{"title":"Sustainability","authors":"","doi":"10.1111/jgh.16709","DOIUrl":null,"url":null,"abstract":"<p><b>65</b></p><p><b>Using patient satisfaction scores to compare performance of nurse practitioner against doctors in direct access endoscopy clinic</b></p><p>David Huynh, Aathavan Shanmuga Anandan, Ruth Ayers and Peter Hendy</p><p><i>Mater Hospital Brisbane, Brisbane, Australia</i></p><p><i><b>Background and Aim</b>:</i> Physician shortages contribute to the growing presence of nurse practitioners (NP), driven by the expectation that NP can reduce outpatient wait times, leading to better patient outcomes. While Direct Assessment Endoscopy (DAE) aims to streamline access for simple cases, it still requires doctor involvement for consent and assessment. An NP-led care model presents an alternative, but concerns exist anecdotally about patient acceptance. We seek to assess patient expectations and acceptance of a newly introduced NP-led DAE clinic at Mater Health Brisbane (MHB).</p><p><b><i>Methods:</i></b> Patients attending DAE clinics at the MHB were surveyed across two months. Patients completed two survey sections: a pre- and post-consultation questionnaire using a 5-point Likert scale. The pre-consultation questions were set to determine if the patients had pre-conceived biases such as “expecting to see a doctor”. Post-consultation questions assessed ‘communication’, ‘experience’, ‘professionalism’, and ‘understanding’ of endoscopic procedures. Patients were blinded to whether they would see an NP or doctor for their endoscopic consultation. Scores were collated to compare NP against doctors.</p><p><i><b>Results</b>:</i> 92 patients offered to participate in the survey with 71 (77%) patients completing questionnaires. 33 (46%) patients saw a doctor, and 38 saw an NP (54%). NP ratings were significantly higher than doctors regarding ‘professionalism and friendliness’ (see table 1). NP scores were numerically greater than doctors in ‘overall experience’, ‘understanding’, and ‘communication’. Of the total 71 patients, 61 had anticipated seeing a doctor. Of these 61 patients, 51% encountered an NP instead (n = 31). Of these 31 patients, 28 expressed no reservations about seeing either an NP or a doctor following the consultation. The average scores for doctors (Group A) regarding overall experience, professionalism, understanding, and communication were 4.0 (95% CI [3.5–4.5]), 4.2 (95% CI [3.8–4.7]), 4.5 (95% CI [4.3–4.7], and 4.5 (95% CI [4.3–4.7]), respectively. Conversely, patients with preconceived biases determined by all the patients wanting to see a doctor (Group B) reported average scores of 4.3 (95% CI [3.9–4.7]), 4.7 (95% CI [4.5–4.9]), 4.5 (95% CI [4.5–4.6]), and 4.5 (95% CI [4.4–4.8]) for the same attributes, respectively.</p><p><b><i>Conclusion:</i></b> Overall, NP results proved non-significantly higher in all metrics than doctors except ‘professionalism and friendliness’. We also showed that pre-existing biases did not significantly influence patients' overall experiences with NPs. This suggests that the integration of an NP into our new DAE clinic is well accepted and comparable to doctor-led consultation.</p><p><b>282</b></p><p><b>The use of Millipore strip biopsy saves costs: Experience from a New Zealand tertiary centre</b></p><p><b>Laura Hollingsworth</b>, Jan Kubovy, Malcolm Arnold and Kelly Jones</p><p><i>Christchurch Hospital, Christchurch, New Zealand</i></p><p><b><i>Background and Aim:</i></b> The demand for gastrointestinal (GI) endoscopy has significantly increased worldwide over the last decade along with associated waste. Millipore strips (MPS) enable biopsy specimens from different areas of the GI tract to be placed in one pottle and aligned on a strip according to specific sites (Fig. 1,2). This reduces the number of pottles and saves on lab time showing great promise in terms of cost savings and carbon foot print. The use of MPS has been successfully used in a number of countries. The technique was first introduced and validated at our centre in 2009. We aimed to review the use of MPS over the last two years at our centre and to determine the current cost saving. This was compared to the initial cost saving analysis proposed in 2009. Secondly, we reviewed current MPS utilisation across our department.</p><p><b><i>Methods:</i></b> A retrospective review of all endoscopic biopsies performed at our centre between July 2021 to June 2023 was conducted. Data were obtained from Delphic Sysmex pathology processing system. Cost analysis was based on the following figures to process samples histologically (excluding GST): Millipore strip $NZ 102.36 (average 4–6 biopsies per strip). Standard biopsy $NZ 69.74 (costs including lab time).</p><p><b><i>Results:</i></b> A total of 12,288 endoscopies which included biopsies were performed in our endoscopy unit over the two-year period generating a total of 24,659 specimen pottles. Of these, 9.8% (1205) used MPS, averaging one MPS per procedure. In comparison 90.2% (11083) used standard biopsy collection alone with an average of 6.7 pottles per procedure. The calculated cost saving excluding GST was $NZ 109,404 per annum (conservative estimate based on 4 histologic samples per MPS). The cost saving estimate in 2009 was $NZ 135,200 per annum assuming every eligible endoscopy case would be utilised. MPS use in our department ranged from 0 to 97 per endoscopist per annum.</p><p><i><b>Conclusion</b>:</i> MPS use brings significant cost savings despite imperfect uptake. Improved awareness could yield even more impressive results.</p><p><b>553</b></p><p><b>Introduction of a sustainable model to reduce the environmental impact of endoscopy at a tertiary Australian centre</b></p><p><b>Hasib Ahmadzai</b><sup>1</sup>, Emily Lau<sup>1</sup>, Karamea Tumata<sup>1</sup>, Kyoungia Roh<sup>1</sup>, Mohammad Kharbat<sup>1</sup> and Philip Craig<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, St George Hospital, Kogarah, Australia;</i> <sup>2</sup><i>Faculty of Medicine, University of New South Wales, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic procedures play a critical role in the diagnosis and management of gastrointestinal and respiratory disorders. These procedures however, are a major source of waste production, impacting the environment. Environmentally sustainable models including waste segregation may reduce landfill and biohazard waste production while capturing recyclable products. Currently endoscopic waste is segregated only into general landfill or biohazard (clinical), which requires incineration with immediate CO<sub>2</sub> production. This study aimed to document the amount and type of waste reduction that could be achieved through the implementation of a “green” sustainable model in a tertiary endoscopy unit.</p><p><b><i>Methods:</i></b> We performed a prospective study in our Endoscopy unit to calculate the mass (kg) of landfill waste, biohazard waste and linen used over sequential four-week periods. During the <i>baseline</i> period all endoscopy staff underwent training sessions focussed on introduction of environmentally sustainable methods to minimise waste. The mass of waste categories: landfill, biohazard, reusable (soft and hard plastics, paper) and linen was then re-measured over the second <i>green</i> four-week period.</p><p><b><i>Results:</i></b> 1347 endoscopic procedures were performed during the two-month study. During the <i>baseline</i> period 1072.1 kg of waste was generated during 643 procedures and during the <i>green</i> period 1096.4 kg of waste during 704 procedures. Captured recyclable materials during the <i>green</i> period included 26.7 kg soft plastics, 37.8 kg paper and 84.6 kg hard plastics. 13.6% of total waste generated was deemed recyclable. There was a significant reduction in the daily landfill waste generated during the <i>green</i> period with daily median 35.1 kg (<i>baseline)</i> vs 28.9 kg (<i>green)</i> (<i>P</i> = 0.044). Overall non-recyclable median waste was 1.64 kg/procedure during <i>baseline</i> compared to 1.37 kg/procedure during the <i>green</i> period (<i>P</i> = 0.011). Median baseline landfill waste measured 1.12 kg/procedure compared to 0.89 kg/procedure in the green period (<i>P</i> = 0.014). The reduction of landfill waste alone over four weeks contributed to an estimated 521.5 kg CO<sub>2</sub> equivalents in CO<sub>2</sub> emissions, which is similar to the greenhouse gases emitted by an average petrol-powered car driven 2,136 km; or the CO<sub>2</sub> emissions from 261 kg of burnt coal.</p><p><b><i>Conclusion:</i></b> To our knowledge, this is the first Australian study to confirm that implementation of an environmentally sustainable approach in the endoscopy unit leads to: 1) significant reduction in the amount of landfill waste; 2) over 13% of generated waste may be recycled; 3) wider utilisation of similar models in endoscopy units and other hospital departments would lead to reduction in environmental impacts with reduced CO<sub>2</sub> emissions.</p><p>Types of waste generated per procedure during the baseline and green study periods\n\n </p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":null,"pages":null},"PeriodicalIF":3.7000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16709","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16709","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
65
Using patient satisfaction scores to compare performance of nurse practitioner against doctors in direct access endoscopy clinic
David Huynh, Aathavan Shanmuga Anandan, Ruth Ayers and Peter Hendy
Mater Hospital Brisbane, Brisbane, Australia
Background and Aim: Physician shortages contribute to the growing presence of nurse practitioners (NP), driven by the expectation that NP can reduce outpatient wait times, leading to better patient outcomes. While Direct Assessment Endoscopy (DAE) aims to streamline access for simple cases, it still requires doctor involvement for consent and assessment. An NP-led care model presents an alternative, but concerns exist anecdotally about patient acceptance. We seek to assess patient expectations and acceptance of a newly introduced NP-led DAE clinic at Mater Health Brisbane (MHB).
Methods: Patients attending DAE clinics at the MHB were surveyed across two months. Patients completed two survey sections: a pre- and post-consultation questionnaire using a 5-point Likert scale. The pre-consultation questions were set to determine if the patients had pre-conceived biases such as “expecting to see a doctor”. Post-consultation questions assessed ‘communication’, ‘experience’, ‘professionalism’, and ‘understanding’ of endoscopic procedures. Patients were blinded to whether they would see an NP or doctor for their endoscopic consultation. Scores were collated to compare NP against doctors.
Results: 92 patients offered to participate in the survey with 71 (77%) patients completing questionnaires. 33 (46%) patients saw a doctor, and 38 saw an NP (54%). NP ratings were significantly higher than doctors regarding ‘professionalism and friendliness’ (see table 1). NP scores were numerically greater than doctors in ‘overall experience’, ‘understanding’, and ‘communication’. Of the total 71 patients, 61 had anticipated seeing a doctor. Of these 61 patients, 51% encountered an NP instead (n = 31). Of these 31 patients, 28 expressed no reservations about seeing either an NP or a doctor following the consultation. The average scores for doctors (Group A) regarding overall experience, professionalism, understanding, and communication were 4.0 (95% CI [3.5–4.5]), 4.2 (95% CI [3.8–4.7]), 4.5 (95% CI [4.3–4.7], and 4.5 (95% CI [4.3–4.7]), respectively. Conversely, patients with preconceived biases determined by all the patients wanting to see a doctor (Group B) reported average scores of 4.3 (95% CI [3.9–4.7]), 4.7 (95% CI [4.5–4.9]), 4.5 (95% CI [4.5–4.6]), and 4.5 (95% CI [4.4–4.8]) for the same attributes, respectively.
Conclusion: Overall, NP results proved non-significantly higher in all metrics than doctors except ‘professionalism and friendliness’. We also showed that pre-existing biases did not significantly influence patients' overall experiences with NPs. This suggests that the integration of an NP into our new DAE clinic is well accepted and comparable to doctor-led consultation.
282
The use of Millipore strip biopsy saves costs: Experience from a New Zealand tertiary centre
Laura Hollingsworth, Jan Kubovy, Malcolm Arnold and Kelly Jones
Christchurch Hospital, Christchurch, New Zealand
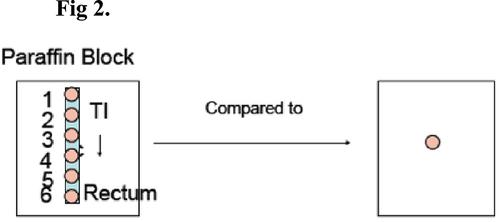
Background and Aim: The demand for gastrointestinal (GI) endoscopy has significantly increased worldwide over the last decade along with associated waste. Millipore strips (MPS) enable biopsy specimens from different areas of the GI tract to be placed in one pottle and aligned on a strip according to specific sites (Fig. 1,2). This reduces the number of pottles and saves on lab time showing great promise in terms of cost savings and carbon foot print. The use of MPS has been successfully used in a number of countries. The technique was first introduced and validated at our centre in 2009. We aimed to review the use of MPS over the last two years at our centre and to determine the current cost saving. This was compared to the initial cost saving analysis proposed in 2009. Secondly, we reviewed current MPS utilisation across our department.
Methods: A retrospective review of all endoscopic biopsies performed at our centre between July 2021 to June 2023 was conducted. Data were obtained from Delphic Sysmex pathology processing system. Cost analysis was based on the following figures to process samples histologically (excluding GST): Millipore strip $NZ 102.36 (average 4–6 biopsies per strip). Standard biopsy $NZ 69.74 (costs including lab time).
Results: A total of 12,288 endoscopies which included biopsies were performed in our endoscopy unit over the two-year period generating a total of 24,659 specimen pottles. Of these, 9.8% (1205) used MPS, averaging one MPS per procedure. In comparison 90.2% (11083) used standard biopsy collection alone with an average of 6.7 pottles per procedure. The calculated cost saving excluding GST was $NZ 109,404 per annum (conservative estimate based on 4 histologic samples per MPS). The cost saving estimate in 2009 was $NZ 135,200 per annum assuming every eligible endoscopy case would be utilised. MPS use in our department ranged from 0 to 97 per endoscopist per annum.
Conclusion: MPS use brings significant cost savings despite imperfect uptake. Improved awareness could yield even more impressive results.
553
Introduction of a sustainable model to reduce the environmental impact of endoscopy at a tertiary Australian centre
Hasib Ahmadzai1, Emily Lau1, Karamea Tumata1, Kyoungia Roh1, Mohammad Kharbat1 and Philip Craig1,2
1Department of Gastroenterology and Hepatology, St George Hospital, Kogarah, Australia;2Faculty of Medicine, University of New South Wales, Sydney, Australia
Background and Aim: Endoscopic procedures play a critical role in the diagnosis and management of gastrointestinal and respiratory disorders. These procedures however, are a major source of waste production, impacting the environment. Environmentally sustainable models including waste segregation may reduce landfill and biohazard waste production while capturing recyclable products. Currently endoscopic waste is segregated only into general landfill or biohazard (clinical), which requires incineration with immediate CO2 production. This study aimed to document the amount and type of waste reduction that could be achieved through the implementation of a “green” sustainable model in a tertiary endoscopy unit.
Methods: We performed a prospective study in our Endoscopy unit to calculate the mass (kg) of landfill waste, biohazard waste and linen used over sequential four-week periods. During the baseline period all endoscopy staff underwent training sessions focussed on introduction of environmentally sustainable methods to minimise waste. The mass of waste categories: landfill, biohazard, reusable (soft and hard plastics, paper) and linen was then re-measured over the second green four-week period.
Results: 1347 endoscopic procedures were performed during the two-month study. During the baseline period 1072.1 kg of waste was generated during 643 procedures and during the green period 1096.4 kg of waste during 704 procedures. Captured recyclable materials during the green period included 26.7 kg soft plastics, 37.8 kg paper and 84.6 kg hard plastics. 13.6% of total waste generated was deemed recyclable. There was a significant reduction in the daily landfill waste generated during the green period with daily median 35.1 kg (baseline) vs 28.9 kg (green) (P = 0.044). Overall non-recyclable median waste was 1.64 kg/procedure during baseline compared to 1.37 kg/procedure during the green period (P = 0.011). Median baseline landfill waste measured 1.12 kg/procedure compared to 0.89 kg/procedure in the green period (P = 0.014). The reduction of landfill waste alone over four weeks contributed to an estimated 521.5 kg CO2 equivalents in CO2 emissions, which is similar to the greenhouse gases emitted by an average petrol-powered car driven 2,136 km; or the CO2 emissions from 261 kg of burnt coal.
Conclusion: To our knowledge, this is the first Australian study to confirm that implementation of an environmentally sustainable approach in the endoscopy unit leads to: 1) significant reduction in the amount of landfill waste; 2) over 13% of generated waste may be recycled; 3) wider utilisation of similar models in endoscopy units and other hospital departments would lead to reduction in environmental impacts with reduced CO2 emissions.
Types of waste generated per procedure during the baseline and green study periods
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


