male. Patients in the <i>high</i> WBC group had the highest extramedullary disease burden at diagnosis followed by patients in the <i>intermediate</i> and <i>low</i> groups (38% vs. 29% and 12%, respectively; <i>p</i> < .001). Patients in the <i>intermediate</i> WBC group more often had core-binding factor AML (CBF-AML; <i>p</i> < .001), that is, harbored inv(16)(p13.1q22)/t(16;16)(p13.1;q22) or t(8;21)(q22;q22)<span><sup>12</sup></span> (Table S2), and the <i>low</i> WBC group patients had complex karyotype more often (<i>p</i> < .001). Patients in the <i>high</i> WBC group presented more frequently with <i>FLT</i>3-ITD than those in the <i>intermediate</i> and, especially, <i>low</i> groups (36% vs. 24% vs. 12%, respectively; <i>p</i> < .001). Among patients with <i>FLT</i>3-ITD, those in the <i>high</i> WBC group had more often high allelic ratio (≥50%) than patients in the <i>intermediate</i> and <i>low</i> groups (30% vs. 17% vs. 5%, respectively; <i>p</i> < .001).</p><p>Patients in the <i>intermediate</i> WBC group had a higher CR rate (<i>p</i> < .001), longer DFS (<i>p</i> = .002; Figure S2), EFS (<i>p</i> < .001; Figure 1A), and OS (<i>p</i> < .001; Figure 1B) than patients in the other two WBC groups (Table S3). <i>Intermediate</i> WBC group patients also had higher CR rates (<i>p</i> = .009; Table S4), longer DFS (<i>p</i> = .01; Table S5), EFS (<i>p</i> < .001; Table S6), and OS (<i>p</i> = .01; Table S7) in multivariable modeling, after adjusting for other variables provided in Tables S4–S7.</p><p>Among patients categorized according to the 2022 ELN classification, those in the Favorable group who had an <i>intermediate</i> WBC had longer EFS (<i>p</i> < .004; Figure 1C) and were associated by trend with a longer DFS (<i>p</i> = .08; Figure S3) and OS (<i>p</i> = .06; Figure S4) than patients with <i>high</i> WBC. WBC group did not affect patient outcome in the 2022 ELN Intermediate or Adverse groups. Within the 2022 ELN Favorable group, <i>intermediate</i> WBC was associated with longer DFS (<i>p</i> = .04), EFS (<i>p</i> = .002), and OS (<i>p</i> = .005) in patients with <i>CEBPA</i><sup>bZIP</sup> mutations or <i>NPM1</i> mutations with no <i>FLT3</i>-ITD, but not in patients with CBF-AML (Figure 1D–F). Our data thus suggest it may be time to rethink the paradigm that all AML patients who present with an elevated WBC at diagnosis have a greater probability of relapse or worsened survival. For example, younger adults with AML classified in <i>high</i> WBC group who harbor genetic alterations assigning them to either 2022 ELN Intermediate or Adverse group do not have worse outcomes than other patients assigned to the same 2022 ELN genetic-risk groups who have <i>low</i> or <i>intermediate</i> WBC levels. In contrast, our data suggest that a more aggressive post-remission treatment is needed for patients categorized in the 2022 ELN Favorable group who belong to either <i>high</i> or <i>low</i> WBC group. This is especially relevant for 2022 ELN Favorable patients who carry <i>CEBPA</i><sup>bZIP</sup> mutations or have <i>NPM1</i> mutations in the absence of <i>FLT3</i>-ITD. Conversely, younger adults with AML and a 2022 ELN Favorable profile belonging to the <i>intermediate</i> WBC group do better than those in the <i>low</i> or <i>high</i> WBC categories. This finding requires further validation and exploration.</p><p>We next analyzed the differences in WBC group-associated gene-expression profiles. Patients in the <i>high</i> WBC group had upregulation of the C-X-C motif chemokine ligand 10 (<i>CXCL10</i>) and hypoxia inducible lipid droplet associated (<i>HILPDA</i>) genes, and downregulation of the fibronectin 1 (<i>FN1</i>) and mesothelin (<i>MSLN</i>) genes compared with the <i>intermediate</i> group (Figure S5A). This suggests a predilection for inflammatory cytokine signaling and upregulation of fat storage and fatty acid metabolism in this group, which also mimicked the GSEA results seen in the <i>high</i> WBC group (Figure S6A). Conversely, <i>MMP7</i> and <i>GZMA</i> were upregulated in the <i>low</i> WBC group compared with the <i>intermediate</i> group (Figure S5B), which may suggest a common catabolic/destructive pathway as also seen in its GSEA with increasing inflammation (i.e., interferon α/γ) (Figure S6B). Importantly, high inflammation risk-score recently emerged as a strong prognosticator of treatment outcome in AML.<span><sup>13</sup></span> While higher inflammation was associated with select molecular features, its prognostic significance was independent from established molecular risk markers.<span><sup>13</sup></span> Our data suggest that the adverse prognostic impact of high WBC may, in part, be mediated by changes in the inflammatory response, thereby supporting exploration of therapies targeting inflammation to mitigate the adverse prognosis.</p><p>Given the clinically relevant sequelae of hyperleukocytosis (HL),<span><sup>14</sup></span> we also analyzed the extreme WBC ranges of our patient cohort with WBC ≥50 000/μL. We observed that patients with a WBC >200 000/μL had OS similar to OS of patients with a WBC between 50 000/μL and 200 000/μL (Figure S1B). Our analysis is limited by a relatively small number of only 30 patients presenting with a WBC >200 000/μL, but this may suggest that the “extreme” ends of HL may be equivalent to the “lower” ends of clinically defined HL. There is currently mixed data concerning best initial management for patients who present with HL regarding leukapheresis compared to more immediate chemotherapy.<span><sup>15-19</sup></span> Currently it is unclear as to how to best manage patients presenting with HL in regard to leukapheresis compared to more immediate chemotherapy. Retrospective data have shown variable outcomes with either approach and there are multiple barriers due to the acuity of these patients in performing a prospective study to better determine selection of initial management. These WBC groups should not be used to determine management for patients with clinical signs or symptoms of leukostasis, but serve as a prognostic tool in conjunction with a physician's clinical expertise to help guide therapy decisions.</p><p>In conclusion, we propose three WBC groups to offer additional prognostic information for younger AML patients. Our study revealed that an <i>intermediate</i> WBC group was associated with better outcomes among all patients, with higher CR rates and longer survival in all calculated metrics (DFS, EFS, OS) in multivariable modeling compared with patients in the <i>low</i> and <i>high</i> WBC groups. Patients in the 2022 ELN Favorable group, especially those with non-CBF-AML, benefited from having <i>intermediate</i> WBC levels at diagnosis. Clear differences in the metabolic pathways exist among WBC groups. These WBC groups offer additional prognostic information for younger AML patients.</p><p>MO, A-KE, ASM, and KM designed the study; MO, DN, KM, JK, CJW, SO, JSB, JCB, ASM, and A-KE analyzed the data; DN and JK performed the statistical analysis; MO, KM, DN, CJW, ASM, and A-KE wrote the manuscript; AJC, KM, RAL, JEK, BLP, RMS, JCB, and ASM were involved directly or indirectly in the care of patients and/or sample procurement. All authors read and agreed upon the final version of the manuscript.</p><p>CJW is a consultant for Vigeo Therapeutics and employed at Karyopharm Therapeutics, and has ownership interest in Karyopharm Therapeutics and Bristol-Myers Squibb Co. JSB is a consultant/advisory board member for AbbVie, AstraZeneca, INNATE, KITE. RAL received research funding from Astellas, Cellectis, Gilead, Novartis, and Rafael Pharmaceuticals; and consults for AbbVie, CVS/Caremark, Epizyme, and Takeda. JEK has received honoraria from Gilead, Magellan, and Novartis; consulting fees from Gilead, Magellan, Novartis, Pharmacyclics, and Seattle Genetics; institutional research funding from Boehringer Ingelheim, Cantex, Erytech, and Millennium; and travel support from Gilead, Novartis, and Seattle Genetics. BLP received honoraria from Jazz Pharmaceuticals, Novartis, and Pfizer. RMS consults for AbbVie, Agios, Aprea, Arog, Boston Pharmaceuticals, Bristol Myers Squibb, Celgene, Foghorn Therapeutics, GlaxoSmithKline, Innate, Janssen, Jazz, Macrogenics, Novartis, Onconova, and Takeda; received research funding from AbbVie, Agios, Arog, and Novartis; and serves on the advisory committee or board of directors for Actinium, Amgen, Astellas, BerGen Bio, Boston Pharmaceuticals, Elevate Bio, Gemoab, Syndax, Syntrix/ACI, and Syros. JCB has a consultancy/advisory role with Syndax, Novartis, Vincera; research funding from Pharmacyclics LLC, an AbbVie Company, Genentech, Janssen, Acerta; ownership for Vincera. A-KE served on the Diversity, Equite, and Inclusion Advisory Boards of AstraZeneca and has a current employment of her spouse at Karyopharm Therapeutics. ASM is a Senior Medical Director for the Leukemia and Lymphoma Society's Beat AML clinical study; serves on the DMSC for Foghorn Therapeutics and has served as a consultant for AbbVie, BMS, Novartis Pharmaceuticals, Treadwell Therapeutics, and Vincerx Pharma. The other authors declare no competing financial interests.</p><p>All patients provided written informed consent for participation in the treatment studies and in companion studies CALGB 8461 (cytogenetic studies), CALGB 9665 (leukemia tissue bank), and CALGB 20202 (molecular studies) before enrollment in accordance with the Declaration of Helsinki.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 11","pages":"2236-2240"},"PeriodicalIF":10.1000,"publicationDate":"2024-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27465","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27465","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Acute myeloid leukemia (AML) is a biologically and clinically heterogenous disease with diverse genetic abnormalities1-6 and a wide-ranging white blood cell counts (WBC) at diagnosis.1 The 2022 European LeukemiaNet (ELN) genetic-risk classification incorporates cytogenetic and selected molecular alterations to define Favorable, Intermediate, and Adverse genetic-risk groups providing valuable prognostic information.1 Pretreatment WBC levels are also a main prognostic factor for patients with AML;7, 8 however, there are no standardized WBC-associated groups that improve prognostication for younger patients. de Jonge et al.9 first investigated the impact of WBC on outcome of AML patients harboring NPM1 mutations and FLT3 internal tandem duplications (FLT3-ITD) that were divided into three WBC groups: <20 000/μL, WBC 20 000/μL–100 000/μL, and ≥100 000/μL. We decided to build upon this previous work by analyzing a larger, clinically and molecularly well-characterized cohort of 1121 younger (aged <60 years) adults with de novo AML to define clinically relevant WBC level groups and determine their potential independent prognostic impact and associations with gene-expression profiles.
We defined three WBC groups: low (<10 000/μL, n = 298 patients), intermediate (10 000–49 999/μL, n = 488), and high (≥50 000/μL, n = 335). These groups were chosen because there was no correlation with an observable steady decrease in any analyzed outcome endpoint, including disease-free (DFS), event-free (EFS), or overall (OS) survival, with WBC increasing above 50 000/μL by 10 000/μL increments, nor were there any linear changes in endpoints associated with WBC decreasing below 10 000/μL in 1000/μL increments across the entire cohort (Figure S1A,B). All patients were similarly treated with a cytarabine/anthracycline based induction on frontline Cancer and Leukemia Group B (CALGB)/Alliance for Clinical Trials in Oncology (Alliance) protocols, with details of CALGB treatment protocols provided in the Data S1. No patient included in the analysis received an allogeneic hematopoietic stem-cell transplantation (HSCT) in first complete remission (CR), and patients who underwent an allogeneic HSCT off-study were not included because of incomplete or missing follow-up information. All patients were enrolled on CALGB 8461 (cytogenetic studies), CALGB 9665 (leukemia tissue bank), and CALGB 20202 (molecular studies) companion protocols, with further treatment details provided in the Data S1. The mutational status of 80 total protein-coding genes was determined centrally at The Ohio State University by targeted amplicon sequencing using the MiSeq platform (Illumina)6 and further detailed in the Data S1. Analysis of differentially expressed genes within each WBC group was done on peripheral blood samples via total transcriptome RNAseq with subsequent gene set enrichment analyses (GSEA) via Hallmark/Kegg pathways of 40% of our entire cohort. Clinical endpoints were defined according to generally accepted criteria.1 Baseline characteristics were compared using the Fisher's exact and Wilcoxon rank-sum tests for categorical and continuous variables, respectively.10 Estimated probabilities of DFS and OS were calculated using the Kaplan–Meier method,11 and the log-rank test evaluated differences between survival distributions. Multivariable logistic regression models were generated for attainment of CR, and multivariable proportional hazards models were constructed for DFS and OS using a limited backward elimination procedure, with variables significant at α = 0.2 from the univariable analyses considered for multivariable analyses. All analyses were performed by the Alliance Statistics and Data Center on a database locked on June 9, 2020 using SAS 9.4 and TIBCO Spotfire S + 8.2.
Pretreatment patient characteristics are shown in Table S1. The median age for the three WBC groups (low, intermediate, and high) was similar (46, 44, and 43 years, respectively), and 55% of patients were male. Patients in the high WBC group had the highest extramedullary disease burden at diagnosis followed by patients in the intermediate and low groups (38% vs. 29% and 12%, respectively; p < .001). Patients in the intermediate WBC group more often had core-binding factor AML (CBF-AML; p < .001), that is, harbored inv(16)(p13.1q22)/t(16;16)(p13.1;q22) or t(8;21)(q22;q22)12 (Table S2), and the low WBC group patients had complex karyotype more often (p < .001). Patients in the high WBC group presented more frequently with FLT3-ITD than those in the intermediate and, especially, low groups (36% vs. 24% vs. 12%, respectively; p < .001). Among patients with FLT3-ITD, those in the high WBC group had more often high allelic ratio (≥50%) than patients in the intermediate and low groups (30% vs. 17% vs. 5%, respectively; p < .001).
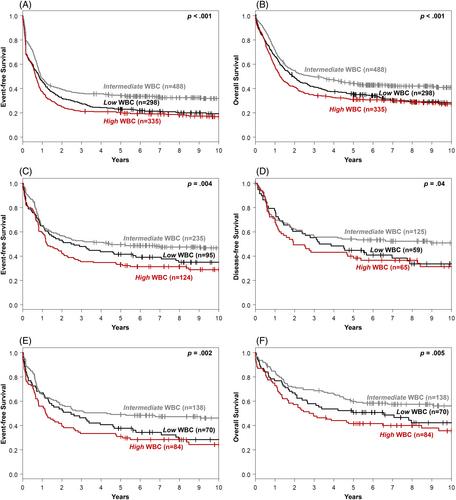
Patients in the intermediate WBC group had a higher CR rate (p < .001), longer DFS (p = .002; Figure S2), EFS (p < .001; Figure 1A), and OS (p < .001; Figure 1B) than patients in the other two WBC groups (Table S3). Intermediate WBC group patients also had higher CR rates (p = .009; Table S4), longer DFS (p = .01; Table S5), EFS (p < .001; Table S6), and OS (p = .01; Table S7) in multivariable modeling, after adjusting for other variables provided in Tables S4–S7.
Among patients categorized according to the 2022 ELN classification, those in the Favorable group who had an intermediate WBC had longer EFS (p < .004; Figure 1C) and were associated by trend with a longer DFS (p = .08; Figure S3) and OS (p = .06; Figure S4) than patients with high WBC. WBC group did not affect patient outcome in the 2022 ELN Intermediate or Adverse groups. Within the 2022 ELN Favorable group, intermediate WBC was associated with longer DFS (p = .04), EFS (p = .002), and OS (p = .005) in patients with CEBPAbZIP mutations or NPM1 mutations with no FLT3-ITD, but not in patients with CBF-AML (Figure 1D–F). Our data thus suggest it may be time to rethink the paradigm that all AML patients who present with an elevated WBC at diagnosis have a greater probability of relapse or worsened survival. For example, younger adults with AML classified in high WBC group who harbor genetic alterations assigning them to either 2022 ELN Intermediate or Adverse group do not have worse outcomes than other patients assigned to the same 2022 ELN genetic-risk groups who have low or intermediate WBC levels. In contrast, our data suggest that a more aggressive post-remission treatment is needed for patients categorized in the 2022 ELN Favorable group who belong to either high or low WBC group. This is especially relevant for 2022 ELN Favorable patients who carry CEBPAbZIP mutations or have NPM1 mutations in the absence of FLT3-ITD. Conversely, younger adults with AML and a 2022 ELN Favorable profile belonging to the intermediate WBC group do better than those in the low or high WBC categories. This finding requires further validation and exploration.
We next analyzed the differences in WBC group-associated gene-expression profiles. Patients in the high WBC group had upregulation of the C-X-C motif chemokine ligand 10 (CXCL10) and hypoxia inducible lipid droplet associated (HILPDA) genes, and downregulation of the fibronectin 1 (FN1) and mesothelin (MSLN) genes compared with the intermediate group (Figure S5A). This suggests a predilection for inflammatory cytokine signaling and upregulation of fat storage and fatty acid metabolism in this group, which also mimicked the GSEA results seen in the high WBC group (Figure S6A). Conversely, MMP7 and GZMA were upregulated in the low WBC group compared with the intermediate group (Figure S5B), which may suggest a common catabolic/destructive pathway as also seen in its GSEA with increasing inflammation (i.e., interferon α/γ) (Figure S6B). Importantly, high inflammation risk-score recently emerged as a strong prognosticator of treatment outcome in AML.13 While higher inflammation was associated with select molecular features, its prognostic significance was independent from established molecular risk markers.13 Our data suggest that the adverse prognostic impact of high WBC may, in part, be mediated by changes in the inflammatory response, thereby supporting exploration of therapies targeting inflammation to mitigate the adverse prognosis.
Given the clinically relevant sequelae of hyperleukocytosis (HL),14 we also analyzed the extreme WBC ranges of our patient cohort with WBC ≥50 000/μL. We observed that patients with a WBC >200 000/μL had OS similar to OS of patients with a WBC between 50 000/μL and 200 000/μL (Figure S1B). Our analysis is limited by a relatively small number of only 30 patients presenting with a WBC >200 000/μL, but this may suggest that the “extreme” ends of HL may be equivalent to the “lower” ends of clinically defined HL. There is currently mixed data concerning best initial management for patients who present with HL regarding leukapheresis compared to more immediate chemotherapy.15-19 Currently it is unclear as to how to best manage patients presenting with HL in regard to leukapheresis compared to more immediate chemotherapy. Retrospective data have shown variable outcomes with either approach and there are multiple barriers due to the acuity of these patients in performing a prospective study to better determine selection of initial management. These WBC groups should not be used to determine management for patients with clinical signs or symptoms of leukostasis, but serve as a prognostic tool in conjunction with a physician's clinical expertise to help guide therapy decisions.
In conclusion, we propose three WBC groups to offer additional prognostic information for younger AML patients. Our study revealed that an intermediate WBC group was associated with better outcomes among all patients, with higher CR rates and longer survival in all calculated metrics (DFS, EFS, OS) in multivariable modeling compared with patients in the low and high WBC groups. Patients in the 2022 ELN Favorable group, especially those with non-CBF-AML, benefited from having intermediate WBC levels at diagnosis. Clear differences in the metabolic pathways exist among WBC groups. These WBC groups offer additional prognostic information for younger AML patients.
MO, A-KE, ASM, and KM designed the study; MO, DN, KM, JK, CJW, SO, JSB, JCB, ASM, and A-KE analyzed the data; DN and JK performed the statistical analysis; MO, KM, DN, CJW, ASM, and A-KE wrote the manuscript; AJC, KM, RAL, JEK, BLP, RMS, JCB, and ASM were involved directly or indirectly in the care of patients and/or sample procurement. All authors read and agreed upon the final version of the manuscript.
CJW is a consultant for Vigeo Therapeutics and employed at Karyopharm Therapeutics, and has ownership interest in Karyopharm Therapeutics and Bristol-Myers Squibb Co. JSB is a consultant/advisory board member for AbbVie, AstraZeneca, INNATE, KITE. RAL received research funding from Astellas, Cellectis, Gilead, Novartis, and Rafael Pharmaceuticals; and consults for AbbVie, CVS/Caremark, Epizyme, and Takeda. JEK has received honoraria from Gilead, Magellan, and Novartis; consulting fees from Gilead, Magellan, Novartis, Pharmacyclics, and Seattle Genetics; institutional research funding from Boehringer Ingelheim, Cantex, Erytech, and Millennium; and travel support from Gilead, Novartis, and Seattle Genetics. BLP received honoraria from Jazz Pharmaceuticals, Novartis, and Pfizer. RMS consults for AbbVie, Agios, Aprea, Arog, Boston Pharmaceuticals, Bristol Myers Squibb, Celgene, Foghorn Therapeutics, GlaxoSmithKline, Innate, Janssen, Jazz, Macrogenics, Novartis, Onconova, and Takeda; received research funding from AbbVie, Agios, Arog, and Novartis; and serves on the advisory committee or board of directors for Actinium, Amgen, Astellas, BerGen Bio, Boston Pharmaceuticals, Elevate Bio, Gemoab, Syndax, Syntrix/ACI, and Syros. JCB has a consultancy/advisory role with Syndax, Novartis, Vincera; research funding from Pharmacyclics LLC, an AbbVie Company, Genentech, Janssen, Acerta; ownership for Vincera. A-KE served on the Diversity, Equite, and Inclusion Advisory Boards of AstraZeneca and has a current employment of her spouse at Karyopharm Therapeutics. ASM is a Senior Medical Director for the Leukemia and Lymphoma Society's Beat AML clinical study; serves on the DMSC for Foghorn Therapeutics and has served as a consultant for AbbVie, BMS, Novartis Pharmaceuticals, Treadwell Therapeutics, and Vincerx Pharma. The other authors declare no competing financial interests.
All patients provided written informed consent for participation in the treatment studies and in companion studies CALGB 8461 (cytogenetic studies), CALGB 9665 (leukemia tissue bank), and CALGB 20202 (molecular studies) before enrollment in accordance with the Declaration of Helsinki.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


