{"title":"Advanced Endoscopic Techniques","authors":"","doi":"10.1111/jgh.16696","DOIUrl":null,"url":null,"abstract":"<p><b>16</b></p><p><b>Early experience with endoscopic submucosal dissection at Austin Health</b></p><p><b>Sitong Chen</b><sup>1</sup>, Sujievvan Chandran<sup>1,2,3</sup>, Leonardo Zorron Cheng Tao Pu<sup>2,3</sup>, Nicholas Dalkie<sup>3</sup>, Rhys Vaughan<sup>1,2,3</sup> and Marios Efthymiou<sup>1,2,3</sup></p><p><sup>1</sup><i>Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Parkville, Australia;</i> <sup>2</sup><i>Liver Transplant Unit, Austin Health, Heidelberg, Australia;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, Austin Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic submucosal dissection (ESD) is a minimally invasive endoscopic procedure which employs en-bloc dissection technique to remove premalignant or early malignant gastrointestinal lesions. In Japan, ESD is considered as first line treatment for early gastrointestinal neoplasms, yet the wide adoption of ESD in the West has been slow. Barriers include the technical difficulty of ESD, lower prevalence of early gastric cancer in the West, and the lack of training opportunities. We know that gastric location is the easiest location to start training in ESD whereas colorectal ESD is more challenging. The aim of this study was to assess the early experience with ESD at Austin Health.</p><p><b><i>Methods:</i></b> A retrospective analysis was conducted on 31 consecutive gastrointestinal lesions in 27 patients who underwent ESD from June 2020 to April 2023 at Austin Health, Melbourne Australia. Clinical and procedural data, complications, and the efficacy and efficiency of the ESD procedure were evaluated.</p><p><b><i>Results:</i></b> Twenty-seven patients (12 females and 15 males) were enrolled in the study, with a mean age of 72.0 years. Overall, thirty-one lesions were resected, including 16 gastric lesions, 6 oesophageal lesions and 9 colorectal lesions. The mean size of the lesions was 35.8mm and the mean resected base area was 12.0cm<sup>2</sup>. In the total cohort, en-bloc resection rate was 96.8%. Final ESD histology upstaged the initial diagnosis in four lesions based on pre-ESD pinch biopsies and imaging. Eleven malignant lesions were found in the final pathology. Six complications were reported in our study, including two cases of intraoperative perforation and four cases of delayed bleeding (all the complications were managed medically/endoscopically). The mean hospital stay was 1.6 days for all patients, and 19 patients were discharged after an overnight admission.</p><p><b><i>Conclusion:</i></b> ESD is an effective and safe treatment for gastrointestinal neoplasms in an Australian tertiary centre and our early treatment outcomes were comparable to recently published large study data. Outcomes are likely to progressively improve with further experience.</p><p><b>30</b></p><p><b>Intrathoracic cholecystitis managed with endoscopic gallbladder drainage</b></p><p><b>Andrea Huang</b><sup>1,4</sup>, Thomas Williams<sup>1,4</sup>, Nivene Saad<sup>2,4</sup>, Adam Frankel<sup>3,4</sup>, Zaki Hamarneh<sup>1</sup>, Shwan Karim<sup>1</sup> and Adrian Maher<sup>1,4</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>2</sup><i>Department of Radiology, Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>3</sup><i>Department of Upper Gastrointestinal Surgery, Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>4</sup><i>Faculty of Medicine, University of Queensland, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Intrathoracic acute cholecystitis is a presentation that typically occurs in the context of a prior history of a traumatic diaphragmatic hernia. Cholecystectomy and hernia repair has been the mainstay of management in previous case reports, either via open surgical, laparoscopic or thoracoscopic techniques. However not all patients may be suitable for major operations and alternative management options, such as endoscopic ultrasound-guided approaches, are required.</p><p><b><i>Case Report:</i></b> This case report describes that of a 67 year old female who presented with intrathoracic acute cholecystitis complicated by a type 1 myocardial infarction. In the months prior, she had received neoadjuvant chemotherapy and immunotherapy for a poorly-differentiated gastro-oesophageal adenocarcinoma and was awaiting re-evaluation for surgical resection. Her staging scans had demonstrated a large diaphragmatic hernia presumed secondary to a car crash in her youth. The hernia contained the right lobe of the liver, hepatic flexure, first and secondary part of the duodenum, and the gallbladder. Initial management of the intrathoracic acute cholecystitis with antibiotics was unsuccessful. Supine laparoscopy with both abdominal and right thoracic ports was attempted, however the gallbladder could not be visualized. Given her recent medical issues, major open surgery was avoided. Endoscopic ultrasound-guided internal drainage of the gallbladder was successfully achieved using a 10mm x 10mm lumen apposing metal stent, with visible passage of stones and resolution of cholecystitis.</p><p><b>57</b></p><p><b>Endoscopic ultrasound-guided tissue acquisition with rapid on-site evaluation for the evaluation of solid pancreatic lesions: A retrospective observational study at a tertiary level Australian Hospital</b></p><p><b>Josh McCarthy</b>, Stephen Philcox and Donna Gillies</p><p><i>John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Background</i></b>: Pancreatic cancer is common and associated with a high mortality. The preoperative diagnosis of solid pancreatic lesions can be challenging however EUS-guided tissue acquisition offers a minimally invasive and accurate diagnostic procedure that has been established at our institution since 2010.</p><p><b><i>Aim</i></b>: The objective of this study is to review the diagnostic accuracy of EUS-guided tissue acquisition of solid pancreatic lesions at our institution and to report associations with inaccurate results.</p><p><b><i>Method</i></b>: We performed a retrospective review of EUS-guided biopsies performed from 1/1/2019 - 31/8/2023 to investigate solid pancreatic lesions at a tertiary centre. Data was obtained from the endoscopy database and the electronic medical record. The final diagnosis was based upon surgical resection histopathology or if non-resected, clinical follow-up at least 6 months following the EUS-guided biopsy.</p><p><b><i>Results</i></b>: 80 patients were included in this review. The correct diagnosis was obtained in 75 of 80 patients, equivalent to a diagnostic accuracy of 93.75% (95% CI, 86%-97.9%). Over the study period, there was increased utilization of the Acquire (Boston Scientific) biopsy needle, although this needle did not outperform the other needles. There was no association with diagnostic accuracy and location of the pancreatic mass. There were 3 minor complications reported from the 80 procedures.</p><p><b><i>Conclusion</i>:</b> EUS-guided tissue acquisition to investigate solid pancreatic lesions at our institution has high diagnostic accuracy and is a safe procedure.</p><p><b>77</b></p><p><b>Colonic full thickness resection device: Single-centre experience</b></p><p><b>Vicki McGarrigle</b>, Leonardo Zorron Cheng Tao Pu, Rhys Vaughan, Marios Efthymiou and Sujievvan Chandran</p><p><i>Austin Health, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Endoscopic full-thickness resection (eFTR) using a Full Thickness Resection Device (FTRD) is an emerging technique for resecting difficult colorectal lesions and early colorectal cancers. This method potentially reduces the risk of polyp recurrence and may avoid invasive surgery. Data on its use and outcomes in Australia are limited.</p><p><b><i>Methods:</i></b> Participants were selected from Austin Health’s FTRD database, including all patients who underwent colorectal FTRD. Data collected included patient demographics, lesion size, technical success, resection rates, and complications. Statistical analysis was performed using IBM SPSS.</p><p><b><i>Results:</i></b> A total of 23 patients were included (mean age 65, 70% males). Technical success was 91%, with complete histological resection (R0) in 96%. Delayed complications occurred in 17% of cases, with 75% due to bleeding and 25% due to appendicitis. The mean procedure time was 44 minutes. Difficult positioning was associated with delayed complications (75% vs. 5.6%, p=0.021). Delayed bleeding occurred in 67% of diverticular associated lesions compared to 5% for other FTRD indications (p=0.02). Delayed bleeding was also more common in difficult positions (60% vs. 0%, p=0.006). No significant associations were found between variables and R0, although large effect sizes were noted between procedure time and delayed complications (-1.1)</p><p><b><i>Discussion:</i></b> In this small study, FTRD appears to be effective for the resection of complex colorectal lesions. This study highlights important predictive factors for FTRD complications. Understanding these factors is crucial for improving outcomes and patient care. We plan to gain further insight with a multi-centre FTRD study across Australia and New Zealand.</p><p><b>105</b></p><p><b>Are improvements in biochemical and radiological markers following endoscopic drainage of walled off necrosis associated with reduced need for reintervention and survival?</b></p><p><b>Matthew Bartlett</b><sup>1</sup>, Jade Frank<sup>2</sup>, John Leeds<sup>3</sup>, Kofi Oppong<sup>3</sup>, Sanjay Pandanaboyana<sup>3</sup> and Manu Nayar<sup>3</sup></p><p><sup>1</sup><i>Sir Charles Gairdner Hospital, Perth, Australia;</i> <sup>2</sup><i>Prince Charles Hospital, Brisbane, Australia;</i> <sup>3</sup><i>Freeman Hospital, Newcastle Upon Tyne, United Kingdom</i></p><p><b><i>Background and Aim:</i></b> Endoscopic step-up approach for walled off necrosis (WON) following acute pancreatitis involves EUS guided insertion of lumen apposing metal stents (LAMS) and is now the standard of care. Treatment response varies, many patients will require further intervention via direct endoscopic necrosectomy to aid resolution of WON. Small studies have identified biochemical factors associated with need for repeat re-intervention including duration of elevated c-reactive protein (CRP). This study aimed to evaluate whether biochemical and radiological improvements following LAMS insertion are associated with fewer reinterventions and survival.</p><p><b><i>Methods:</i></b> Patients were identified from an acute pancreatitis regional remote care pathway. Patients with WON who underwent endoscopic drainage between 2018 and 2023 were included. Retrospective data on baseline characteristics, pancreatitis characteristics, and number of endoscopic necrosectomies following LAMS insertion was collected. CRP and white cell count (WCC) around the LAMS insertion were investigated. Improvement was defined as >5% reduction within 48 hours following insertion. CT scan reports within 7 days of LAMS insertion were collected, improvement was defined as a report commenting on improvement in the collection with no other adverse changes. The outcomes assessed were need for necrosectomy following LAMS insertion, and death during admission. Differences in these outcomes was evaluated based on CRP, WCC and radiological responses.</p><p><b><i>Results:</i></b> 97 patients were identified. 42 patients had reduction of CRP >5%, 41 patients had reduction of WCC >5% following LAMS insertion. Requirement for necrosectomy was not significantly different in those with and without CRP reduction, 35 (83%) vs 50 (91%) (OR 0.50, <i>p</i>=0.21); or in those with and without WCC reduction, 33 (80%) vs 52 (93%) (OR 0.32, p=0.07). Inpatient deaths were not significantly different in those with and without a CRP reduction, 2 (5%) vs 9 (16%) (OR 0.25, <i>p</i>=0.07); or in those with and without WCC reduction, 5 (12%) vs 6 (11%) (OR 1.17, <i>p</i>=0.82). Radiological improvement following LAMS insertion was present in 53 patients. Requirement for necrosectomy was not significantly different in those with and without radiological evidence of improvement, 45 (85%) vs 40 (91%%) (OR 0.56, <i>p</i>=0.37). Inpatient deaths were not significantly different between patients with or without radiological improvement 7 (13%) vs 4 (9%) (OR 1.5, <i>p</i>=0.52).</p><p><b><i>Conclusion</i></b>: CRP, WCC and radiological improvements following insertion of LAMS are not associated with fewer reinterventions or reduced risk of death. Further investigation of factors associated with successful response to endoscopic drainage is needed.</p><p><b>208</b></p><p><b>Endoscopic ultrasound-fine needle aspiration in a regional secondary centre in Victoria: an evaluation of diagnostic yield for pancreatic malignancies in pancreatic masses and complication rates</b></p><p><b>Daniel Yee Lee Ng</b>, Mitchell Steele, Tania Chapman, Sajith Kattiparambil Gangadharan and Dileep Mangira</p><p><i>Grampians Health, Ballarat, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic ultrasound (EUS) with fine needle aspiration/biopsy (FNA) is an important diagnostic tool for pancreatic masses. Multiple aspects of the EUS-FNA process may influence the efficacy of results including needle gauge, number of needle passes and patient presentation. This study evaluated the efficacy and safety of EUS-FNA approach in investigating pancreatic masses at a secondary regional centre.</p><p><b><i>Methods:</i></b> All cases of EUS with suspected pancreatic lesions performed by a single endoscopist at a secondary regional centre were identified between June 2022 and September 2023. Data collected included: indication, performance of FNA, needle gauge utilized, number of passes performed, histology results, complications, and presentations to hospital within 4-week period post-procedure. Pathology results that were positive for neoplastic findings were noted as “cytologic positive”, and if further confirmed via surgical means are considered “histologic positive”. For pathology results that were negative, subsequent radiological investigations were identified and assessed for progression. If no surveillance was performed or found 6-months after procedure, the case was excluded as loss of follow-up. If surveillance imaging showed progression, the instance was considered false-negative, and if no progression, this was considered confirmation of benign findings. A calculation of sensitivity, specificity, positive predictive value (PPV) and negative predictive value was performed; as well as a report of occurrences of complications.</p><p><b><i>Results:</i></b> A total of 86 EUS procedures were identified, 5 were excluded as they were performed for therapeutic purposes. 24 were indicated for pancreatic masses. A total of 22 FNAs were performed in this subgroup. 19 FNAs were positive for neoplastic findings: 17 adenocarcinomas, 1 adenocarcinoma with concurrent chronic lymphocytic leukemia (CLL) in a patient with known CLL, and 1 perivascular epithelioid cell tumour (PEComa). 8 of these findings were confirmed surgically. The remaining 3 FNAs identified 2 intraductal papillary mucinous neoplasms (IPMN) with low-grade dysplasia, 1 of which had radiological progression and the other considered benign. 1 sample was identified as chronic pancreatitis but lost to follow-up. All cases utilized a 22-gauge fine needle biopsy device except in 2 instances where a 25 and 19-gauge needle was utilized due to lack of availability, and an additional 19-gauge needle was utilized. In both cases findings were positive for neoplasms. An average of 3 passes was performed. Cumulative sensitivity was 95%, specificity of 100%, PPV of 100%, and NPV of 50%. A breakdown of figures was provided in red (for “cytologic-only positive” cases) and green (for “histologic positive” cases). This is summarized in figure 1. 4 complications were recorded across the 81 EUS procedures as follows: 1 superficial mucosal tear; 1 exacerbation of chronic pancreatitis; 2 cases of abdominal pain (1 of which was post-ERCP). No complications resulted in mortality. Complication rate 4/81 (4.9%).</p><p><b>224</b></p><p><b>Endo-ACEF: Endoscopic ultrasound-guided gallbladder drainage in the elderly and frail: A prospective multicentre cohort trial</b></p><p><b>Sidhartha Gupta</b><sup>1</sup>, Andrew Gray<sup>1</sup> and Daniel Croagh<sup>1,2</sup></p><p><sup>1</sup><i>Monash Health, Melbourne, Australia;</i> <sup>2</sup><i>St Vincent's Hospital, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Acute cholecystitis (AC) is a prevalent condition requiring emergency surgery, particularly among the elderly and frail population. <sup>(1)</sup> Since 2007, endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) has emerged and evolved as a viable alternative to laparoscopic cholecystectomy for non-surgical candidates. <sup>(2)</sup> Australia's aging population is well documented, with nonagenarians growing faster than any other age group. Although laparoscopic cholecystectomy is the standard treatment for cholecystitis, it poses significant risks for patients with high comorbidity burdens or poor physical health, especially in emergency settings. Data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) shows a cholecystectomy-associated mortality rate of 5.5% in nonagenarians, rising to 9.5% in emergencies. <sup>(3)</sup> Additionally, older patients often experience a more severe disease course, with higher conversion rates to open surgery. <sup>(4, 5)</sup></p><p>Traditionally, percutaneous cholecystostomy (PC) has been used to manage cholecystitis in high-risk surgical candidates. EUS-GBD offers a minimally invasive, definitive treatment, avoiding the drain-related morbidity associated with PC. Recent randomised trials have favoured EUS-GBD over PC for high risk surgical patients with AC given lower rates of adverse events, reinterventions and readmissions. <sup>(6)</sup> Little research has prospectively assessed EUS-GBD as the primary modality specifically in the elderly, who may or may not be high surgical risk, or frail patients of any age.</p><p>We aim to evaluate EUS-GBD utilising a lumen opposing metal stent (LAMS) to as the primary intervention for patients that are either aged eighty-eight years or older, or at least moderately frail. This will include patients who are elderly and frail, elderly and fit, as well as patients that are frail but not necessarily elderly. This age threshold strikes a balance between limiting the intervention between those of extreme age while maximising the potential population that could benefit.</p><p><b><i>Methods:</i></b> This multicentre prospective cohort study evaluates the technical and clinical success of EUS-GBD in patients aged eighty-eight years and older, or those classified as at least moderately frail, across two tertiary academic institutions. The surgical team will assess frailty using the Clinical Frailty Score (CFS), with patients having a CFS ≥ 6 out of 9 total points considered for inclusion. Eligible patients will undergo EUS-GBD with a lumen-apposing metal stent (LAMS) after fitness assessment by the Anaesthetic and Peri-Operative Medical Unit. The primary endpoints are the technical success rate of EUS-GBD (confirmed by endoscopic and CT imaging) and clinical success rate (resolution of symptoms and biochemical improvement). Secondary endpoints include procedure-related morbidity and mortality, and long-term LAMS efficacy and patency. Retrospective data of previous EUS-GBD procedures is also being collected.</p><p><b><i>Discussion:</i></b> We anticipate that our trial will demonstrate high clinical and technical success rates for EUS-GBD, with lower morbidity and mortality compared to traditional surgical approaches. We also expect a reduced rate of recurrent gallstone-related morbidity compared to non-operative treatments for AC. By focusing on elderly and frail patients, this study aims to highlight the benefits of endoscopic definitive treatment. Future research could explore lowering the age and frailty thresholds to expand the benefits of minimally invasive endoscopic treatment to a broader patient population.</p><p><b>References</b></p><p>\n 1. <span>Escartín, A</span>, <span>González, M</span>, <span>Cuello, E</span> et al. <span>Acute cholecystitis in Very Elderly Patients: Disease Management Outcomes, and Risk Factors for Complications</span>. <i>Surgery Research and Practice</i> <span>2019</span>; <span>2019</span>: 9709242.</p><p>\n 2. <span>Baron, TH</span>, <span>Topazian, MD</span>. <span>Endoscopic transduodenal drainage of the gallbladder: implications for endoluminal treatment of gallbladder disease</span>. <i>Gastrointest Endosc.</i> <span>2007 Apr</span>; <span>65</span>(<span>4</span>): <span>735</span>-<span>737</span>.</p><p>\n 3. <span>Irojah, B</span>, <span>Bell, T</span>, <span>Grim, R</span>, et al. <span>Are They Too Old for Surgery? Safety of Cholecystectomy in Superelderly Patients (≥ Age 90)</span>. <i>The Permanente Journal</i> <span>2017</span>; <span>21</span>: 16-013.</p><p>\n 4. <span>Borzellino, G</span>, <span>Sauerland, S</span>, <span>Minicozzi, A</span>, et al. <span>Laparoscopic cholecystectomy for severe acute cholecystitis. A meta-analysis of results</span>. <i>Surgical Endoscopy</i> <span>2008</span>; <span>22</span>: <span>8</span>–<span>15</span></p><p>\n 5. <span>Dubecz, A</span>, <span>Langer, M</span>, <span>Stadlhuber, R</span> et al. <span>Cholecystectomy in the Very Elderly – Is 90 the New 70?</span> <i>Journal of Gastrointestinal Surgery</i> <span>2012</span>; <span>16</span>: <span>282</span>-<span>285</span>.</p><p>\n 6. <span>Teoh, AYB</span>, <span>Kitano, M</span>, <span>Itoi, T</span>, et al. <span>Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in very high-risk surgical patients with acute cholecystitis: an international randomised multicentre controlled superiority trial (DRAC 1)</span> <i>Gut</i> <span>2020</span>; <span>69</span>: <span>1085</span>–<span>1091</span>.</p><p><b>226</b></p><p><b>Can optical evaluation distinguish between T1a and T1b esophageal adenocarcinoma: an international expert inter-observer agreement study</b></p><p><b>Sunil Gupta</b><sup>1,2</sup>, Francesco V Mandarino<sup>1</sup>, Julia Gauci<sup>1</sup>, Anthony Whitfield<sup>1,2</sup>, Clarence Kerrison<sup>1</sup>, Prabha Selvanathan<sup>3</sup>, Puja Kumar<sup>1</sup>, Neal Shahidi<sup>1</sup>, Luke Hourigan<sup>3</sup>, Helmut Messmann<sup>4</sup>, Michael Wallace<sup>5</sup>, Alessandro Repici<sup>6</sup>, Mario Dinis-Ribeiro<sup>7</sup>, Gregory Haber<sup>8</sup>, Andrew Taylor<sup>9</sup>, Irving Waxman<sup>10</sup>, Peter Siersema<sup>11</sup>, Roos Pouw<sup>12</sup>, Arnaud Lemmers<sup>13</sup>, Raf Bisschops<sup>14</sup>, Jeffrey Mosko<sup>15</sup>, Christopher Teshima<sup>15</sup>, Krish Ragunath<sup>16,17</sup>, Thomas Rosch<sup>18</sup>, Oliver Pech<sup>19</sup>, Torsten Beyna<sup>20</sup>, Prateek Sharma<sup>21</sup>, Eric Y Lee<sup>1</sup>, Stephen Williams<sup>1</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Westmead Hospital, Sydney, Australia;</i> <sup>2</sup><i>University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>4</sup><i>University Hospital, Augsburg, Germany;</i> <sup>5</sup><i>Mayo Clinic, Jacksonville, USA;</i> <sup>6</sup><i>Humanitas Research Hospital, Milan, Italy;</i> <sup>7</sup><i>Porto Comprehensive Cancer Center, Porto, Portugal;</i> <sup>8</sup><i>NYU Langone Health, New York, USA;</i> <sup>9</sup><i>St Vincent's Hospital Melbourne, Melbourne, Australia;</i> <sup>10</sup><i>Rush University Medical Center, Chicago, USA;</i> <sup>11</sup><i>Radboudumc Radboud Institute for Health Sciences, Nijmegen, Netherlands;</i> <sup>12</sup><i>Amsterdam University Medical Centers, Amsterdam, Netherlands;</i> <sup>13</sup><i>CUB Erasme Hospital, Belgium;</i> <sup>14</sup><i>University Hospitals Leuven, Belgium;</i> <sup>15</sup><i>St Michael's Hospital, Toronto, Canada;</i> <sup>16</sup><i>Royal Perth Hospital, Perth, Australia;</i> <sup>17</sup><i>Curtin Medical School, Perth, Australia;</i> <sup>18</sup><i>University Hospital Hamburg-Eppendorf, Hamburg, Germany;</i> <sup>19</sup><i>St. John of God Hospital, Regensburg, Germany;</i> <sup>20</sup><i>Evangelisches Krankenhaus, Düsseldorf, Germany;</i> <sup>21</sup><i>Kansas City VA Medical Center, Kansas City, USA</i></p><p><b><i>Introduction:</i></b> While piecemeal EMR for T1a oesophageal adenocarcinoma is acceptable, R0 excision is advocated for T1b disease as it may offer a potential cure and mitigate recurrence. Thus, distinguishing between T1a and T1b disease is imperative under current treatment paradigms. We sought to ascertain whether expert Barrett’s endoscopists were able to make this distinction based on optical evaluation.</p><p><b><i>Methods:</i></b> Sixty sets of endoscopic images of histologically confirmed high grade dysplasia (HGD), T1a and T1b disease (n=20 sets for each) were compiled from consecutive patients at a single institution. Each set contained four images, and were standardized to include an overview, a close-up in high-definition white light, a near-focus magnification image, and a narrow-band image. Experts were invited to predict histology for each set.</p><p><b><i>Results:</i></b> 19 experts from 8 countries (Australia, USA, Italy, Netherlands, Germany, Canada, Belgium, and Portugal) participated. The majority had been practicing for >20 years, with a median annual case volume for Barrett’s EMR of 50 (IQR 18-75), and Barrett’s ESD of 25 (IQR 10-45). Oesophageal adenocarcinoma (T1a/b) could be distinguished from HGD, with a pooled sensitivity of 89.1% (95% CI: 86.7-91.2). When predicting the T-stage for T1b adenocarcinoma cases, the pooled sensitivity was 43.8% (95% CI: 38.5-49.2). Fleiss’ kappa was 0.421 (95% CI: 0.399-0.442, P<0.001), indicating fair-to-moderate agreement.</p><p><b><i>Conclusions:</i></b> Expert Barrett’s endoscopists can reliably differentiate T1a/T1b oesophageal adenocarcinoma from HGD. Although there is fair-to-moderate agreement for T-staging, T1b disease cannot be reliably distinguished from T1a disease. This may have implications on clinical decision making and selection of endoscopic treatment methods.</p><p><b>242</b></p><p><b>Endocytoscopy in real time assessment of histological and endoscopic activity in ulcerative colitis</b></p><p><b>Thanaboon Chaemsupaphan</b><sup>1,2</sup>, Mohammad Shir Ali<sup>1</sup>, Sudarshan Paramsothy<sup>1,3</sup> and Rupert Leong<sup>1,3</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;</i> <sup>2</sup><i>Division of Gastroenterology, Department of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand;</i> <sup>3</sup><i>Faculty of Medicine and Health, University of Sydney, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> With 500-fold magnification, endocytoscopy (CF-H290ECI; Olympus Medical Systems Corporation, Japan; ARTG 121183) is a novel advanced imaging technology enabling real-time imaging of the intestinal mucosa. Endoscopic-histological remission assessment in ulcerative colitis (UC) has become the standard of care. Endoscopists, however, are uninvolved in the assessment of histology. Endocytoscopy might improve workflow and efficiency in the evaluation of UC activity.</p><p><b><i>Methods:</i></b> In this single-center, prospective cohort study at Concord Hospital, Sydney, UC participants consenting to colonoscopy and endocytoscopy for disease assessment were recruited. Methylene blue chromoendoscopy enhanced cellular imaging. Data collected were demographics, disease activity, Mayo endoscopic score (MES) and endocytoscopic activity based on crypt shape, inter-crypt distance, cellular infiltration, and extent of vascularization. Correlation against the MES and the Nancy histological index (NHI) was conducted and validation against the ErLangen Endocytoscopy in CoLiTis (ELECT) score, and the endocytoscopy score (ECSS) was performed using Kappa (κ) statistics and Spearman correlation coefficient (<i>r</i>). <i>P</i> value <0.05 was deemed statistically significant. Duration and adverse events data were recorded.</p><p><b><i>Results:</i></b> A total of 61 colonic bowel segments were evaluated (endoscopic improvement 69%, histological remission 64%; Table 1). Endocytoscopy correlated significantly with MES using both the ECSS (κ=0.57, <i>P</i> < 0.001; <i>r</i>=0.81, <i>P</i><0.001) and the ELECT (κ=1.00, <i>P</i><0.001; <i>r</i>=0.85, <i>P</i><0.001) scoring systems. Endocytoscopy correlated with NHI using both the ECSS (κ=0.47, <i>P</i><0.001; <i>r</i>=0.74, <i>P</i><0.001) and the ELECT (κ=0.89, <i>P</i>< 0.001; <i>r</i>=0.78, <i>P</i><0.001) systems. ELECT score demonstrated superior diagnostic performance in determining histological improvement (NHI 0-1) with sensitivity, specificity, and AUROC of 96%, 100%, and 0.98 (95%CI: 0.95-1.00), versus 70%, 100%, and 0.85 (95%CI: 0.78-0.92) with ECSS. Of the 42 segments in endoscopic remission, 3 (7.1%) demonstrated histological activity on endocytoscopy. No serious adverse events were reported, apart from temporary urinary discolouration from methylene blue excretion.</p><p><i><b>Conclusion</b>:</i> Instant simultaneous endoscopic and histological assessment of IBD is possible using endocytoscopy, which was safe, accurate and well-tolerated. The ELECT score reflects histology significantly better than the ECSS.</p><p><b>Table1</b> Characteristics of colonic lesions of UC cohort\n\n </p><p><b>322</b></p><p><b>Transient biliary stenting facilitates large common biliary duct stone fragmentation, aiding the subsequent retrieval: a case report</b></p><p><b>Denis Rubtsov</b>, Reuben Malloy, David Huynh, Robert Franz and Aditya Agarwal</p><p><i>The Prince Charles Hospital, Brisbane, Australia</i></p><p><b><i>Introduction:</i></b> Endoscopic retrieval of large common bile duct (CBD) stones (>2.5mm) may be challenging during the endoscopic retrograde cholangiopancreatography (ERCP). When the calculus cannot be removed, transient plastic stents are placed in the CBD to permit free bile drainage. There is a growing body of evidence suggesting that stent placement may facilitate stone fragmentation and migration. We present a case of a large stone fragmentation following plastic stents insertion.</p><p><b><i>Case report:</i></b> A 57-year-old man presented with jaundice, pruritis and abdominal pain in January 2024. He was febrile but hemodynamically stable. Total bilirubin was elevated to 142 umol/L (ref: N <20) and conjugated bilirubin was 98 umol/L (ref: N <4). Magnetic resonance cholangio-pancreatography (MRCP) demonstrated no cholelithiasis and an oval 24mm calculus in ampulla, with CBD dilatation to 15mm. Patient was managed with intravenous antibiotics and underwent ERCP, confirming the large calculus presence in the CBD. A sphincterotomy was performed with a monofilament traction sphincterotome using electrocautery. Balloon sphincterotomy was attempted, followed by lithotripter, however this failed to extract the stone. Two 10-French 7cm plastic biliary stents with a single external flap and a single internal flap were placed 6cm into the common bile duct to maintain bile flow. This was followed by an insertion of an additional 7-French 7cm plastic stent with full external and internal pigtails. The patient recovered well, and biochemical parameters normalised. He then represented for laparoscopic cholecystectomy 5 weeks later. A post-operative cholangiogram demonstrated a presence of multiple filling defects in the CBD, instead of one round 25mm calculus seen previously, which appeared to have been fragmented. A follow-up ERCP 8 weeks later showed three calculi in the CBD, the largest of which was 8mm in diameter. These were successfully and atraumatically retrieved with the balloon retraction. There were no large stone observed, and,considering there were no cholelithiasis on the index MRCP, it could be concluded that either the stone has been fragmented or migrated earlier.</p><p><b>340</b></p><p><b>Successful use of dual over-the-scope clips for haemostasis in high-risk duodenal ulcer bleeding</b></p><p><b>James Chen</b><sup>1,2</sup>, Tim Mitchell<sup>1</sup> and Niroshan Muwanwella<sup>1</sup></p><p><sup>1</sup><i>Royal Perth Hospital, Perth, Australia;</i> <sup>2</sup><i>University of Western Australia, Perth, Australia</i></p><p><i><b>Introduction</b>:</i> Managing high-risk active duodenal ulcer bleeding is challenging. While various techniques exist, the use of dual Over-The-Scope (OTS) clips for ulcer haemostasis remains unreported. We present a case illustrating the application of this technique in a complex bleeding duodenal ulcer scenario.</p><p><b><i>Case Presentation:</i></b> A 46-year-old male with recent non-steroidal anti-inflammatory drug use following hip trauma presented with fresh rectal bleeding and signs of hemodynamic instability. Computed tomography angiography revealed an arterial blush in the antrum/D1, prompting a gastroscopy revealing a large superficial ulcer with two distinct areas of active arterial bleeding (Forrest Ia) (Figure A – first ulcer bleeding source). The ulcer had a local adrenaline injection (2 mL, concentration 1:20000) for vasoconstriction and improved visualization. Using an OVESCO OTS clip system, two clips (12mm outer diameter, 6mm arm length) were deployed under direct visualization to individual bleeding vessels within the ulcer bed (Figure B – second ulcer bleeding point with first OVESCO OTS clip seen distally, Figure C – post OTS clip deployment). Careful attention ensured optimal clip placement and avoided luminal obstruction. Haemospray was administered post-clip placement for comprehensive ulcer base coverage. Successful haemostasis was achieved post-clip deployment, with no significant bleeding during observation. Management included 72 hours of proton pump inhibitor infusion, NSAID avoidance, and rebleeding monitoring without complications. A repeat gastroscopy was performed 8 weeks after index gastroscopy with healed ulcer with two clips still in situ and no evidence of duodenal stricture (Figure D).</p><p><b>345</b></p><p><b>A retrospective audit of ERCP practice in the regional hospital</b></p><p><b>Thant Zaw</b><sup>1,2</sup>, Joseph Bradbear<sup>1</sup>, Aditya Agarwal<sup>1</sup>, Peter Boyd<sup>1,2</sup> and Montri Gururatsakul<sup>1,2</sup></p><p><sup>1</sup><i>Cairns Hospital, Cairns North, Australia;</i> <sup>2</sup><i>James Cook University, Cairns, Australia</i></p><p><i><b>Introduction</b>:</i> Endoscopic retrograde cholangiopancreatography (ERCP) plays a vital role in therapeutic procedures for disorders of the biliary and pancreatic systems. However, ERCP also is a high-risk endoscopic procedure. The major complications generally are: adverse events from anesthetic/sedation, bleeding, cholangitis, perforation and post ERCP pancreatitis. This study was done to evaluate our regional ERCP procedures against national standards to ensure quality control and enhance practice methods.</p><p><b><i>Aims and Methods</i></b>: The retrospective audit over a period from May 2018 to December 2020 was conducted to evaluate our local ERCP practices against the guidelines, aiming to ensure quality assurance and enhance practice improvement. With a total of 654 ERCPs analyzed, performed by four different proceduralists, the audit underscores the hospital's role in the regional hospital. The audit utilised a meticulous cross-referencing approach, integrating data from the Provation database with the iEMR database and AUSLAB software for pathology results. The primary outcome is procedure findings and the successful cannulation and ductal clearance rates. The secondary outcome is to measure the complication rates of ERCP.</p><p><b><i>Results</i></b>: Among 645 ERCPs were performed, to highlight the most common findings were biliary stones (50.75%) of the total, followed by biliary stricture (15.81%), microlithiasis (11.98%), malignant biliary obstruction (3.53%). The audit reported an average successful cannulation rate of 91.4% and a ductal clearance rate of 88.74%. The audit also focused on the incidence of complications, with 11 cases of post ERCP bleeding (1.7%), 9 cases had post-ERCP pancreatitis (1.4%), and 2 cases had perforation (0.3%). The sub-analysis of post-ERCP pancreatitis showed that there were 2 cases of mild, 3 cases of moderate, and 4 cases of severe pancreatitis.</p><p><b><i>Conclusion</i></b>: The audit's findings are a testament to the hospital's commitment to maintaining high standards in ERCP procedures, reflecting the low incidence of significant complications highlights the effectiveness of the procedural protocols and pre-emptive measures in place to mitigate risks associated with ERCP.</p><p><b>351</b></p><p><b>Long term follow-up of 35 appendiceal orifice neoplasms resected by endoscopic full thickness resection</b></p><p><b>Oliver Cronin</b><sup>1,2,3,4</sup>, Kayla Meys<sup>2</sup>, Sofia Yuen<sup>2</sup>, Abhinav Vij<sup>2</sup>, Tamas Gonda<sup>2</sup>, Adam Goodman<sup>2</sup>, Michael J Bourke<sup>3,4</sup> and Gregory Haber<sup>2</sup></p><p><sup>1</sup><i>Northern Hospital, Melbourne, Australia;</i> <sup>2</sup><i>NYU Langone, New York, USA;</i> <sup>3</sup><i>University of Sydney, Sydney, Australia;</i> <sup>4</sup><i>Westmead Hospital, Sydney, Australia</i></p><p><b><i>Background and Aims:</i></b> Endoscopic full-thickness resection (EFTR) is an established, safe technique for the resection of appendiceal orifice (AO) neoplasms. Post-EFTR appendicitis is a recognised complication. There are no systematic reviews and a paucity of literature which has assessed medium and long-term outcomes especially with respect to delayed appendicitis, mucocele, or fistula formation. We aimed to evaluate long-term efficacy of EFTR for AO lesions.</p><p><b><i>Patients and Methods:</i></b> Consecutive AO lesions referred for consideration of EFTR were prospectively studied. Multiple data points were recorded including technical success, EFTR histopathological data, complications, and follow-up surveillance data by colonoscopy. Surveillance CT was performed due to concern of potential mucocele from the obstructed remnant appendix.</p><p><i><b>Results</b>:</i> Over a 4 year period to July 2023, 37 AO lesions were referred to a tertiary centre for consideration of EFTR. EFTR was attempted in 35 (95%) lesions. Most lesions were small [median size 10mm, interquartile range (IQR) 10-15mm], Paris 0-IIa morphology (n=32, 91%) with serrated histopathology (n=17, 49%). R0 resection was achieved in the majority of cases (n=34, 97%). Complications included appendicitis (n=4, 11%) and delayed bleeding (n=2, 6%). At 6-month (IQR 4-6 months) surveillance colonoscopy, there was 1 (3%) case of recurrence. This was successfully treated endoscopically, confirmed on a second surveillance colonoscopy. There was one case of appendicitis of the remnant at 7 months. At surveillance CT abdomen/pelvis (median 15 months, IQR 7-37 months), 2/17 (12%) fistulas were identified. Both of these patients had presumed adhesions due to abdominal surgery prior to EFTR.</p><p><i><b>Conclusions</b>:</i> EFTR is a safe, effective and durable technique for the curative resection of AO lesions. Appendicitis is a relatively common complication but often managed conservatively. The long-term significance post-EFTR fistulas remains unclear. Caution should be exercised when considering EFTR in a patient with prior regional surgery.</p><p><b>352</b></p><p><b>Endoscopic full thickness resection is a viable alternative to endoscopic submucosal dissection (ESD) for high-risk colonic lesions</b></p><p><b>Oliver Cronin</b><sup>1,2,3,4</sup>, Kayla Meys<sup>2</sup>, Sean Hacking<sup>2</sup>, Mouyed Alawad<sup>2</sup>, Sofia Yuen<sup>2</sup>, Jonathan Cohen<sup>2</sup>, Tamas Gonda<sup>2</sup>, Michael J Bourke<sup>3,4</sup> and Gregory Haber<sup>2</sup></p><p><sup>1</sup><i>Northern Hospital, Melbourne, Australia;</i> <sup>2</sup><i>NYU Langone, New York, USA;</i> <sup>3</sup><i>University of Sydney, Sydney, Australia;</i> <sup>4</sup><i>Westmead Hospital, Sydney, Australia</i></p><p><b><i>Background and Aims:</i></b> Endoscopic submucosal dissection (ESD) is the primary resection technique recommended for high-risk colonic lesions to ensure an R0 resection. Endoscopic full-thickness resection (EFTR) offers a viable alternative. There is little available data on technique, efficacy and cure. We aimed to evaluate outcomes of patients with lesions containing high-grade dysplasia (HGD) and invasive cancer, resected by EFTR.</p><p><b><i>Patients and Methods:</i></b> Consecutive non-lifting lesions referred to a single tertiary centre with suspected localised advanced pathology for consideration of EFTR were prospectively studied. Multiple data points were recorded including technical success, EFTR histopathological data, complications, and follow-up surveillance data.</p><p><i><b>Results</b>:</i> Over a 4 year period to July 2023, 39 lesions were considered eligible for EFTR as an alternative to EMR or ESD, of which 33 (85%) underwent EFTR. 18/33 (55%) lesions contained cancer and 15/33 (45%) lesions contained HGD only. The median size of cancer was 7mm [Interquartile range (IQR) 4-10mm] contained within a median lesion size of 30mm (IQR 21-31mm). The median depth of invasion was 2550μm (IQR 1625-3075μm) and the deepest resected layer contained sub-serosal fat. Of the lesions containing cancer removed by FTR, 17/18 (94%) had an R0 resection. The case without an R0 resection had deep margin involvement, resected to the sub-serosa (depth 4000μm). At 6 month [Interquartile range (IQR) 5-7 months] surveillance colonoscopy, there was 1/23 (4%) case with recurrence, successfully re-resected with FTR, with cure confirmed on second surveillance colonoscopy. Of the patients with cancer who were referred for surgical resection post-FTR, no (0/7, 0%) cases had residual cancer within the surgical specimen.</p><p><b><i>Conclusions</i></b>: EFTR offers a viable, safe and effective alternative to ESD for lesions with advanced pathology. Resection options need to be individualised and clearly outlined to the patient.</p><p><b>372</b></p><p><b>One parathyroidectomy and a cyst-gastrostomy later: an unusual case of hypercalcaemic pancreatitis as a first presentation of primary hyperparathyroidism</b></p><p><b>Eloise James</b>, Tessa Greeve, Gregory Moore and Fiona Pavan</p><p><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Acute pancreatitis is a common presenting complaint in the Emergency Department, often with a clear aetiology. Here we present the case of acute necrotising pancreatitis, requiring emergency endoscopic drainage, as a first presentation of primary hyperparathyroidism (PHPT) in a young female patient.</p><p><b><i>Case report</i></b>: A young woman presented to the Emergency Department with abdominal pain and a reduced level of consciousness. Initial investigations revealed a serum lipase level of 8184 U/L (reference range 0-60U/L) suggestive of pancreatitis. Specific screening for causes found only raised serum adjusted calcium (2.89 mmol/L, reference range 2.1-2.6mmol/L). There was no ultrasound evidence of cholelithiasis or choledocholithiasis. She had no history of alcohol use, and no significant medical history. This suggested hypercalcaemia related acute pancreatitis, and further investigations found raised serum PTH (7.7pmol/L, reference range 1.5-7.0pmol/L) and neck imaging showed a parathyroid mass. She became febrile, and abdominal MR imaging showed necrotising pancreatitis with haemorrhagic collections, initially conservatively managed with broad spectrum antibiotics. Further CT imaging showed increasing size of collections (figure 1) with gastric outlet obstruction, and due to worsening sepsis she underwent endoscopic ultrasound (EUS) guided cyst-gastrostomy on day 18 of admission, and her clinical status improved. Contemporaneous medical management of PHPT-hypercalcaemia failed to reduce calcium levels, increasing to a maximum of 3.4mmol/L (reference range 2.1-2.6mmol/L). Due to this, she underwent a parathyroidectomy on day 19 of admission, and serum calcium levels reduced to within normal range. The relationship between pancreatitis and PHPT-hypercalcemia is debatable, and case reports in the literature suggest notably higher levels of serum calcium than this case, with less severe pancreatitis. Increasing serum calcium level in this case was not associated with worsening clinical or biochemical markers of pancreatitis, following definitive endoscopic management of associated pancreatic collections. This suggests that serum calcium level is not directly related to clinical course of pancreatitis, beyond a possible trigger threshold level as suggested in literature. However, calcium sequestration can be a feature of early pancreatitis, which in a case of PHPT may hinder interpretation of calcium levels.</p><p><b>379</b></p><p><b>Introducing innovative low-code/no-code applications in endoscopy: An app for streamlining triage, enhancing safety, and building regional connectivity for endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound (EUS) at a high volume, tertiary referral hospital</b></p><p><b>Clarence Kerrison</b>, <b>Brian Lam</b>, Anthony Whitfield, Julia Gauci, Anthony Sakiris, Francesco V Mandarino, Eric Y Lee, Stephen Williams, Nicholas Burgess and Michael J Bourke</p><p><i>Westmead Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Low-code/no-code (LCNC) applications remain underutilised as a clinician-driven solution for daily hospital tasks. Existing paper-based systems used for triage and booking of endoscopy referrals are inefficient, prone to documentation errors, and contribute to paper wastage. Our objective was to create an online referral pathway and real-time tracking board for ERCP and EUS to replace the current paper-based system at a large tertiary referral hospital.</p><p><b><i>Methods:</i></b> Using Microsoft’s Power Platform™, PowerApps™, and Power Automate™, gastroenterology clinicians developed an online referral system, bookings and management board, and automated notifications centre for inpatient and outpatient ERCP and EUS referrals. The system went live in May 2023. Results were monitored to April 2024, when referrers were surveyed on the application’s usability.</p><p><b><i>Results:</i></b> 1,392 requests for ERCP and EUS were monitored using the online board, 762 (55%) originating from the new online referral pathway, 405 (29%) manually uploaded from existing paper requests and 225 (16%) re-bookings facilitated by a re-request feature in the application. Of the total requests, 1030 (74%) were tracked to completion, with 219 pending procedures and 103 awaiting future surveillance, while 32 were declined and 8 on hold. Of the online referrals, 170 triggered high suspicion of cancer notifications, with 90% prioritised to first procedure dates within 2 weeks. Online referrals additionally had 100% documentation of patient co-morbidities, anti-platelet/anti-coagulant history through mandatory user input, this compared to 44% of the original paper-based requests (Pearson X<sup>2</sup> = 530.24, p < 0.001). The boards real-time interface provides a full patient journey overview. On average 187 automated email and push notifications per month informed referrers of confirmed booking dates and delayed or completed procedures. 21 of 165 referring doctors responded to a survey representing six referring hospitals, 100% found the online referral system very or somewhat easy to fill out, 95% found the automated messages helpful, and one third booked a follow-up appointment after receiving a completed notification. 100% of responders recommended continuing with the system.</p><p><b><i>Conclusion:</i></b> The use of LCNC applications for triage and booking of ERCP and EUS procedures enhances clinical decision making and efficiency in high volume referral centres, whilst coordinating feedback to referrers and endoscopy staff. The LCNCs application ensured 100% compliance with pre-procedural safety checks. This application was created using existing and accessible Microsoft 365™ business licencing and can be securely integrated into other hospitals with ease.</p><p><b>386</b></p><p><b>Diagnostic yield of rapid onsite evaluation and cell block in endoscopic ultrasound-guided fine needle biopsy of gastrointestinal lesions</b></p><p><b>Mohammad Shir Ali</b>, Donna Gillies, Juan Olivares, Dane Cook and Stephen Philcox</p><p><i>John Hunter Hospital, Newcastle, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic ultrasound (EUS)-guided fine needle biopsy (FNB) often incorporates in-room cytology, commonly referred to as rapid onsite evaluation (ROSE), where cytology slides are prepared and assessed in real-time. In contrast, the cell block (CB) technique uses tissue fragments to create a paraffin block, enabling multiple sections to be cut for in-lab analysis and immunostaining. Despite the advantages of ROSE, the advent of advanced fine-needle biopsy and utilisation of macroscopic on-site evaluation (MOSE) raises questions about the necessity of ROSE. This study examines the effectiveness of ROSE and CB in EUS-guided biopsy at our institution.</p><p><b><i>Methods:</i></b> We retrospectively reviewed medical records of patients aged 16 or older who underwent an EUS at our institution over the past five years. We included patients who received an EUS-guided FNB of any gastrointestinal lesion.</p><p><b><i>Results:</i></b> 617 patients underwent EUS with 256 scheduled for an EUS FNB. Out of these, 226 underwent the biopsy. ROSE was performed in 204 cases. Biopsies targeted pancreatic lesions (163), luminal (23), hepatobiliary (11), and other including lymph nodes (28). Out of 204 patients who underwent EUS FNB with ROSE, 104 (51%) had malignant or neoplastic cytology on ROSE. However, this number increased to 127 (62.2%) upon in-lab evaluation. This increase was primarily due to 21 cases where cytology initially identified as atypical during ROSE was reclassified as malignant or neoplastic after laboratory analysis. Additionally, while 18 out of 204 samples (8.8%) were deemed inadequate during the ROSE evaluation, upon in-lab analysis the final tissue adequacy rate was 97.6% (Table 1). Additionally, 120 patients underwent EUS-guided biopsies of solid pancreatic lesions. Of these, cytology slides were diagnostic in 100 cases, resulting in a diagnostic yield of 83.3%. In contrast, CB had a lower diagnostic yield of 39%. Although fewer patients had EUS-guided biopsies of luminal lesions or lymph nodes, the diagnostic yield for cytology slides and CB were relatively consistent across these groups (Table 2).</p><p><b><i>Conclusion</i></b>: Our study underscores the significance of ROSE in enhancing the diagnostic yield of EUS-guided FNB for solid pancreatic lesions, with cytology slides proving highly effective in obtaining definitive diagnoses. While CBs appeared to have a lower diagnostic yield, this may be influenced by cases where a conclusive diagnosis was already achieved through cytology slides, suggesting that the potential utility of CBs could be underrepresented. To comprehensively assess these findings, prospective randomised trials comparing outcomes with and without ROSE are recommended.</p><p><b>405</b></p><p><b>Impact of margins ablation on the efficacy of cold-forceps avulsion with snare-tip soft coagulation (CAST) for non-lifting large non-pedunculated colorectal polyps</b></p><p><b>Francesco V Mandarino</b><sup>1</sup>, Tim O'Sullivan<sup>1,2</sup>, Julia Gauci<sup>1</sup>, Renato Medas<sup>1</sup>, Clarence Kerrison<sup>1,2</sup>, Anthony Whitfield<sup>1,2</sup>, Brian Lam<sup>1</sup>, Varan Perananthan<sup>1</sup>, Sunil Gupta<sup>1,2</sup>, Stephen J Williams<sup>1</sup>, Oliver Cronin<sup>1,2</sup>, Eric Y Lee<sup>1</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology and Hepatology, Westmead Hospital;</i> <sup>2</sup><i>University of Sydney, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic Mucosal Resection (EMR) with Margin Thermal Ablation by Snare-tip Soft Coagulation (MTA) is effective to treat Large (>20mm) Non-Pedunculated Colorectal Polyps (LNPCP) with recurrence in large studies at <2%. Non-lifting LNPCP (NL-LNPCP) account for approximately 10% of LNPCP and are well managed by EMR with adjunctive Cold-forceps Avulsion with adjuvant Snare-Tip soft coagulation (CAST) for non-lifting areas, however recurrence occurs in >10%. We sought to evaluate the effect of MTA on NL-LNPCPs treated by EMR and CAST.</p><p><b><i>Methods:</i></b> Prospective observational data on consecutive patients with NL-LNPCPs treated by EMR and CAST at a single tertiary center was evaluated. Two cohorts were established: the pre-MTA period (January 2012-June 2017) and the MTA period, (July 2017-October 2023). The primary outcome was the comparison of recurrence rates between the two groups at first surveillance colonoscopy at 6 months (SC1).</p><p><b><i>Results:</i></b> From January 2012 to October 2023, 298 NL-LNPCPs in 298 patients (median age 69.1 years, interquartile range [IQR] 61.5-76.7 years, 43.4% male) underwent EMR and CAST (median size 36.0mm, IQR 24.7-54.2mm): 72 lesions pre-MTA and 226 with MTA. The MTA cohort had a higher rate of NL-LNPCP in complex locations (ileocecal valve, ano-rectal junction, appendiceal orifice) (18.6% vs 5.6%, p=0.02), granular lesions (61.9% vs 41.7%, p=0.01), and lesions with submucosal fibrosis (87.2% vs 72.2%, p=0.05). No differences were observed in procedural time. At SC1, recurrence was lower in the MTA cohort compared to the pre-MTA cohort (2.7% vs 9.7%, p<.001). Deep mural injury type III-V (4.4% vs 4.2%, p=.93) and post-procedural bleeding (5.3 vs 4.2%, p=.94) was similar between the MTA and pre-MTA cohort respectively. There was one case of delayed perforation in the pre-MTA group.</p><p><b><i>Conclusion:</i></b> The implementation of MTA significantly reduced recurrence at SC1 for NL-LNPCP treated by EMR with CAST. The refinement of CAST and addition of MTA in recent years has enabled the treatment of more complex lesions with greater effectiveness without compromising safety.</p><p><b>Table 1</b>\n \n </p><p><b>408</b></p><p><b>Outcomes of endoscopic submucosal dissection for the treatment of oesophageal squamous dysplasia and early squamous cell carcinoma in the West</b></p><p>Sunil Gupta<sup>1,2</sup>, <b>Francesco V Mandarino</b><sup>1</sup>, Julia Gauci<sup>1</sup>, Anthony Whitfield<sup>1,2</sup>, Timothy O'Sullivan<sup>1,2</sup>, Oliver Cronin<sup>1,2</sup>, Clarence Kerrison<sup>1,2</sup>, Andrew Tang<sup>1</sup>, Eric Y Lee<sup>1</sup>, Stephen J Williams<sup>1</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;</i> <sup>2</sup><i>University of Sydney, Sydney, Australia</i></p><p><i><b>Background and Aim</b>:</i> Endoscopic submucosal dissection (ESD) has evolved to become a viable treatment option for oesophageal squamous dysplasia (SD) and early squamous cell carcinoma (ESCC). Although enbloc, R0, excision has the potential to yield an endoscopic cure, surgery remains the standard of care in the West. Furthermore, Western data pertaining to endoscopic outcomes is limited. We aimed to assess the efficacy and safety of ESD for SD and ESCC in a single tertiary referral centre.</p><p><b><i>Methods:</i></b> We conducted a prospective observational cohort study over 87 months until November 2023 in consecutive patients undergoing ESD for SD or ESCC. The primary outcomes were enbloc, R0 and curative resection rates. Secondary outcomes included procedure duration, tumor recurrence and adverse events.</p><p><b><i>Results:</i></b> 112 consecutive patients were referred for treatment and underwent ESD (median age 73 [IQR 68-78]; 50% male; Table 1). Median lesion size was 30 mm (IQR 20-50mm) and Paris IIa was the most common morphology (58.9%). Enbloc resection was achieved in 109 (97.3%) and R0 excision in 87 (77.7%). Curative resection in cases of LGD and HGD, where margins were clear of dysplasia, was 7/11 (63.6%) and 31/34 (91.2%) respectively. In those with T1a/T1b SCC, the curative resection rate was 20/61 (32.8%). In T1a SCC lesions, 11/20 (55.0%) had a curative ESD. Of the remainder, 6/9 were poorly differentiated, 1/9 had LVI, and 2/9 had positive margins (1 deep, 1 peripheral). In T1b SCC lesions, 9/41 were curative (22.0%). The remainder were either poorly differentiated, >T1b-SM1, LVI positive or a combination. In those with T1a/T1b disease, without adverse tumor biology, ESD achieved curative resection in 20/22 (90.9%). In the 41/61 (67.2%) T1a/T1b patients that did not meet criteria for cure, subsequent treatment included surgery (n=5), radiotherapy (n=5) and chemoradiotherapy (n=1). After MDT discussion, the remaining 30 were managed conservatively, due to advanced age or comorbidities. In these, recurrence occurred in 6/30 patients (1 local, 3 nodal, 2 metastatic) at a median follow up of 12 months (6-18 months). The median hospital length of stay was 1 day (IQR 1-3). Oesophageal strictures occurred in 46 patients (41.1%), requiring a median of 3 dilations (IQR 1-8). There were 2 cases of delayed bleeding. There were no perforations.</p><p><b><i>Conclusion:</i></b> ESD is curative for low and high-grade dysplasia. In a Western setting, ESD offers definitive T-staging and has the potential to yield a cure in almost 33% of T1a and T1b SCC cases. Due to a high risk of disease recurrence, adjuvant therapy should be considered in cases of a non-curative resection.</p><p><b>Table 1</b>\n \n </p><p><b>416</b></p><p><b>Five-year clinical outcomes after per oral endoscopy myotomy (POEM) for achalasia</b></p><p><b>Varan Perananthan</b><sup>1,2</sup>, Lucy Bracken<sup>1</sup>, Andrea Huang<sup>3,4</sup>, Francesco V Mandarino<sup>1</sup>, Brian Lam<sup>1</sup>, Julia Gauci<sup>1</sup>, Clarence Kerrison<sup>1</sup>, Sunil Gupta<sup>1,2</sup>, Nicholas Burgess<sup>1,2</sup>, Spiro Raftopoulos<sup>5</sup>, Bronte Holt<sup>6</sup>, Luke Hourigan<sup>3,4</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;</i> <sup>2</sup><i>Westmead Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;</i> <sup>4</sup><i>Gallipoli Medical Research Institute, School of Medicine, The University of Queensland, Brisbane, Australia;</i> <sup>5</sup><i>Department of Gastroenterology and Hepatology, Sir Charles Gairdner Hospital, Perth, Australia;</i> <sup>6</sup><i>Department of Gastroenterology, St Vincent's Hospital, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Per oral endoscopic myotomy (POEM) is a well-established treatment for achalasia with clinical success exceeding 90%. However, the durability of this response is unknown. We sought to evaluate the long-term outcomes of POEM for achalasia 5 years and beyond in a multi-centre setting.</p><p><b><i>Methods:</i></b> Patients who underwent POEM for achalasia types 1, 2, and 3 were prospectively enrolled in a multi-centre observational study with data collected on technical aspects and short-term outcomes. Eckardt scores were calculated before treatment and at 6 months and 2 years after POEM. Among this cohort, patients who underwent POEM before June 2019 were contacted to assess long-term outcomes. The primary outcome was to evaluate the long-term clinical success at 5 years or beyond defined by an Eckart score ≤ 3 without the need for re-intervention. Secondary outcomes included identifying factors associated with re-intervention and subsequent management strategies.</p><p><b><i>Results:</i></b> A total of 237 patients underwent POEM for achalasia in four Australian tertiary centres between January 2014 to June 2019. Median follow up was 6.0 years, (IQR 5.2 – 7.1 years). 47.6% of patients had Type 1, 35.9% had Type 2 and 16.5% had Type 3 achalasia. Previous treatments prior to POEM included Hellers myotomy; 12.6%, pneumatic balloon dilatation; 50.4% and botulinum toxin injection; 8.7%. The median Eckardt score prior to POEM was 8.0 (IQR 6.0 – 9.0) and at 6 months post-POEM was 0.0 (IQR 0.0 – 1.0, p<0.001). At 2 and 5 years follow up scores were 1.0 (IQR 0.00 – 2.00, p<0.001) and 0.0 (IQR 0.0 – 2.0, p<0.001) respectively. Five-year freedom from intervention was 87.6%. 6.2% required a re-do POEM at a median of 14 months post-POEM (IQR13.0 – 24.0) and 8.9% required a pneumatic dilatation at a median of 18 months post-POEM IQR (9.0 – 24.0). Type III achalasia was a risk factor for re-intervention, relative risk (RR) 1.41 (95% CI 1.17 – 1.60, p=0.04). Previous Heller’s was not a risk factor for re-intervention, RR 1.07 (95%CI 0.27 – 3.58), however pneumatic dilatation prior to initial POEM increased the risk of re-intervention, RR 1.71 (95% CI 1.12 – 2.33, p=0.02). Intra-procedural complications (such as major bleeding) were not risk factors for re-intervention, RR 0.97 95% CI (0.16 – 5.35).</p><p><b>444</b></p><p><b>Prevalence of endoscopically curable low-risk cancer amongst large non-pedunculated colorectal polyps</b></p><p><b>Julia Gauci</b><sup>1</sup>, Anthony Whitfield<sup>1,2</sup>, Renato Medas<sup>3,4</sup>, Clarence Kerrison<sup>1,2</sup>, Francesco V Mandarino<sup>1</sup>, David Gibson<sup>5</sup>, Timothy O'Sullivan<sup>1,2</sup>, Oliver Cronin<sup>1,2</sup>, Sunil Gupta<sup>1,2</sup>, Brian Lam<sup>1</sup>, Varan Perananthan<sup>1</sup>, Luke Hourigan<sup>6</sup>, Simon Zanati<sup>5</sup>, Rajvinder Singh<sup>7</sup>, Spiro Raftopoulos<sup>8</sup>, Alan Moss<sup>5</sup>, Gregor Brown<sup>5</sup>, Amir Klein<sup>9</sup>, Lobke Desomer<sup>10</sup>, David Tate<sup>11,12</sup>, Steven Williams<sup>1</sup>, Eric Y Lee<sup>1,2</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Westmead Hospital;</i> <sup>2</sup><i>University of Sydney Medical School, Sydney;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, The Alfred Hospital, Department of Gastroenterology and Hepatology, Epworth Hospital, Melbourne;</i> <sup>4</sup><i>Department of Gastroenterology, Princess Alexandra Hospital (Queensland Health), Brisbane;</i> <sup>5</sup><i>Department of Gastroenterology and Hepatology, Lyell McEwin Hospital, Adelaide, South Australia, Australia;</i> <sup>6</sup><i>Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia;</i> <sup>7</sup><i>Centro Hospitalar e Universitario Sao Joao, Porto, Portugal;</i> <sup>8</sup><i>Faculty of Medicine of University of Porto, Portugal;</i> <sup>9</sup><i>Ambam Heath Care Campus, Rappaport Faculty of Medicine, Technion Institute of Technology, Haifa, Israel;</i> <sup>10</sup><i>AZ Delta Roeselare, Ghent, Belgium;</i> <sup>11</sup><i>Department of Gastroenterology and Hepatology, University Hospital of Ghent, Ghent, Belgium;</i> <sup>12</sup><i>Faculty of Medicine, University of Ghent, Ghent, Belgium</i></p><p><b><i>Background and Aims:</i></b> Endoscopic submucosal dissection (ESD) is increasingly promoted for the treatment of all large non-pedunculated colorectal polyps (LNPCP), to cure potential low-risk cancers (superficial submucosal invasion without additional high-risk histopathological features). The effect of a universal en bloc strategy on oncological outcomes for the treatment of LNPCP in the right colon is unknown. We evaluated this in a large Western population.</p><p><b><i>Methods:</i></b> A prospective cohort of patients referred for endoscopic resection (ER) of LNPCP was analysed. Patients found to have cancer after ER and those referred directly to surgery were included. The primary outcome was to determine the proportion of right colon LNPCP with low-risk cancer.</p><p><b><i>Results:</i></b> Over 180 months until June 2023, 3294 sporadic right colon LNPCP in 2956 patients were referred for ER at 7 sites (median size 30mm [IQR 15]). 63 (2.1%) patients were referred directly to surgery and cancer was proven in 56 (88.9%). 2851/2956 (96.4%) LNPCP underwent ER (median size 35mm [IQR 20]) of which 75 (2.6%) were cancers. The overall prevalence of cancer in the right colon was 4.4% (131/2956). Detailed histopathological analysis was possible in 115/131 (88%) cancers (71 after ER, 44 direct to surgery). After excluding missing histopathological data, 23/2940 (0.78%) sporadic right colon LNPCP were low-risk cancers.</p><p><b><i>Conclusions:</i></b> The proportion of right colon LNPCP referred for ER containing low-risk cancer amenable to endoscopic cure was <1%, in a large, multicentre Western cohort. A universal ESD strategy for the management of right colon LNPCP is unlikely to yield improved patient outcomes given the minimal impact on oncological outcomes.</p><p><i><b>Clinical Trial:</b></i> Australian Colonic Endoscopic Resection (ACE) cohort: NCT01368289 (https://classic.clinicaltrials.gov/ct2/show/NCT01368289); NCT02000141 (https://classic.clinicaltrials.gov/ct2/show/NCT02000141)</p><p><b><i>Key words:</i></b> colorectal cancer, endoscopic mucosal resection, endoscopic submucosal dissection, large non-pedunculated colorectal polyps</p><p><b>446</b></p><p><b>Endoscopic resection related duodenal strictures: Prevalence, risk factors, management and outcomes</b></p><p><b>Julia Gauci</b><sup>1</sup>, Renato Medas<sup>2,3</sup>, Francesco V Mandarino<sup>1</sup>, Clarence Kerrison<sup>1,4</sup>, Anthony Whitfield<sup>1,4</sup>, Sunil Gupta<sup>1,4</sup>, Hunter Wang<sup>4</sup>, Mayenaaz Sidhu<sup>1,4</sup>, Brian Lam<sup>1</sup>, Lucy Bracken<sup>1</sup>, Varan Perananthan<sup>1</sup>, Timothy O'Sullivan<sup>1,4</sup>, Oliver Cronin<sup>1,4</sup>, Steven Williams<sup>1,4</sup>, Eric Y Lee<sup>1,4</sup>, Nicholas Burgess<sup>1,4</sup> and Michael J. Bourke<sup>1,4</sup></p><p><sup>1</sup><i>Westmead Hospital, Sydney, Australia;</i> <sup>2</sup><i>The University of Sydney, Westmead Clinical School of Medicine, Sydney, Australia;</i> <sup>3</sup><i>Centro Hospitalar e Universitario Sao Joao, Porto, Portugal;</i> <sup>4</sup><i>Faculty of Medicine of University of Porto, Porto, Portugal</i></p><p><b><i>Background and Aim:</i></b> Endoscopic resection (ER) of large (≥15mm) duodenal laterally spreading lesions (D-LSLs) is now standard of care. Data on prevalence, risk factors and management of strictures after ER of D-LSL are absent; we sought to evaluate this is in a large tertiary referral cohort.</p><p><b><i>Patients and Methods:</i></b> A prospective cohort of D-LSLs treated by ER in an expert tissue resection centre was analysed. Strictures were considered \"severe\" if patients experienced obstructive symptoms, \"moderate\" if an adult gastroscope (diameter 9.9mm) could not pass the stenosis, or \"mild\" if there was resistance on successful passage. When necessary, dilatation was performed every 2-4 weeks, until scope passage without resistance was achieved. Primary outcomes included stricture prevalence, risk factors and management.</p><p><b><i>Results:</i></b> Over 193 months until February 2023, 246 lesions in 239 patients were included (51.2% male, median age 70 years [IQR 14], median size 35mm [IQR 25]). 30 (12.2%) resections resulted in stenosis; 14 mild (46.7%), 4 moderate (13.3%) and 12 severe (40%). 18 (7.3%) required balloon dilation (median number of sessions, 2 [IQR 6]). After multivariable analysis, post ER-defect circumference ≥80% was the strongest independent predictor for stricture formation (OR 62.96 [confidence interval 17.9-276.7], p<0.001). The incidence of stricture formation with an ER-defect ≥80%, 60-79% and <60% was 72.2% (n=26/36), 12.5% (n=4/32) and 0% (n=0/178) respectively. All severe strictures (12/12, 100%) occurred in ER-defects ≥80%.</p><p><b><i>Conclusions:</i></b> ER-defect circumference strongly predicts stricture formation following ER of D-LSL. These findings can be used to guide informed consent and post-procedural care.</p><p><b>447</b></p><p><b>Safety and efficacy of endoscopic retrograde cholangiopancreatography in nonagenarians - A retrospective cohort study</b></p><p><b>Amirah Etchegaray</b><sup>1</sup>, Sanjivan Mudaliar<sup>1</sup>, Kimberley Ryan<sup>1</sup>, Karen Hay<sup>2</sup>, Jason Hwang<sup>1</sup>, Benedict Devereaux<sup>1</sup>, Mark Appleyard<sup>1</sup> and Florian Grimpen<sup>1</sup></p><p><sup>1</sup><i>Royal Brisbane and Women's Hospital, Brisbane, Australia;</i> <sup>2</sup><i>QIMR Berghofer Medical Research Institute, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Increasing numbers of older patients with pancreatobiliary disease are undergoing Endoscopic Retrograde Cholangiopancreatography (ERCP). Older patients may be at higher risk of post-ERCP complications due to age and comorbidities, however, data to support this claim is lacking. The aim of this study was to evaluate long-term mortality, procedural outcomes, and safety of ERCP in nonagenarian patients aged 90 years and older.</p><p><b><i>Methods:</i></b> A retrospective study of consecutive patients aged ≥90 years that underwent ERCP at a single adult tertiary hospital between March 2011 and April 2023. Subjects were identified from a prospectively maintained endoscopy database (Provation MD). Endoscopic records were reviewed for procedural factors, including successful biliary cannulation, sphincterotomy, and stent placement. The primary outcome was long-term survival. Secondary outcomes included procedural success and adverse events. Post-ERCP adverse events were classified according to the American Society for Gastrointestinal Endoscopy (ASGE) guidelines. Logistic regression was used to analyse procedural outcomes, survival explored using Kaplan-Meier methods and factors predictive of survival identified using Cox proportional hazard modelling.</p><p><b><i>Results:</i></b> 159 consecutive ERCP were performed in 115 nonagenarian patients. The mean age of the cohort was 92.3 (SD ± 2.1); 67% of patients were referred from a rural or regional hospital with a steady increase in ERCPs performed throughout the study period (Figure 1A). Choledocholithiasis with cholangitis (78.6%) was the most common indication, followed by malignant biliary obstruction (MBO, 18.9%), and bile leak (2.5%). Majority [88%] of nonagenarians with benign pathology were symptomatic (cholangitis and/or raised pre-procedure bilirubin >20μmol/L) at first ERCP, including 9% with a non-native papilla. Survival was significantly reduced with malignancy, with a 30-day, 3-month and 1 year survival of 78%, 52% and 9% respectively, compared to 98%, 94% and 89% for choledocholithiasis (p=<0.001, Figure 1B). Technical success was achieved in 91% of index ERCPs including 95% of procedures for benign pathology and 67% for MBO (p=<0.001). Complications occurred in 5% of procedures, most commonly cardiorespiratory (1.8%), bleeding (1.2%) and pancreatitis (0.6%). The 30-day mortality in patients that experienced a complication was 13.4% (n=1, choledocholithiasis with cholangitis).</p><p><b><i>Conclusion:</i></b> Our data suggests that therapeutic ERCP is a safe, effective and clinically relevant intervention for benign and malignant pathology in select nonagenarians. Age does not constitute a barrier to the performance of ERCP in appropriately selected patients. Nonagenarians may be counselled for a success and complication rate equivocal to younger populations.</p><p><b>449</b></p><p><b>Impact of margin thermal ablation on recurrence after endoscopic mucosal resection of large (≥40mm) colorectal lesions</b></p><p><b>Julia Gauci</b><sup>1</sup>, Clarence Kerrison<sup>1,2</sup>, Anthony Whitfield<sup>1,2</sup>, Timothy O'Sullivan<sup>1,2</sup>, Sunil Gupta<sup>1</sup>, Francesco V Mandarino<sup>1</sup>, Brian Lam<sup>1</sup>, Varan Perananthan<sup>1</sup>, Oliver Cronin<sup>1</sup>, Renato Medas<sup>1</sup>, Eric Y Lee<sup>1</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Westmead Hospital;</i> <sup>2</sup><i>Westmead Clinical School of Medicine, The University of Sydney, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic mucosal resection (EMR) of large (≥20mm) non-pedunculated colorectal polyps (LNPCP) ≥40mm is complex, and associated with an increased risk of recurrent or residual adenoma (RRA). Margin Thermal Ablation to the EMR defect margin using snare-tip soft coagulation (MTA) reduces the rate of RRA. Its impact on this high-risk LNPCP subgroup is unknown. We sought to analyse its effect in a large prospective cohort of LNPCP ≥40mm.</p><p><b><i>Methods:</i></b> We retrospectively analysed a prospectively collected cohort of consecutive patients who underwent conventional EMR in an expert tissue resection centre. MTA technique was developed in 2012. Enrolment for the MTA randomised control trial took place between July 2013-May 2016 and became standard practice from mid-2017. The cohort was divided into three phases: ‘pre-MTA’; July 2008- June 2012, ‘MTA adoption’; July 2012-June 2017 and ‘standardised MTA’; July 2017-July 2023. RRA was defined as adenomatous tissue detected at the first surveillance colonoscopy (SC1) and confirmed on histology. MTA was defined as complete application of snare-tip soft coagulation to the entire EMR defect margin. The primary outcome was to compare the RRA rate between the three time periods.</p><p><b><i>Results:</i></b> Over 15 years until July 2023, 1023 LNPCP ≥40mm in 1023 patients underwent EMR (median lesion size 50mm, IQR 20mm) of which 936 (91.5%) were successful. 836 patients (median lesion size 50mm, IQR 20) underwent SC1 at a median of 6 months (IQR 4). The rates of RRA in the pre-MTA, MTA-adoption and standardised-MTA phases were 20.3% (n=45/221), 19.2% (n=59/308) and 4.9% (n=15/307) respectively (p=<0.001). The rates of complete MTA in the pre-MTA, MTA adoption and standardised-MTA phases were 0, 37.7% (n=116/308) and 94.5% (n=290/307). 17 (5.5%) of cases within the standardised-MTA did not receive MTA due to difficult access (n=7), concern for stricture formation in fully circumferential LNPCP (n=8) or sedation-related issues (n=2). The rate of RRA in this group was 22.2% (n=4/18).</p><p><b><i>Conclusion:</i></b> Margin thermal ablation post-EMR of LNPCP ≥40mm (median size 50mm) significantly reduced the rate of RRA in a large, prospective cohort. When MTA was not applied, RRA was similar across the three time periods (p=0.1), indicating that the main impact on RRA reduction was the use of MTA with snare-tip soft coagulation, rather than a factor of EMR technique improvement over time.</p><p><b>455</b></p><p><b>Endoscopic ultrasound-guided gallbladder drainage compared to percutaneous cholecystostomy drainage: observational cohort study to assess safety and outcomes in non-operative candidates</b></p><p><b>Michael Chieng</b><sup>1</sup>, Rees Cameron<sup>2</sup>, Estella Johns<sup>2</sup>, Jerry Chin<sup>1</sup> and Frank Weilert<sup>1</sup></p><p><sup>1</sup><i>Health New Zealand, Hamilton, New Zealand;</i> <sup>2</sup><i>Health New Zealand, Wellington, New Zealand</i></p><p><i><b>Background and Aim</b>:</i> Cholecystectomy is the definitive treatment for cholecystitis but many patients are not surgical candidates or require bridging treatments before surgical candidacy. Percutaneous cholecystostomy (PC) is the current standard-of-care for achieving gallbladder decompression in non-surgical cholecystitis (NSC) but has risks of incomplete drainage, tube displacement, and disease recurrence. Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) is an emerging intervention that allows for insertion of wider drainage internal stents. We compared the outcomes of EUS-GBD with PC to determine safety, feasibility, and risks of re-intervention for both approaches in NSC.</p><p><b><i>Methods:</i></b> Outcomes of 19 EUS-GBD cases were retrospectively compared with a randomized sample of 27 PC cases performed between January 2010 and January 2023 at two tertiary referral centres in New Zealand. Demographic and outcome data were recorded including technical success, clinical success, length of hospital stay (LOS), adverse events, and re-interventions. Clinical success was defined by clinical improvement (resolution of fever, improvement in biochemistry, and symptoms) within 72 hours of the procedure. Median follow up of the cohorts was 24 months.</p><p><b><i>Results:</i></b> Age, gender and ethnicity data were balanced between groups. Technical and clinical success were complete in both EUS-GBD (n=19/19) and PC (n=27/27) cohorts, with no intra-procedural complications. EUS-GBD cases allowed for insertion of a wider diameter drainage device (10mm vs 3mm, p=<0.0001). There were significantly fewer adverse events in the EUS-GBD group (15.8% vs 51.9%, p=0.03) and proportionally fewer re-interventions, although this did not reach statistical significance (3/19 [15.8%] EUS-GBD vs 9/27 [33.3%] PC, p=0.21). EUS-GBD achieved significantly earlier discharge than the PC group (LOS: 4 days vs 12 days, p=0.006). EUS-GBD adverse events included cholangitis (1) and recurrent cholecystitis (2). PC adverse events included cholangitis (3), GB haemorrhage (1), PC displacement (2), PC blockage (2), recurrent cholecystitis (4), peritonitis (1), and pain requiring hospitalisation (1). There was no requirement for emergent surgery in the EUS-GBD cohort, however, three surgeries performed in the PC group related to complications of PC tube dysfunction.</p><p><b><i>Conclusion:</i></b> Compared with traditional PC for the treatment of cholecystitis in non-surgical candidates, EUS-GBD was technically comparable and safe with significantly fewer adverse events, reduced hospital stay, and lower need for emergent surgery.</p><p><b>463</b></p><p><b>Endoscopic ultrasound-guided gallbladder drainage for malignant biliary obstruction in patients who have failed ERCP and EUS-guided choledochoduodenostomy: safety and outcomes</b></p><p><b>Michael Chieng</b><sup>1</sup>, Rees Cameron<sup>2</sup>, Estella Johns<sup>2</sup>, Jerry Chin<sup>1</sup> and Frank Weilert<sup>1</sup></p><p><sup>1</sup><i>Health New Zealand, Hamilton, New Zealand;</i> <sup>2</sup><i>Health New Zealand, Wellington, New Zealand</i></p><p><b><i>Background and Aim:</i></b> Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) is described as a rescue therapy for patients with malignant biliary obstruction who fail biliary access with ERCP and/or EUS-guided choledochoduodenostomy (EUS-CDD). The traditional approach in this setting has been percutaneous transhepatic cholangiogram (PTC) but this carries risks. There have been few small series reporting outcomes of EUS-GBD for this indication. We report a multi-centre review of outcomes for malignant biliary drainage utilising EUS-GBD in non-surgical patients.</p><p><b><i>Methods:</i></b> A review of a prospectively collected cohort of 28 EUS-GBD cases was performed between January 2017 and January 2024 at two tertiary referral centres in New Zealand. A transduodenal approach was universal, using electrocautery-enhanced lumen apposing metal stents (LAMS), and anaesthesia-assisted sedation. Demographic and outcome data were recorded including technical success, clinical success, length of hospital stay (LOS), adverse events, re-interventions, and survival. Clinical success was defined by clinical improvement (resolution of fever, improvement in biochemistry, and symptoms) within 72 hours of the procedure. Re-interventions were split into early procedures, deemed necessary within 7 days, or late procedures occurring beyond 7 days. Median follow up was 36 months.</p><p><i><b>Result</b>s<b>:</b></i> Mean age of the cohort was 74 years (SD=9) with 9/28 (32.1%) females, and 5/28 (17.9%) Māori ethnicity. Pancreatic cancer was the most common diagnosis in 78.6% (22/28). Technical and clinical success was achieved in all 28 cases (100%). Stent size ranged from 8 – 15mm, with a median of 10mm. There were no procedural complications and no early re-interventions. Mean length of hospital stay was 4 days (SD=4). Adverse events were recorded in 14/28 (50%) with the majority (9/14, 64.3%) being infectious and managed conservatively with antibiotics; except for one patient who underwent PTC. There was one mortality 4 days following EUS-GBD, which was attributable to peritonitis from stent maldeployment of previously attempted EUS-CDD. EUS-GBD was performed as a rescue therapy in this setting and occurred without complication. 17.9% (5/28) cases required re-intervention over the follow up period. Recurrent biliary obstruction occurred in 3 cases (10.7%), with 1 case of cholangitis (3.57%), and stent obstruction (3.57%). These were treated with PTC (n=3), ERCP (n=1) and stent removal (n=1) respectively. Median survival was 135 days.</p><p><i><b>Conclusion</b>:</i> EUS-GBD is technically and clinically successful at treating malignant biliary obstruction offering a short hospital stay and excellent procedural adverse event profile. Late adverse events occurred as shown in previous series, but more than 82% of cases did not require any invasive reintervention. In a cohort of non-surgical candidates with advanced malignancy, planning a definitive treatment that avoids further intervention is paramount and EUS-GBD decompression appears to offer a safe, effective, and durable alternative to PTC in this setting.</p><p><b>468</b></p><p><b>Risk of bleeding after X-Tack closure of large mucosal defects in high risk patients: A case series</b></p><p><b>Peter Litwin</b><sup>1</sup>, Kelly Tam<sup>2</sup>, Kathryn Sharley<sup>1</sup>, Amanda H Lim<sup>1,3</sup>, Jeevinesh Naidu<sup>3</sup> and William Tam<sup>1,3</sup></p><p><sup>1</sup><i>Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>2</sup><i>Bond University, Robina, Australia;</i> <sup>3</sup><i>University of Adelaide, Adelaide, Australia</i></p><p><b><i>Background and Aim:</i></b> There is evolving literature on the risk of bleeding in large mucosal defects after polypectomy in patients on anticoagulant and antiplatelet medications. We report our experience of using X-tack, a through-the-scope suture-based device to close large, irregularly shaped mucosal defects after polypectomy of upper and lower gastrointestinal lesions in an elderly cohort with high rates of antithrombotic use.</p><p><b><i>Methods:</i></b> Data were collected from prospective cases performed by 2 endoscopists at three institutions. The X-Tack device was used to close large irregular mucosal defects and in circumstances where the endoscopist considered post-procedural bleeding risk to be high. Where relevant, antiplatelet medication was continued, whilst anticoagulation was held for 48 hours pre-procedure (or where renal function mandated otherwise) and re-commenced on the day of procedure.</p><p><b><i>Results:</i></b> Fourteen patients (median age: 74 years, IQR: 19) underwent the X-tack procedure. Defects were closed in the stomach (n=1), duodenum (n=1), proximal colon (n=9) and distal colon (n=3). Diathermy snare was utilised in mucosal resection in all but one case (duodenal adenoma). Median size of the lesions was 33mm (IQR: 31), with histology demonstrating 10 tubular or tubulo-villous adenomas, 2 sessile serrated lesions, 1 neuroendocrine tumour and 1 invasive adenocarcinoma. Nine of the fourteen patients were on anti-coagulant (n=4) or anti-platelet (n=5) therapy. Technical success of device deployment was 93%, with one device malfunctioning requiring closure using clips. Ten of the fourteen patients achieved defect closure using a single X-Tack device alone. Two patients required a second X-Tack kit and four (including patient with failed X-Tack deployment) required additional clips to close the respective mucosal defects. Clinical success was 86% over a median 10 month follow up period, with no incidents of perforation but two patients (one on anticoagulant, one on antiplatelet) did experience mild, delayed post-procedural bleeding at day 4 and day 8 respectively. Both patients were managed conservatively without the need for repeat endoscopy, blood transfusion, interventional radiology or surgery.</p><p><b>473</b></p><p><b>Safety and efficacy of Kaffes intraductal self-expanding metal stents in the management of post-liver transplant anastomotic strictures</b></p><p><b>Chee Lim</b><sup>1</sup>, Jonathan Ng<sup>1</sup>, Babak Sarraf<sup>1</sup>, Rhys Vaughan<sup>1,2</sup>, Marios Efthymiou<sup>1,2</sup>, Leonardo Zorron Cheng Tao Pu<sup>1,2</sup> and Sujievvan Chandran<sup>1,2</sup></p><p><sup>1</sup><i>Austin Health, Australia;</i> <sup>2</sup><i>Melbourne Medical School, The University of Melbourne, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Endoscopic management is the first-line therapy for post-liver-transplant anastomotic strictures. Although the optimal duration of treatment with plastic stents has been reported to be 8-12 months, data on safety and duration for metal stents in this setting is scarce. Due to limited access to endoscopic retrograde cholangiopancreatography (ERCP) during the coronavirus disease 2019 pandemic in our centre, there was a change in practice towards increased usage and length-of-stay of the Kaffes biliary intraductal self-expanding stent in patients with suitable anatomy. This was mainly due to the theoretical benefit of Kaffes stents allowing for longer indwelling periods compared to the traditional plastic stents. We aimed to compare the safety and efficacy profile of different stenting durations using Kaffes stents.</p><p><b><i>Methods:</i></b> Adult liver transplant recipients aged 18 years and above who underwent ERCP were retrospectively identified during a 10-year period through a database query. Unplanned admissions post-Kaffes stent insertion were identified manually through electronic and scanned medical records. The main outcome was the incidence of complications when stents were left indwelling for 3 months vs 6 months. Stent efficacy was calculated via rates of stricture recurrence between patients that had stenting courses for ≤ 120 d or > 120 d.</p><p><b><i>Results:</i></b> During the study period, a total of 66 ERCPs with Kaffes insertion were performed in 54 patients throughout their stenting course. In 33 ERCPs, the stent was removed or exchanged on a 3-month interval. No pancreatitis, perforations or deaths occurred. Minor post-ERCP complications were similar between the 3-month (abdominal pain and intraductal migration) and 6-month (abdominal pain, septic shower and embedded stent) groups - 6.1% vs 9.1% respectively, P = 0.40. All strictures resolved at the end of the stenting course, but the stenting course was variable from 3 to 22 months. The recurrence rate for stenting courses lasting for up to 120 d was 71.4% and 21.4% for stenting courses of 121 d or over (P = 0.03). There were 28 patients that were treated with a single ERCP with Kaffes, 21 with removal after 120 d and 7 within 120 d. There was a significant improvement in stricture recurrence when the Kaffes was removed after 120 d when a single ERCP was used for the entire stenting course (71.0% vs 10.0%, P = 0.01).</p><p><b><i>Conclusion:</i></b> Utilising a single Kaffes intraductal fully-covered metal stent for at least 4 months is safe and efficacious for the management of post-transplant anastomotic strictures.</p><p><b>490</b></p><p><b>The west catching up with the east: high-magnification NBI is an accurate tool for the diagnosis of gastric neoplasia in a western population</b></p><p><b>Edward Young</b><sup>1,2</sup>, Nicholas Wan<sup>1,2</sup>, Andrew Ruszkiewicz<sup>1,3</sup> and Rajvinder Singh<sup>1,2</sup></p><p><sup>1</sup><i>Lyell McEwin Hospital, Northern Adelaide Local Health Network;</i> <sup>2</sup><i>Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>SA Pathology, Adelaide, Australia</i></p><p><b><i>Introduction:</i></b> Gastric cancer is the third leading cause of cancer-related death worldwide.<sup>1</sup> In high-incidence countries such as Korea and Japan, nationwide gastric cancer screening programs have reduced the incidence of advanced gastric cancer by facilitating detection of lesions at an early stage amenable to endoscopic resection.<sup>2</sup> Accurate endoscopic prediction of histology and invasion depth is critical for guiding endoscopic or surgical resection techniques. In these high-incidence countries, high-magnification narrow band imaging (M-NBI) has been established as an effective form of advanced mucosal imaging for diagnosis and prediction of invasion depth.<sup>3, 4</sup> Data is lacking on the applicability of this technique in western populations where early gastric cancer is less frequently encountered.</p><p><b><i>Methods:</i></b> This is an analysis of a prospectively collected database of gastric lesions that were assessed and either biopsied or resected by an interventional endoscopist at a single Australian Public Hospital between 2009 and 2023. All lesions were assessed endoscopically using M-NBI and a determination made at the time of reporting whether the lesion was neoplastic or non-neoplastic, as well as histological prediction between adenoma, early gastric cancer, invasive adenocarcinoma and ‘other neoplastic’ lesions. This was then correlated with the final histology. 95% confidence intervals of classification statistics were obtained based on binomial proportions and a kappa statistic was calculated to assess the agreement between M-NBI histological prediction.</p><p><b><i>Results:</i></b> A total of 232 lesions in 183 patients were included in the final analysis, including 35 adenomas, 29 early gastric cancers, 6 invasive adenocarcinomas, 137 non-neoplastic lesions and 25 ‘other neoplastic’ lesions (including neuroendocrine tumours and lymphoma). For differentiating neoplastic versus non-neoplastic lesions, M-NBI had a sensitivity of 97.9% (CI 92.6-99.7%) and specificity of 97.1% (CI 92.7-99.2%), with a PPV of 98.52% (CI 94.8-99.8%) and NPV of 95.9% (CI 89.8-98.9%). The overall accuracy of M-NBI was 97.4% (CI 94.5-99.1%). M-NBI also had high specificity (97.1%, CI 92.7-99.2%) for identifying lesions suitable for endoscopic resection, with a PPV of 96.9% (CI 89.2-99.6%). The observed agreement between the M-NBI predicted histology and the final pathological diagnosis was 91.81% with a derived kappa statistic of 0.865, indicating excellent agreement.</p><p><b><i>Conclusion:</i></b> M-NBI can be used with a high degree of accuracy in western populations, equivalent to the accuracy demonstrated by experts in eastern countries. When used by a proceduralist trained in advanced mucosal imaging M-NBI is highly specific for identifying appropriate lesions for endoscopic resection.</p><p><b>References</b></p><p>\n 1. <span>Bray, F</span>, <span>Ferlay, J</span>, <span>Soerjomataram, I</span>, et al. <span>Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries</span>. <i>CA Cancer J Clin</i> <span>2018</span>; <span>68</span>: <span>394</span>-<span>424</span>.</p><p>\n 2. <span>Narii, N</span>, <span>Sobue, T</span>, <span>Zha, L</span>, et al. <span>Effectiveness of endoscopic screening for gastric cancer: The Japan Public Health Center-based Prospective Study</span>. <i>Cancer Sci</i> <span>2022</span>; <span>113</span>: <span>3922</span>-<span>3931</span>.</p><p>\n 3. <span>Kato, M</span>, <span>Kaise, M</span>, <span>Yonezawa, J</span>, et al. <span>Magnifying endoscopy with narrow-band imaging achieves superior accuracy in the differential diagnosis of superficial gastric lesions identified with white-light endoscopy: a prospective study</span>. <i>Gastrointest Endosc</i> <span>2010</span>; <span>72</span>: <span>523</span>-<span>9</span>.</p><p>\n 4. <span>Kobara, H</span>, <span>Mori, H</span>, <span>Fujihara, S</span>, et al. <span>Prediction of invasion depth for submucosal differentiated gastric cancer by magnifying endoscopy with narrow-band imaging</span>. <i>Oncol Rep</i> <span>2012</span>; <span>28</span>: <span>841</span>-<span>7</span>.</p><p><b>500</b></p><p><b>Intraductal papillary mucinous neoplasm of bile duct: A case report of the challenges of diagnosis and management</b></p><p><b>Michael Christmas</b><sup>1</sup>, Wilson Siu<sup>1</sup>, Perveen Aslam<sup>1</sup>, Shivendra Lalloo<sup>1</sup>, Mitali Fadia<sup>1</sup>, Ngee-Soon Lau<sup>1</sup> and Vipul Aggarwal<sup>1,2</sup></p><p><sup>1</sup><i>ACT Health, Canberra, Australia;</i> <sup>2</sup><i>Australian National University, Canberra, Australia</i></p><p><b><i>Introduction:</i></b> Intraductal papillary mucinous neoplasm of the bile duct (IPMN-B) is a rare tumour arising from biliary epithelial tissue and recognized as a precursor lesion to cholangiocarcinoma. IPMN-B are characterized by intraluminal hypersecretion of mucin that can intermittently impede bile flow, leading to repeated episodes of cholangitis and biliary obstruction<sup>1</sup>. Diagnosis can be challenging particularly due to the lack of defining features on imaging<sup>2</sup>. Surgical resection remains the definitive treatment<sup>3</sup>. Here we present a case of the endoscopic challenges prior to surgical resection.</p><p><b><i>Case presentation:</i></b> A 78 year old male originally from Laos, with a background of non-insulin dependent diabetes, chronic obstructive pulmonary disease and transient ischaemic attack. Presented to our institution with cholangitis, serum bilirubin 190 umol/L and CRP 55mg/L. This is in the setting of recent admission one month earlier with painless jaundice (serum bilirubin 50 umol/L) where he was treated as cholangitis and his initial investigation had not revealed a cause for biliary obstruction. With improving bilirubin (39 umol/L) and clinical improvement, he was discharged with plan for ongoing outpatient investigations. On admission he was commenced on antibiotics and similar to his initial, Magnetic Resonance Cholangiopancreatography (MRCP) revealed dilated and tortuous intrahepatic biliary ducts in both lobes of the liver. No choledocholithiasis nor mass lesion was seen. An initial Endoscopic Retrograde Cholangiopancreatography (ERCP) removed a significant amount of pus from the CBD, but no stones or sludge, a 10 French 7 cm straight plastic stent was placed. Subsequent CT imaging did not show decompression of the intrahepatic ducts, there was no significant decline in the serum bilirubin (206 umol/L). This prompted repeat ERCP for placement of longer stents into the Left Intrahepatic Duct (LIHD) and Right Intrahepatic Duct (RIHD) raising possibility of RIHD stricture. We opted to insert 10 Fr 10cm and 10 Fr 12cm straight plastic stents, respectively. Despite these measures, the biliary obstruction persisted (bilirubin 291 umol/L). The team then opted for a RIHD percutaneous transhepatic cholangiostomy (PTC) for drainage of the biliary system. There was initially reasonable output from the PTC and decline in serum bilirubin (256 umol/L) that plateaued with time, a repeat CT scan showed the PTC drain to be in an appropriate position. The decision was then made to proceed with a combined gastroenterology and interventional radiology case. Endoscopic technique: Through the existing right Percutaneous Transhepatic Biliary Drainage (PTBD), a long 0.035 inch wire was introduced into the periampullary duodenum for endoscopic capture. The original PTC drain was removed and replaced by 10 French Cook sheath. ERCP was performed with removal of the 2 previous plastic stents and capture of the wire. With balloon sweep, copious drainage of viscous mucopurulent material was expelled through the ampulla. Interval cholangiogram revealed partial clearing of filling defect in the CHD/CBD with improved contrast passage. Subsequent over the wire passage of Spyglass choledochoscope system confirmed accumulation of mucoid material at the hilar confluence and CHD, and a flat, villous lesion was revealed at the confluence of the right liver sectoral ducts, the anterior more affected. Several biopsy samples obtained with spybite microforceps with biopsies confirming IPMN-B with low-grade dysplasia. Finally, a 15 cm 10 Fr plastic stent was deployed over the PTC placed guidewire, the rostral end shown to be favourably positioned in the anterior sectoral duct on final cholangiogram obtained through upsized 12 French internal/external drain. The latter also demonstrated considerable clearance of prior mucoid filling defects in the CHD/CBD. Post procedure, the patient’s bilirubin remained stubbornly elevated (200 umol/L). A flushing technique of the PTC was employed where a flush of 10mL normal saline was delivered every 8 hours and increasing to every 6 hours finally resulting in declining bilirubin (84 umol/L at discharge). The patient’s family was taught how to continue this until the patient’s planned surgery. The patient did not require any further admissions to hospital prior to having his extended right hemihepatectomy.</p><p><b><i>Conclusions:</i></b> Technical challenges exist with the diagnosis and early management of IPMN B. Techniques in diagnosis and therapy to alleviate the burden of mucinous obstruction prior to surgical resection are described here.</p><p><b>References</b></p><p>\n 1. <span>Yeh, TS</span>, et al. <span>Cholangiographic spectrum of intraductal papillary mucinous neoplasm of the bile ducts</span>. <i>Ann Surg.</i> <span>2006</span> Aug; <span>244</span>(<span>2</span>): <span>248</span>-<span>53</span>.</p><p>\n 2. <span>Kung, JWC</span>, et al. <span>Intraductal papillary neoplasm of the bile duct: the role of single-operator cholangioscopy</span>. <i>VideoGIE.</i> <span>2017</span> Dec 13; <span>3</span>(<span>2</span>): <span>55</span>-<span>57</span>.</p><p>\n 3. <span>Ohtsuka, M</span>, et al. <span>Intraductal papillary neoplasms of the bile duct</span>. <i>Int J Hepatol.</i> <span>2014</span>; <span>2014</span>: <span>4590</span>-<span>91</span>.</p><p><b>505</b></p><p><b>Cold vs hot snare endoscopic mucosal resection for large (≥15mm) flat non-pedunculated colorectal polyps: A randomized controlled trial</b></p><p><b>Timothy O'Sullivan</b><sup>1,2</sup>, Oliver Cronin<sup>1,2</sup>, Arnout Van Hattem<sup>3</sup>, Francesco V Mandarino<sup>1</sup>, Julia Gauci<sup>1</sup>, Clarence Kerrison<sup>1</sup>, Anthony Whitfield<sup>1,2</sup>, Sunil Gupta<sup>1,2</sup>, Eric Y Lee<sup>1</sup>, Stephen Williams<sup>1</sup>, Nicholas Burgess<sup>1,2</sup> and Michael J Bourke<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;</i> <sup>2</sup><i>Westmead Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, Netherlands Cancer Institute, Amsterdam, Netherlands</i></p><p><b><i>Background and Aim:</i></b> Endoscopic mucosal resection (EMR) is standard of care for the management of large (≥20mm) non-pedunculated colonic polyps (LNPCPs). Its efficacy and cost effectiveness were limited by recurrence. Margin thermal ablation (MTA) to the post-EMR defect, has greatly mitigated this problem. However, electrocautery-related complications of delayed bleeding and perforation incur significant morbidity. Cold snare polypectomy is effective and safe for the resection of small polyps with negligible recurrence rates. Application of cold snare resection to LNPCPs, while an attractive alternative, lacks high-quality evidence. We conducted a randomized trial to compare the efficacy and safety of cold EMR (C-EMR) to conventional (H-EMR).</p><p><b><i>Methods:</i></b> A prospective single-centre randomized controlled trial was conducted at an Australian tertiary referral centre for flat, 15-50mm adenomatous LNPCPs referred for endoscopic resection. Prior to resection, eligible LNPCPs were randomly assigned to EMR using a dedicated cold snare or conventional H-EMR with margin thermal ablation (control). First surveillance colonoscopy (SC1) was conducted 6 months following resection. Scars were evaluated with high-definition white-light, narrow-band imaging and biopsy. The primary outcome was endoscopically visible and/or histologically confirmed recurrence at SC1. Secondary outcomes were clinically significant post-EMR bleeding (CSPEB), delayed perforation and technical success.</p><p><b><i>Results:</i></b> 920 LNPCPs were referred for endoscopic resection between November 2019-September 2023. 177 LNPCPs in 177 patients were randomized to either the C-EMR arm (n=87) or H-EMR arm (n=90). Treatment groups were equivalent with no significant difference in lesion size or technical success (86/87 (98.9%) vs 90/90 (100%); p=0.31). One C-EMR required conversion to H-EMR due to unexpected submucosal fibrosis. Following exclusions, 147 LNPCPs undertook SC1 (77 C-EMR, 70 H-EMR). On intention to treat and per protocol analysis, recurrence was significantly greater in C-EMR (16/87, 18.4% vs 1/90, 1.1%; RR 16.6, 95%CI 2.24-122; p<0.001 and 16/76 (21.1%) vs 1/70 (1.4%); p<0.001 respectively). Significant deep mural injury (27/90 (30%) vs 0; p<0.001) and delayed perforation (1/90 (1.1%) vs 0; p=0.32) only occurred in the H-EMR group. CSPEB and intraprocedural bleeding were significantly greater in the H-EMR arm (7/90 (7.8%) vs 1/87 (1.1%); RR 6.77, 95% CI 0.85-53.9; p = 0.034 and 12/90 (13.3%) vs 1/87 (1.1%); p=0.002 respectively).</p><p><b><i>Conclusion:</i></b> Compared to conventional H-EMR, C-EMR for flat, adenomatous LNPCPs, demonstrates superior safety with equivalent technical success. However, endoscopic recurrence is significantly greater for cold snare resection and is currently a limitation of the technique.</p><p><b>508</b></p><p><b>Multicentre prospective evaluation of the Hot Spaxus lumen apposing metal stent for EUS-guided drainage of pancreatic walled off necrosis</b></p><p><b>Tony He</b><sup>1</sup>, Nicholas Burgess<sup>2</sup>, Milan S Bassan<sup>3</sup>, Benedict Devereaux<sup>4</sup> and Bronte Holt<sup>1</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Melbourne;</i> <sup>2</sup><i>Westmead Hospital;</i> <sup>3</sup><i>Liverpool Hospital, Sydney;</i> <sup>4</sup><i>Royal Brisbane and Women's Hospital, Brisbane, Australia</i></p><p><b><i>Background and Aims:</i></b> Endoscopic ultrasound (EUS)-guided drainage of pancreatic walled off necrosis (WON) with cautery-assisted lumen-apposing metal stents (LAMS) has a high technical and clinical success rate of 53-100%<sup>1,2</sup>. This study aims to prospectively evaluate a new cautery-assisted LAMS (Hot Spaxus, Taewoong Medical, Korea) to inform on the safety and efficacy of the device in the treatment of WON.</p><p><b><i>Methods:</i></b> This is a prospective, multicenter cohort study conducted at four tertiary care hospitals in Australia, including patients with symptomatic pancreatic WON requiring EUS-guided drainage. Procedures were performed with anaesthetic support and intravenous antibiotics, under EUS and fluoroscopy control. Decision for and timing of direct endoscopic necrosectomy was based on degree of necrosis. LAMS were removed at 4 weeks, with clinical and radiologic follow up at 1 and 3 months. Primary outcomes were technical success, intra-procedural and 30-day major adverse events. Secondary outcomes included clinical success, stent-related complications, procedural time and number of reinterventions.</p><p><b><i>Results:</i></b> 20 patients (mean (SD) age 54.6 (15.6); females 55%; mean (SD) WON size 12.8cm (4.6); 10% had >50% solid necrosis, 55% had 21-50% necrosis, 35% had <20% necrosis) were enrolled and included in the final analysis. Primary indication for EUS-guided drainage was abdominal pain (80%). Technical success was 100% with no intra-procedural complications. One patient (5%) had a splenic artery pseudoaneurysm bleed 29 days post-LAMS insertion, treated by radiologically guided embolization. The median (IQR) time for stent deployment was 10 minutes (5, 10). The mean (SD) number of endoscopic interventions to clear the cavity was 2.95 (1.7). The LAMS was removed at a mean (SD) time of 29.3 days (6.5), replaced by double pigtail stents in 95% of patients for long term drainage. 10% of patients had a likely disconnected duct on EUS or CT/MRI. At 3-months, 95% of patients had resolution of pre-intervention symptoms and 90% had WON resolution on CT/MRI.</p><p><b><i>Conclusion:</i></b> The new cautery-assisted LAMS has a high technical and clinical success rate for the treatment of pancreatic WON, with no intra-procedural complications, and a similar post-procedural adverse event profile to alternative devices. Randomized prospective studies comparing the available cautery-assisted LAMs in the treatment of pancreatic WON are required.</p><p><b>References</b></p><p>\n 1. <span>Chandrasekhara, V</span>, <span>Barthet, M</span>, <span>Devière, J</span>, et al. <span>Safety and efficacy of lumen-apposing metal stents versus plastic stents to treat walled-off pancreatic necrosis: systematic review and meta-analysis</span>. <i>Endosc Int Open.</i> <span>2020</span>; <span>8</span>: <span>E1639</span>–<span>E1653</span>.</p><p>\n 2. <span>Baron, TH</span>, <span>DiMaio, CJ</span>, <span>Wang, AY</span>, <span>Morgan, KA</span>. <span>American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis</span>. <i>Gastroenterology</i>. <span>2020</span>; <span>158</span>(<span>1</span>): <span>67</span>-<span>75</span>.e1.</p><p><b>509</b></p><p><b>Impact of margin thermal ablation after endoscopic mucosal resection of large (≥20mm) non-pedunculated colonic polyps on long term recurrence</b></p><p><b>Timothy O'Sullivan</b><sup>1,2</sup>, Francesco V Mandarino<sup>1</sup>, Julia Gauci<sup>1</sup>, Anthony Whitfield<sup>1,2</sup>, Clarence Kerrison<sup>1</sup></p><p>Catarina Neto do Nascimento, Sunil Gupta<sup>1,2</sup>, Oliver Cronin<sup>1,2</sup>, Anthony Sakiris<sup>1</sup>, Juan F Prieto Aparicio<sup>1</sup>, Sophie Arndtz<sup>3</sup>, Gregor Brown<sup>3</sup>, Spiro Raftopoulos<sup>4</sup>, David Tate<sup>5,6</sup>, Eric Y Lee<sup>1</sup>, Stephen Williams<sup>1</sup>, NICHOLAS BURGESS<sup>1,2</sup>, MICHAEL J BOURKE<sup>1,2</sup></p><p><sup>1</sup><i>Department of Gastroenterology and Hepatology, Westmead Hospital, Australia;</i> <sup>2</sup><i>Westmead Clinical School, University of Sydney, Sydney, Australia;</i> <sup>3</sup><i>Department of Gastroenterology and Hepatology, The Alfred Hospital, Melbourne, Australia;</i> <sup>4</sup><i>Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia;</i> <sup>5</sup><i>Department of Gastroenterology and Hepatology, University Hospital of Ghent, Ghent, Belgium;</i> <sup>6</sup><i>University of Ghent, Ghent, Belgium</i></p><p><b><i>Background and Aim:</i></b> EMR is the standard of care for the management of large (≥20mm) non-pedunculated colonic polyps (LNPCPs). However, its efficacy and cost effectiveness, are limited by recurrence and the necessity for scheduled surveillance. Consequently, current surveillance intervals are conservative. Margin thermal ablation (MTA) after EMR for LNPCPs has dramatically reduced the incidence of recurrence at first surveillance colonoscopy at six-months (SC1). If this effect is durable, then subsequent surveillance intervals in patients who have been cleared of synchronous polyps could be substantially lengthened. We prospectively evaluated long-term surveillance outcomes in a cohort of LNPCPs that have undergone MTA.</p><p><b><i>Methods:</i></b> Consecutive patients with LNPCPs undergoing EMR and MTA from four academic endoscopy centres were prospectively recruited. All patients that underwent successful endoscopic resection received SC1 six months post resection. EMR scars were carefully evaluated with high-definition white light, narrow band imaging with near focus and biopsy. In the absence of recurrence, second surveillance (SC2) colonoscopy was conducted at a subsequent interval of 12 months with the scar evaluation process repeated. A historical control arm was generated from LNPCPs that underwent EMR without MTA. The primary outcome was recurrence at SC2 in all LNPCPs with a recurrence-free scar at SC1.</p><p><b><i>Results:</i></b> 1315 LNPCPs referred for EMR were enrolled over 90 months until October 2022. Following exclusions, 1148 LNPCPs underwent EMR with complete MTA. 238 LNPCPs formed the control arm from January 2012-May 2016. 852 LNPCPs underwent SC1. 31 additional synchronous LNPCPs were cleared at this procedure. 26/852 (3.1%) LNPCPs demonstrated recurrence. 472 LNPCPs free of recurrence at SC1 underwent SC2 at a mean interval of 23.1 months (95%CI 22.1-24.2) after the index EMR. 471 demonstrated a bland scar without recurrence. Only one recurrence occurred related to a 0-IIa+Is 20mm granular TVA located on the ileocaecal valve. Recurrence at SC2 was significantly less in the MTA arm vs controls (1/472 (0.2%) vs 9/238 (3.8%); p <0.001).</p><p><b><i>Conclusion:</i></b> LNPCPs that have undergone successful EMR with MTA and are free of recurrence at SC1 are very unlikely to develop recurrence in subsequent surveillance out to 2 years. Following EMR of LNPCPs with MTA, patients who are cleared of synchronous neoplasia and demonstrate no recurrence after careful scar examination, can potentially undergo next surveillance in 3-5 years. Such an approach would reduce costs and enhance patient compliance.</p><p><b>515</b></p><p><b>Efficacy and safety of EUS-guided drainage of post-surgical fluid collections</b></p><p>Michael MacIsaac<sup>1</sup>, Tony He<sup>1</sup>, Tulio Soares<sup>1</sup>, Fiona Jones<sup>1</sup>, Lena Tabbaa<sup>2</sup>, Daniel Croagh<sup>2</sup> and Bronte Holt<sup>1</sup></p><p><sup>1</sup><i>St Vincent's Hospital Melbourne, Australia;</i> <sup>2</sup><i>Monash Health, Melbourne, Australia</i></p><p><b><i>Introduction:</i></b> Post-surgical fluid collections (PSFCs) are a common complication of gastrointestinal (GI) surgery and are usually managed by percutaneous drainage. Emerging data suggests that endoscopic ultrasound (EUS) guided drainage of PSFCs may be a safe and effective alternative, which can similarly be performed early after PSFC development (≤4 weeks).</p><p><b><i>Methods:</i></b> Retrospective, multi-centre cohort study of all patients referred for EUS-guided drainage of symptomatic PSFCs after hepatobiliary, upper GI or colorectal surgery at two tertiary referral centres in Melbourne, Australia over a 7-year period from 1<sup>st</sup> January 2016 to 31<sup>st</sup> December 2022. Patients were identified using hospital databases, multi-disciplinary meeting records and review of all EUS cases, with electronic medical record data extraction. Primary outcome measures were technical success (ability to access and drain a PSFC by placement of a transmural stent), clinical success (complete clinical resolution of symptoms and reduction/resolution of PSCF on CT at 3 months) and rate of adverse events, with major adverse events defined as grade III or above on the Clavien Dindo Classification.</p><p><b><i>Results:</i></b> 42 patients were referred for EUS-guided drainage of PSFCs (median age 61 years (IQR, 46–71); 25 (60%) male). The most common index surgery was pancreatic (N=19, 45%) and the primary indication for drainage was sepsis (N=29, 69%). Mean collection size was 6.1cm (range 1.7–13.5cm). EUS was performed at a median of 30 days (IQR, 19-69 days) post-surgery; 19 (45%) were done in ≤4 weeks of PSFC development. EUS-guided drainage was attempted in 34 (81%) patients with 100% technical success. Eight patients were excluded at EUS due to unsuitable collection morphology (PSFC too small or not identified, N=5; immature PSFC wall, N=2; PSFC not abutting the GI lumen, N=1). Clinical success was achieved in 33/34 (97%) patients who underwent EUS-guided drainage; one patient had symptom resolution post drainage however follow up CT showed an increase in the size of the PSFC. A single EUS-guided drainage was performed in 29 patients; 5 patients required >1 endoscopic procedure (range 2–4). There were no intra-procedural complications. Nine (26%) post-procedural adverse events occurred, of which three were classified as major adverse events.</p><p><b><i>Conclusions:</i></b> EUS-guided drainage of PSFCs is technically feasible, can be safely performed early following PSFC formation in a significant proportion of patients and achieves high rates of clinical success with few major adverse events. It is a minimally invasive alternative to percutaneous drainage, avoiding the need for an external drain with attendant risk of blockage, dislodgement, and infection. EUS-guided drainage should be considered as a therapeutic option for patients with PSFCs after GI surgery.</p><p><b>534</b></p><p><b>Endoscopic ultrasound related adverse events at a tertiary hospital</b></p><p><b>Deepu David</b><sup>1,2</sup>, Michael Ma<sup>2</sup>, Vanoo Jayasekeran<sup>2</sup> and Andre Chong<sup>2</sup></p><p><sup>1</sup>Sunshine Coast University Hospital Sunshine coast, Australia; <sup>2</sup>Fiona Stanley hospital, Perth, Australia</p><p><b>Background and Aim:</b> Endoscopic ultrasound (EUS) is a commonly used procedure in Gastroenterology. Although EUS complication rate is presumed to be low, scarce data exists from Australia. Aim of this study was to assess the complication rates and the factors influencing the complications in patients undergoing EUS.</p><p><b>Methods:</b> A retrospective review of all adult patients who underwent EUS examination between Dec 2014 and June 2022 June were conducted. Patients needing inpatient admission within 5 days of undergoing the procedure were included in the study. Data including the demographics, details of the procedure and the adverse events were collected.</p><p><b>Results:</b> A total of 1868 patients had undergone EUS during the period. 135 patients needed admission within 5 days post-procedure after undergoing EUS-guided FNA. 21 patient admissions were for complications related to the EUS procedure. The most common complication was acute pancreatitis, and all cases were mild in severity (33.33%). One patient with pancreatitis had undergone a concomitant ERCP, along with EUS. Other complications noted were duodenal ulcer-associated hematemesis, duodenal perforation, retroperitoneal hematoma, splenic vein thrombosis, mucinous cyst fluid leak into the peritoneal cavity, and cholangitis. A trainee was present in less than one-third of the procedures (31.5%) with complications. None of the patients with complications were on regular anticoagulants peri-procedure. There was no mortality associated with any of the complications.</p><p><b><i>Conclusion:</i></b> The incidence of complications was extremely low. The most common complication was acute pancreatitis.</p><p><b>Table 1</b>\n \n </p><p><b>550</b></p><p><b>Show me your PEC: Endoscopic ultrasound, histological features and management of an exceedingly rare pancreatic perivascular epithelioid cell tumour (PEComa)</b></p><p>Angus Ferguson<sup>1,2</sup>, <b>Daniel Saitta</b><sup>1</sup>, Sharon Wallace<sup>1,3</sup> and Dileep Mangira<sup>1,3</sup></p><p><sup>1</sup><i>Grampians Health Ballarat, Ballarat, Australia;</i> <sup>2</sup><i>Western Health, Australia;</i> <sup>3</sup><i>Dorevitch Pathology, Melbourne, Australia</i></p><p><b><i>Background:</i></b> Perivascular Epithelioid Cell tumours (PEComas) are rare mesenchymal tumours, including angiomyolipomas, clear cell ‘sugar’ tumours, and lymphangioleiomyomas. These tumours are usually benign but may occasionally be malignant (1). Pancreatic PEComas are extremely rare, with only 35 cases reported in the literature as of 2024 (2). They are 4.5 times more common in women and typically present with vague or no symptoms (1). Noteworthy features of this case include utilisation of endoscopic ultrasound (EUS) in diagnosis of a PEComa.</p><p><b><i>Case:</i></b> A 45-year-old woman, with a history of hemithyroidectomy, uterine fibroids, and depression, was admitted following a motor vehicle accident. An abdominal CT scan revealed a 14mm incidental arterial hyperenhancing focus at the head of the pancreas, initially suspected to be a neuroendocrine tumour. Follow-up MRI confirmed a T2 hyperenhancing 14x12.2x13.5mm hypervascular lesion. Serum investigations including FBE, UEC’s, LFTs and TFT’s, and tumour markers Chromogranin A, Ca 19-9, 5-HIAA were also within normal limits. EUS described a 16x14mm well-circumscribed mass at the head of the pancreas and subsequent fine needle aspiration biopsies showed epithelioid cells with glycogen-rich cytoplasm. Immunohistochemistry was positive for SMA, Caldesmon, HMB-45, Melan-A, and PR. The Ki-67 index was approximately 10%. Due to anatomical location, rarity of tumour and uncertain future malignant potential, this patient underwent a curative pancreaticoduodenectomy without adjuvant chemo/radiotherapy. She is now 6 months post procedure without evidence of recurrence.</p><p><b><i>Discussion:</i></b> The immunohistochemical profile and morphological features confirmed the diagnosis of PEComa. Whilst PEComas are commonly benign some have malignant potential. The main clinical challenge lies in differentiating PEComas malignant potential to determine further management. Typically, classification utilises Folpe et al.’s criteria which assesses the presence of 6 features: Size >5cm; Infiltrative lesion; High nuclear grade and cellularity; Mitotic rate ≥1/50 HPF; Presence of necrosis; Presence of vascular invasion (3). The presence of 2 or more of these ‘worrisome’ features indicates a ‘Malignant' lesion; one feature indicates ‘Uncertain Malignant Potential’ and no features suggests a ‘Benign’ lesion. Given the rarity of pancreatic PEComas treatment guidelines are not well-established. However, surgical excision remains the standard approach, as seen in this case.</p><p><i><b>Conclusion</b>:</i> This case highlights an extremely rare differential of a pancreatic mass lesions. Early sampling and immunohistochemical analysis are crucial for accurate diagnosis and determining malignancy potential. This case emphasizes the role of endoscopic ultrasound in diagnosing this rare condition. Given their rarity, patient centred multidisciplinary management is essential. Surgical excision with pancreaticoduodenectomy is an extremely invasive procedure, so prior accurate diagnosis is a critical step before subjecting patients to such an invasive surgical approach. An ability to recognise and potential monitor for malignant radiological, EUS, and/or fine needle aspirate features may represent a viable alternative to surgery given their predominantly benign nature.</p><p><b>References</b></p><p>\n 1. <span>Bleeker, JS</span>, <span>Quevedo, JF</span>, <span>Folpe, AL</span>. <span>“Malignant” Perivascular Epithelioid Cell Neoplasm: Risk Stratification and Treatment Strategies</span>. <i>Sarcoma</i> <span>2012</span>; <span>2012</span>: <span>1</span>–<span>12</span>.</p><p>\n 2. <span>Sixto, MN</span>, <span>Iglesias, RC</span>, <span>Fernández, SE</span>, <span>Pereira, CR</span>, <span>Santos, RS</span>. <span>Pancreatic PEComa, a not so uncommon neoplasm? Systematic review and therapeutic update</span>. <i>Gastroenterol Hepatol</i> <span>2024</span>; <span>47</span>: <span>93</span>-<span>100</span>.</p><p>\n 3. <span>Folpe, AL</span>, <span>Mentzel, T</span>, <span>Lehr, HA</span>, <span>Fisher, C</span>, <span>Balzer, BL</span>, <span>Weiss, SW</span>. <span>Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature</span>. <i>Am J Surg Pathol</i> <span>2005</span>; <span>29</span>: <span>1558</span>–<span>1575</span>.</p><p><b>583</b></p><p><b>Outcomes of endoscopic resection of gastro-oesophageal junction high grade dysplastic and adenocarcinoma lesions</b></p><p><b>David Law</b>, Marcus Chin and Niroshan Muwanwella</p><p><i>Royal Perth Hospital, Perth, Australia</i></p><p><b><i>Background and Aim:</i></b> The incidence of oesophageal adenocarcinoma has been increasing in recent years with Barrett’s oesophagus being the main identified precursor. The gastro-oesophageal junction (GOJ) has a high rate of oesophageal adenocarcinoma. Defining the GOJ can be difficult with guidelines such as the Kyoto consensus proposed to help identification. Similarly, guidance on the surveillance of GOJ pre-cancerous lesions lacks clarity in existing Barrett’s oesophagus screening protocols. We reviewed the outcomes and histology of endoscopic resected GOJ lesions to identify whether pre-cancerous changes were present, which could help guide endoscopic screening of the GOJ.</p><p><b><i>Methods:</i></b> Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) of GOJ lesions performed from May 2013 to December 2023 were captured through the local endoscopy reporting programme ProcRep. Details including patients’ characteristics, histology reports and follow-up procedures were obtained via electronic records. Patients with histology showing high grade dysplasia (HGD) or adenocarcinoma were included in the study, whilst non-dysplastic lesions were excluded.</p><p><b><i>Results:</i></b> A total of 27 patients received endoscopic resection for GOJ lesions with HGD or adenocarcinomas, 13 underwent EMR and 14 underwent ESD. 15 of the 27 patients had T1a lesions, none of whom developed recurrence. 6 patients had T1b lesions, 5 proceeded with oesophagectomy or chemoradiotherapy. The remaining 1 patient declined further treatment, with no local recurrence on surveillance endoscopies. 13 patients were known with Barrett’s oesopahgus prior endoscopic resection, all of whom had short segment Barrett’s oesophagus. Of the remaining 14 patients, 7 had resection histology showing Barrett’s dysplastic changes, whilst 7 had no features of Barrett’s oesophagus.</p><p><b><i>Conclusion</i></b>: Patients in our study achieved high clinical success from endoscopic resection with no case of recurrence. The majority of patients in our cohort had preceding Barrett’s oesophagus. However, 25.9% were noted with Barrett’s on histology only and another 25.9% had no Barrett’s oesophagus on endoscopy or histology. This highlights the importance of a thorough examination of the GOJ even in the absence of overt Barrett’s oesophagus. Further studies should be carried out to review the histology of GOJ adenocarcinomas without Barrett’s mucosal changes, to provide improved guidance on the screening of the GOJ and identifying pre-cancerous lesions.\n\n </p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":null,"pages":null},"PeriodicalIF":3.7000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16696","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16696","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
16
Early experience with endoscopic submucosal dissection at Austin Health
Sitong Chen1, Sujievvan Chandran1,2,3, Leonardo Zorron Cheng Tao Pu2,3, Nicholas Dalkie3, Rhys Vaughan1,2,3 and Marios Efthymiou1,2,3
1Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Parkville, Australia;2Liver Transplant Unit, Austin Health, Heidelberg, Australia;3Department of Gastroenterology and Hepatology, Austin Health, Melbourne, Australia
Background and Aim: Endoscopic submucosal dissection (ESD) is a minimally invasive endoscopic procedure which employs en-bloc dissection technique to remove premalignant or early malignant gastrointestinal lesions. In Japan, ESD is considered as first line treatment for early gastrointestinal neoplasms, yet the wide adoption of ESD in the West has been slow. Barriers include the technical difficulty of ESD, lower prevalence of early gastric cancer in the West, and the lack of training opportunities. We know that gastric location is the easiest location to start training in ESD whereas colorectal ESD is more challenging. The aim of this study was to assess the early experience with ESD at Austin Health.
Methods: A retrospective analysis was conducted on 31 consecutive gastrointestinal lesions in 27 patients who underwent ESD from June 2020 to April 2023 at Austin Health, Melbourne Australia. Clinical and procedural data, complications, and the efficacy and efficiency of the ESD procedure were evaluated.
Results: Twenty-seven patients (12 females and 15 males) were enrolled in the study, with a mean age of 72.0 years. Overall, thirty-one lesions were resected, including 16 gastric lesions, 6 oesophageal lesions and 9 colorectal lesions. The mean size of the lesions was 35.8mm and the mean resected base area was 12.0cm2. In the total cohort, en-bloc resection rate was 96.8%. Final ESD histology upstaged the initial diagnosis in four lesions based on pre-ESD pinch biopsies and imaging. Eleven malignant lesions were found in the final pathology. Six complications were reported in our study, including two cases of intraoperative perforation and four cases of delayed bleeding (all the complications were managed medically/endoscopically). The mean hospital stay was 1.6 days for all patients, and 19 patients were discharged after an overnight admission.
Conclusion: ESD is an effective and safe treatment for gastrointestinal neoplasms in an Australian tertiary centre and our early treatment outcomes were comparable to recently published large study data. Outcomes are likely to progressively improve with further experience.
30
Intrathoracic cholecystitis managed with endoscopic gallbladder drainage
Andrea Huang1,4, Thomas Williams1,4, Nivene Saad2,4, Adam Frankel3,4, Zaki Hamarneh1, Shwan Karim1 and Adrian Maher1,4
1Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;2Department of Radiology, Princess Alexandra Hospital, Brisbane, Australia;3Department of Upper Gastrointestinal Surgery, Princess Alexandra Hospital, Brisbane, Australia;4Faculty of Medicine, University of Queensland, Brisbane, Australia
Introduction: Intrathoracic acute cholecystitis is a presentation that typically occurs in the context of a prior history of a traumatic diaphragmatic hernia. Cholecystectomy and hernia repair has been the mainstay of management in previous case reports, either via open surgical, laparoscopic or thoracoscopic techniques. However not all patients may be suitable for major operations and alternative management options, such as endoscopic ultrasound-guided approaches, are required.
Case Report: This case report describes that of a 67 year old female who presented with intrathoracic acute cholecystitis complicated by a type 1 myocardial infarction. In the months prior, she had received neoadjuvant chemotherapy and immunotherapy for a poorly-differentiated gastro-oesophageal adenocarcinoma and was awaiting re-evaluation for surgical resection. Her staging scans had demonstrated a large diaphragmatic hernia presumed secondary to a car crash in her youth. The hernia contained the right lobe of the liver, hepatic flexure, first and secondary part of the duodenum, and the gallbladder. Initial management of the intrathoracic acute cholecystitis with antibiotics was unsuccessful. Supine laparoscopy with both abdominal and right thoracic ports was attempted, however the gallbladder could not be visualized. Given her recent medical issues, major open surgery was avoided. Endoscopic ultrasound-guided internal drainage of the gallbladder was successfully achieved using a 10mm x 10mm lumen apposing metal stent, with visible passage of stones and resolution of cholecystitis.
57
Endoscopic ultrasound-guided tissue acquisition with rapid on-site evaluation for the evaluation of solid pancreatic lesions: A retrospective observational study at a tertiary level Australian Hospital
Josh McCarthy, Stephen Philcox and Donna Gillies
John Hunter Hospital, Newcastle, Australia
Background: Pancreatic cancer is common and associated with a high mortality. The preoperative diagnosis of solid pancreatic lesions can be challenging however EUS-guided tissue acquisition offers a minimally invasive and accurate diagnostic procedure that has been established at our institution since 2010.
Aim: The objective of this study is to review the diagnostic accuracy of EUS-guided tissue acquisition of solid pancreatic lesions at our institution and to report associations with inaccurate results.
Method: We performed a retrospective review of EUS-guided biopsies performed from 1/1/2019 - 31/8/2023 to investigate solid pancreatic lesions at a tertiary centre. Data was obtained from the endoscopy database and the electronic medical record. The final diagnosis was based upon surgical resection histopathology or if non-resected, clinical follow-up at least 6 months following the EUS-guided biopsy.
Results: 80 patients were included in this review. The correct diagnosis was obtained in 75 of 80 patients, equivalent to a diagnostic accuracy of 93.75% (95% CI, 86%-97.9%). Over the study period, there was increased utilization of the Acquire (Boston Scientific) biopsy needle, although this needle did not outperform the other needles. There was no association with diagnostic accuracy and location of the pancreatic mass. There were 3 minor complications reported from the 80 procedures.
Conclusion: EUS-guided tissue acquisition to investigate solid pancreatic lesions at our institution has high diagnostic accuracy and is a safe procedure.
77
Colonic full thickness resection device: Single-centre experience
Vicki McGarrigle, Leonardo Zorron Cheng Tao Pu, Rhys Vaughan, Marios Efthymiou and Sujievvan Chandran
Austin Health, Melbourne, Australia
Introduction: Endoscopic full-thickness resection (eFTR) using a Full Thickness Resection Device (FTRD) is an emerging technique for resecting difficult colorectal lesions and early colorectal cancers. This method potentially reduces the risk of polyp recurrence and may avoid invasive surgery. Data on its use and outcomes in Australia are limited.
Methods: Participants were selected from Austin Health’s FTRD database, including all patients who underwent colorectal FTRD. Data collected included patient demographics, lesion size, technical success, resection rates, and complications. Statistical analysis was performed using IBM SPSS.
Results: A total of 23 patients were included (mean age 65, 70% males). Technical success was 91%, with complete histological resection (R0) in 96%. Delayed complications occurred in 17% of cases, with 75% due to bleeding and 25% due to appendicitis. The mean procedure time was 44 minutes. Difficult positioning was associated with delayed complications (75% vs. 5.6%, p=0.021). Delayed bleeding occurred in 67% of diverticular associated lesions compared to 5% for other FTRD indications (p=0.02). Delayed bleeding was also more common in difficult positions (60% vs. 0%, p=0.006). No significant associations were found between variables and R0, although large effect sizes were noted between procedure time and delayed complications (-1.1)
Discussion: In this small study, FTRD appears to be effective for the resection of complex colorectal lesions. This study highlights important predictive factors for FTRD complications. Understanding these factors is crucial for improving outcomes and patient care. We plan to gain further insight with a multi-centre FTRD study across Australia and New Zealand.
105
Are improvements in biochemical and radiological markers following endoscopic drainage of walled off necrosis associated with reduced need for reintervention and survival?
Matthew Bartlett1, Jade Frank2, John Leeds3, Kofi Oppong3, Sanjay Pandanaboyana3 and Manu Nayar3
1Sir Charles Gairdner Hospital, Perth, Australia;2Prince Charles Hospital, Brisbane, Australia;3Freeman Hospital, Newcastle Upon Tyne, United Kingdom
Background and Aim: Endoscopic step-up approach for walled off necrosis (WON) following acute pancreatitis involves EUS guided insertion of lumen apposing metal stents (LAMS) and is now the standard of care. Treatment response varies, many patients will require further intervention via direct endoscopic necrosectomy to aid resolution of WON. Small studies have identified biochemical factors associated with need for repeat re-intervention including duration of elevated c-reactive protein (CRP). This study aimed to evaluate whether biochemical and radiological improvements following LAMS insertion are associated with fewer reinterventions and survival.
Methods: Patients were identified from an acute pancreatitis regional remote care pathway. Patients with WON who underwent endoscopic drainage between 2018 and 2023 were included. Retrospective data on baseline characteristics, pancreatitis characteristics, and number of endoscopic necrosectomies following LAMS insertion was collected. CRP and white cell count (WCC) around the LAMS insertion were investigated. Improvement was defined as >5% reduction within 48 hours following insertion. CT scan reports within 7 days of LAMS insertion were collected, improvement was defined as a report commenting on improvement in the collection with no other adverse changes. The outcomes assessed were need for necrosectomy following LAMS insertion, and death during admission. Differences in these outcomes was evaluated based on CRP, WCC and radiological responses.
Results: 97 patients were identified. 42 patients had reduction of CRP >5%, 41 patients had reduction of WCC >5% following LAMS insertion. Requirement for necrosectomy was not significantly different in those with and without CRP reduction, 35 (83%) vs 50 (91%) (OR 0.50, p=0.21); or in those with and without WCC reduction, 33 (80%) vs 52 (93%) (OR 0.32, p=0.07). Inpatient deaths were not significantly different in those with and without a CRP reduction, 2 (5%) vs 9 (16%) (OR 0.25, p=0.07); or in those with and without WCC reduction, 5 (12%) vs 6 (11%) (OR 1.17, p=0.82). Radiological improvement following LAMS insertion was present in 53 patients. Requirement for necrosectomy was not significantly different in those with and without radiological evidence of improvement, 45 (85%) vs 40 (91%%) (OR 0.56, p=0.37). Inpatient deaths were not significantly different between patients with or without radiological improvement 7 (13%) vs 4 (9%) (OR 1.5, p=0.52).
Conclusion: CRP, WCC and radiological improvements following insertion of LAMS are not associated with fewer reinterventions or reduced risk of death. Further investigation of factors associated with successful response to endoscopic drainage is needed.
208
Endoscopic ultrasound-fine needle aspiration in a regional secondary centre in Victoria: an evaluation of diagnostic yield for pancreatic malignancies in pancreatic masses and complication rates
Daniel Yee Lee Ng, Mitchell Steele, Tania Chapman, Sajith Kattiparambil Gangadharan and Dileep Mangira
Grampians Health, Ballarat, Australia
Background and Aim: Endoscopic ultrasound (EUS) with fine needle aspiration/biopsy (FNA) is an important diagnostic tool for pancreatic masses. Multiple aspects of the EUS-FNA process may influence the efficacy of results including needle gauge, number of needle passes and patient presentation. This study evaluated the efficacy and safety of EUS-FNA approach in investigating pancreatic masses at a secondary regional centre.
Methods: All cases of EUS with suspected pancreatic lesions performed by a single endoscopist at a secondary regional centre were identified between June 2022 and September 2023. Data collected included: indication, performance of FNA, needle gauge utilized, number of passes performed, histology results, complications, and presentations to hospital within 4-week period post-procedure. Pathology results that were positive for neoplastic findings were noted as “cytologic positive”, and if further confirmed via surgical means are considered “histologic positive”. For pathology results that were negative, subsequent radiological investigations were identified and assessed for progression. If no surveillance was performed or found 6-months after procedure, the case was excluded as loss of follow-up. If surveillance imaging showed progression, the instance was considered false-negative, and if no progression, this was considered confirmation of benign findings. A calculation of sensitivity, specificity, positive predictive value (PPV) and negative predictive value was performed; as well as a report of occurrences of complications.
Results: A total of 86 EUS procedures were identified, 5 were excluded as they were performed for therapeutic purposes. 24 were indicated for pancreatic masses. A total of 22 FNAs were performed in this subgroup. 19 FNAs were positive for neoplastic findings: 17 adenocarcinomas, 1 adenocarcinoma with concurrent chronic lymphocytic leukemia (CLL) in a patient with known CLL, and 1 perivascular epithelioid cell tumour (PEComa). 8 of these findings were confirmed surgically. The remaining 3 FNAs identified 2 intraductal papillary mucinous neoplasms (IPMN) with low-grade dysplasia, 1 of which had radiological progression and the other considered benign. 1 sample was identified as chronic pancreatitis but lost to follow-up. All cases utilized a 22-gauge fine needle biopsy device except in 2 instances where a 25 and 19-gauge needle was utilized due to lack of availability, and an additional 19-gauge needle was utilized. In both cases findings were positive for neoplasms. An average of 3 passes was performed. Cumulative sensitivity was 95%, specificity of 100%, PPV of 100%, and NPV of 50%. A breakdown of figures was provided in red (for “cytologic-only positive” cases) and green (for “histologic positive” cases). This is summarized in figure 1. 4 complications were recorded across the 81 EUS procedures as follows: 1 superficial mucosal tear; 1 exacerbation of chronic pancreatitis; 2 cases of abdominal pain (1 of which was post-ERCP). No complications resulted in mortality. Complication rate 4/81 (4.9%).
224
Endo-ACEF: Endoscopic ultrasound-guided gallbladder drainage in the elderly and frail: A prospective multicentre cohort trial
Sidhartha Gupta1, Andrew Gray1 and Daniel Croagh1,2
1Monash Health, Melbourne, Australia;2St Vincent's Hospital, Melbourne, Australia
Background and Aim: Acute cholecystitis (AC) is a prevalent condition requiring emergency surgery, particularly among the elderly and frail population. (1) Since 2007, endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) has emerged and evolved as a viable alternative to laparoscopic cholecystectomy for non-surgical candidates. (2) Australia's aging population is well documented, with nonagenarians growing faster than any other age group. Although laparoscopic cholecystectomy is the standard treatment for cholecystitis, it poses significant risks for patients with high comorbidity burdens or poor physical health, especially in emergency settings. Data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) shows a cholecystectomy-associated mortality rate of 5.5% in nonagenarians, rising to 9.5% in emergencies. (3) Additionally, older patients often experience a more severe disease course, with higher conversion rates to open surgery. (4, 5)
Traditionally, percutaneous cholecystostomy (PC) has been used to manage cholecystitis in high-risk surgical candidates. EUS-GBD offers a minimally invasive, definitive treatment, avoiding the drain-related morbidity associated with PC. Recent randomised trials have favoured EUS-GBD over PC for high risk surgical patients with AC given lower rates of adverse events, reinterventions and readmissions. (6) Little research has prospectively assessed EUS-GBD as the primary modality specifically in the elderly, who may or may not be high surgical risk, or frail patients of any age.
We aim to evaluate EUS-GBD utilising a lumen opposing metal stent (LAMS) to as the primary intervention for patients that are either aged eighty-eight years or older, or at least moderately frail. This will include patients who are elderly and frail, elderly and fit, as well as patients that are frail but not necessarily elderly. This age threshold strikes a balance between limiting the intervention between those of extreme age while maximising the potential population that could benefit.
Methods: This multicentre prospective cohort study evaluates the technical and clinical success of EUS-GBD in patients aged eighty-eight years and older, or those classified as at least moderately frail, across two tertiary academic institutions. The surgical team will assess frailty using the Clinical Frailty Score (CFS), with patients having a CFS ≥ 6 out of 9 total points considered for inclusion. Eligible patients will undergo EUS-GBD with a lumen-apposing metal stent (LAMS) after fitness assessment by the Anaesthetic and Peri-Operative Medical Unit. The primary endpoints are the technical success rate of EUS-GBD (confirmed by endoscopic and CT imaging) and clinical success rate (resolution of symptoms and biochemical improvement). Secondary endpoints include procedure-related morbidity and mortality, and long-term LAMS efficacy and patency. Retrospective data of previous EUS-GBD procedures is also being collected.
Discussion: We anticipate that our trial will demonstrate high clinical and technical success rates for EUS-GBD, with lower morbidity and mortality compared to traditional surgical approaches. We also expect a reduced rate of recurrent gallstone-related morbidity compared to non-operative treatments for AC. By focusing on elderly and frail patients, this study aims to highlight the benefits of endoscopic definitive treatment. Future research could explore lowering the age and frailty thresholds to expand the benefits of minimally invasive endoscopic treatment to a broader patient population.
References
1. Escartín, A, González, M, Cuello, E et al. Acute cholecystitis in Very Elderly Patients: Disease Management Outcomes, and Risk Factors for Complications. Surgery Research and Practice2019; 2019: 9709242.
2. Baron, TH, Topazian, MD. Endoscopic transduodenal drainage of the gallbladder: implications for endoluminal treatment of gallbladder disease. Gastrointest Endosc.2007 Apr; 65(4): 735-737.
3. Irojah, B, Bell, T, Grim, R, et al. Are They Too Old for Surgery? Safety of Cholecystectomy in Superelderly Patients (≥ Age 90). The Permanente Journal2017; 21: 16-013.
4. Borzellino, G, Sauerland, S, Minicozzi, A, et al. Laparoscopic cholecystectomy for severe acute cholecystitis. A meta-analysis of results. Surgical Endoscopy2008; 22: 8–15
5. Dubecz, A, Langer, M, Stadlhuber, R et al. Cholecystectomy in the Very Elderly – Is 90 the New 70?Journal of Gastrointestinal Surgery2012; 16: 282-285.
6. Teoh, AYB, Kitano, M, Itoi, T, et al. Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in very high-risk surgical patients with acute cholecystitis: an international randomised multicentre controlled superiority trial (DRAC 1)Gut2020; 69: 1085–1091.
226
Can optical evaluation distinguish between T1a and T1b esophageal adenocarcinoma: an international expert inter-observer agreement study
Sunil Gupta1,2, Francesco V Mandarino1, Julia Gauci1, Anthony Whitfield1,2, Clarence Kerrison1, Prabha Selvanathan3, Puja Kumar1, Neal Shahidi1, Luke Hourigan3, Helmut Messmann4, Michael Wallace5, Alessandro Repici6, Mario Dinis-Ribeiro7, Gregory Haber8, Andrew Taylor9, Irving Waxman10, Peter Siersema11, Roos Pouw12, Arnaud Lemmers13, Raf Bisschops14, Jeffrey Mosko15, Christopher Teshima15, Krish Ragunath16,17, Thomas Rosch18, Oliver Pech19, Torsten Beyna20, Prateek Sharma21, Eric Y Lee1, Stephen Williams1, Nicholas Burgess1,2 and Michael J Bourke1,2
1Westmead Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia;3Princess Alexandra Hospital, Brisbane, Australia;4University Hospital, Augsburg, Germany;5Mayo Clinic, Jacksonville, USA;6Humanitas Research Hospital, Milan, Italy;7Porto Comprehensive Cancer Center, Porto, Portugal;8NYU Langone Health, New York, USA;9St Vincent's Hospital Melbourne, Melbourne, Australia;10Rush University Medical Center, Chicago, USA;11Radboudumc Radboud Institute for Health Sciences, Nijmegen, Netherlands;12Amsterdam University Medical Centers, Amsterdam, Netherlands;13CUB Erasme Hospital, Belgium;14University Hospitals Leuven, Belgium;15St Michael's Hospital, Toronto, Canada;16Royal Perth Hospital, Perth, Australia;17Curtin Medical School, Perth, Australia;18University Hospital Hamburg-Eppendorf, Hamburg, Germany;19St. John of God Hospital, Regensburg, Germany;20Evangelisches Krankenhaus, Düsseldorf, Germany;21Kansas City VA Medical Center, Kansas City, USA
Introduction: While piecemeal EMR for T1a oesophageal adenocarcinoma is acceptable, R0 excision is advocated for T1b disease as it may offer a potential cure and mitigate recurrence. Thus, distinguishing between T1a and T1b disease is imperative under current treatment paradigms. We sought to ascertain whether expert Barrett’s endoscopists were able to make this distinction based on optical evaluation.
Methods: Sixty sets of endoscopic images of histologically confirmed high grade dysplasia (HGD), T1a and T1b disease (n=20 sets for each) were compiled from consecutive patients at a single institution. Each set contained four images, and were standardized to include an overview, a close-up in high-definition white light, a near-focus magnification image, and a narrow-band image. Experts were invited to predict histology for each set.
Results: 19 experts from 8 countries (Australia, USA, Italy, Netherlands, Germany, Canada, Belgium, and Portugal) participated. The majority had been practicing for >20 years, with a median annual case volume for Barrett’s EMR of 50 (IQR 18-75), and Barrett’s ESD of 25 (IQR 10-45). Oesophageal adenocarcinoma (T1a/b) could be distinguished from HGD, with a pooled sensitivity of 89.1% (95% CI: 86.7-91.2). When predicting the T-stage for T1b adenocarcinoma cases, the pooled sensitivity was 43.8% (95% CI: 38.5-49.2). Fleiss’ kappa was 0.421 (95% CI: 0.399-0.442, P<0.001), indicating fair-to-moderate agreement.
Conclusions: Expert Barrett’s endoscopists can reliably differentiate T1a/T1b oesophageal adenocarcinoma from HGD. Although there is fair-to-moderate agreement for T-staging, T1b disease cannot be reliably distinguished from T1a disease. This may have implications on clinical decision making and selection of endoscopic treatment methods.
242
Endocytoscopy in real time assessment of histological and endoscopic activity in ulcerative colitis
Thanaboon Chaemsupaphan1,2, Mohammad Shir Ali1, Sudarshan Paramsothy1,3 and Rupert Leong1,3
1Department of Gastroenterology and Liver Services, Concord Repatriation General Hospital, Sydney, Australia;2Division of Gastroenterology, Department of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand;3Faculty of Medicine and Health, University of Sydney, Sydney, Australia
Background and Aim: With 500-fold magnification, endocytoscopy (CF-H290ECI; Olympus Medical Systems Corporation, Japan; ARTG 121183) is a novel advanced imaging technology enabling real-time imaging of the intestinal mucosa. Endoscopic-histological remission assessment in ulcerative colitis (UC) has become the standard of care. Endoscopists, however, are uninvolved in the assessment of histology. Endocytoscopy might improve workflow and efficiency in the evaluation of UC activity.
Methods: In this single-center, prospective cohort study at Concord Hospital, Sydney, UC participants consenting to colonoscopy and endocytoscopy for disease assessment were recruited. Methylene blue chromoendoscopy enhanced cellular imaging. Data collected were demographics, disease activity, Mayo endoscopic score (MES) and endocytoscopic activity based on crypt shape, inter-crypt distance, cellular infiltration, and extent of vascularization. Correlation against the MES and the Nancy histological index (NHI) was conducted and validation against the ErLangen Endocytoscopy in CoLiTis (ELECT) score, and the endocytoscopy score (ECSS) was performed using Kappa (κ) statistics and Spearman correlation coefficient (r). P value <0.05 was deemed statistically significant. Duration and adverse events data were recorded.
Results: A total of 61 colonic bowel segments were evaluated (endoscopic improvement 69%, histological remission 64%; Table 1). Endocytoscopy correlated significantly with MES using both the ECSS (κ=0.57, P < 0.001; r=0.81, P<0.001) and the ELECT (κ=1.00, P<0.001; r=0.85, P<0.001) scoring systems. Endocytoscopy correlated with NHI using both the ECSS (κ=0.47, P<0.001; r=0.74, P<0.001) and the ELECT (κ=0.89, P< 0.001; r=0.78, P<0.001) systems. ELECT score demonstrated superior diagnostic performance in determining histological improvement (NHI 0-1) with sensitivity, specificity, and AUROC of 96%, 100%, and 0.98 (95%CI: 0.95-1.00), versus 70%, 100%, and 0.85 (95%CI: 0.78-0.92) with ECSS. Of the 42 segments in endoscopic remission, 3 (7.1%) demonstrated histological activity on endocytoscopy. No serious adverse events were reported, apart from temporary urinary discolouration from methylene blue excretion.
Conclusion: Instant simultaneous endoscopic and histological assessment of IBD is possible using endocytoscopy, which was safe, accurate and well-tolerated. The ELECT score reflects histology significantly better than the ECSS.
Table1 Characteristics of colonic lesions of UC cohort
322
Transient biliary stenting facilitates large common biliary duct stone fragmentation, aiding the subsequent retrieval: a case report
Denis Rubtsov, Reuben Malloy, David Huynh, Robert Franz and Aditya Agarwal
The Prince Charles Hospital, Brisbane, Australia
Introduction: Endoscopic retrieval of large common bile duct (CBD) stones (>2.5mm) may be challenging during the endoscopic retrograde cholangiopancreatography (ERCP). When the calculus cannot be removed, transient plastic stents are placed in the CBD to permit free bile drainage. There is a growing body of evidence suggesting that stent placement may facilitate stone fragmentation and migration. We present a case of a large stone fragmentation following plastic stents insertion.
Case report: A 57-year-old man presented with jaundice, pruritis and abdominal pain in January 2024. He was febrile but hemodynamically stable. Total bilirubin was elevated to 142 umol/L (ref: N <20) and conjugated bilirubin was 98 umol/L (ref: N <4). Magnetic resonance cholangio-pancreatography (MRCP) demonstrated no cholelithiasis and an oval 24mm calculus in ampulla, with CBD dilatation to 15mm. Patient was managed with intravenous antibiotics and underwent ERCP, confirming the large calculus presence in the CBD. A sphincterotomy was performed with a monofilament traction sphincterotome using electrocautery. Balloon sphincterotomy was attempted, followed by lithotripter, however this failed to extract the stone. Two 10-French 7cm plastic biliary stents with a single external flap and a single internal flap were placed 6cm into the common bile duct to maintain bile flow. This was followed by an insertion of an additional 7-French 7cm plastic stent with full external and internal pigtails. The patient recovered well, and biochemical parameters normalised. He then represented for laparoscopic cholecystectomy 5 weeks later. A post-operative cholangiogram demonstrated a presence of multiple filling defects in the CBD, instead of one round 25mm calculus seen previously, which appeared to have been fragmented. A follow-up ERCP 8 weeks later showed three calculi in the CBD, the largest of which was 8mm in diameter. These were successfully and atraumatically retrieved with the balloon retraction. There were no large stone observed, and,considering there were no cholelithiasis on the index MRCP, it could be concluded that either the stone has been fragmented or migrated earlier.
340
Successful use of dual over-the-scope clips for haemostasis in high-risk duodenal ulcer bleeding
James Chen1,2, Tim Mitchell1 and Niroshan Muwanwella1
1Royal Perth Hospital, Perth, Australia;2University of Western Australia, Perth, Australia
Introduction: Managing high-risk active duodenal ulcer bleeding is challenging. While various techniques exist, the use of dual Over-The-Scope (OTS) clips for ulcer haemostasis remains unreported. We present a case illustrating the application of this technique in a complex bleeding duodenal ulcer scenario.
Case Presentation: A 46-year-old male with recent non-steroidal anti-inflammatory drug use following hip trauma presented with fresh rectal bleeding and signs of hemodynamic instability. Computed tomography angiography revealed an arterial blush in the antrum/D1, prompting a gastroscopy revealing a large superficial ulcer with two distinct areas of active arterial bleeding (Forrest Ia) (Figure A – first ulcer bleeding source). The ulcer had a local adrenaline injection (2 mL, concentration 1:20000) for vasoconstriction and improved visualization. Using an OVESCO OTS clip system, two clips (12mm outer diameter, 6mm arm length) were deployed under direct visualization to individual bleeding vessels within the ulcer bed (Figure B – second ulcer bleeding point with first OVESCO OTS clip seen distally, Figure C – post OTS clip deployment). Careful attention ensured optimal clip placement and avoided luminal obstruction. Haemospray was administered post-clip placement for comprehensive ulcer base coverage. Successful haemostasis was achieved post-clip deployment, with no significant bleeding during observation. Management included 72 hours of proton pump inhibitor infusion, NSAID avoidance, and rebleeding monitoring without complications. A repeat gastroscopy was performed 8 weeks after index gastroscopy with healed ulcer with two clips still in situ and no evidence of duodenal stricture (Figure D).
345
A retrospective audit of ERCP practice in the regional hospital
Thant Zaw1,2, Joseph Bradbear1, Aditya Agarwal1, Peter Boyd1,2 and Montri Gururatsakul1,2
1Cairns Hospital, Cairns North, Australia;2James Cook University, Cairns, Australia
Introduction: Endoscopic retrograde cholangiopancreatography (ERCP) plays a vital role in therapeutic procedures for disorders of the biliary and pancreatic systems. However, ERCP also is a high-risk endoscopic procedure. The major complications generally are: adverse events from anesthetic/sedation, bleeding, cholangitis, perforation and post ERCP pancreatitis. This study was done to evaluate our regional ERCP procedures against national standards to ensure quality control and enhance practice methods.
Aims and Methods: The retrospective audit over a period from May 2018 to December 2020 was conducted to evaluate our local ERCP practices against the guidelines, aiming to ensure quality assurance and enhance practice improvement. With a total of 654 ERCPs analyzed, performed by four different proceduralists, the audit underscores the hospital's role in the regional hospital. The audit utilised a meticulous cross-referencing approach, integrating data from the Provation database with the iEMR database and AUSLAB software for pathology results. The primary outcome is procedure findings and the successful cannulation and ductal clearance rates. The secondary outcome is to measure the complication rates of ERCP.
Results: Among 645 ERCPs were performed, to highlight the most common findings were biliary stones (50.75%) of the total, followed by biliary stricture (15.81%), microlithiasis (11.98%), malignant biliary obstruction (3.53%). The audit reported an average successful cannulation rate of 91.4% and a ductal clearance rate of 88.74%. The audit also focused on the incidence of complications, with 11 cases of post ERCP bleeding (1.7%), 9 cases had post-ERCP pancreatitis (1.4%), and 2 cases had perforation (0.3%). The sub-analysis of post-ERCP pancreatitis showed that there were 2 cases of mild, 3 cases of moderate, and 4 cases of severe pancreatitis.
Conclusion: The audit's findings are a testament to the hospital's commitment to maintaining high standards in ERCP procedures, reflecting the low incidence of significant complications highlights the effectiveness of the procedural protocols and pre-emptive measures in place to mitigate risks associated with ERCP.
351
Long term follow-up of 35 appendiceal orifice neoplasms resected by endoscopic full thickness resection
Oliver Cronin1,2,3,4, Kayla Meys2, Sofia Yuen2, Abhinav Vij2, Tamas Gonda2, Adam Goodman2, Michael J Bourke3,4 and Gregory Haber2
1Northern Hospital, Melbourne, Australia;2NYU Langone, New York, USA;3University of Sydney, Sydney, Australia;4Westmead Hospital, Sydney, Australia
Background and Aims: Endoscopic full-thickness resection (EFTR) is an established, safe technique for the resection of appendiceal orifice (AO) neoplasms. Post-EFTR appendicitis is a recognised complication. There are no systematic reviews and a paucity of literature which has assessed medium and long-term outcomes especially with respect to delayed appendicitis, mucocele, or fistula formation. We aimed to evaluate long-term efficacy of EFTR for AO lesions.
Patients and Methods: Consecutive AO lesions referred for consideration of EFTR were prospectively studied. Multiple data points were recorded including technical success, EFTR histopathological data, complications, and follow-up surveillance data by colonoscopy. Surveillance CT was performed due to concern of potential mucocele from the obstructed remnant appendix.
Results: Over a 4 year period to July 2023, 37 AO lesions were referred to a tertiary centre for consideration of EFTR. EFTR was attempted in 35 (95%) lesions. Most lesions were small [median size 10mm, interquartile range (IQR) 10-15mm], Paris 0-IIa morphology (n=32, 91%) with serrated histopathology (n=17, 49%). R0 resection was achieved in the majority of cases (n=34, 97%). Complications included appendicitis (n=4, 11%) and delayed bleeding (n=2, 6%). At 6-month (IQR 4-6 months) surveillance colonoscopy, there was 1 (3%) case of recurrence. This was successfully treated endoscopically, confirmed on a second surveillance colonoscopy. There was one case of appendicitis of the remnant at 7 months. At surveillance CT abdomen/pelvis (median 15 months, IQR 7-37 months), 2/17 (12%) fistulas were identified. Both of these patients had presumed adhesions due to abdominal surgery prior to EFTR.
Conclusions: EFTR is a safe, effective and durable technique for the curative resection of AO lesions. Appendicitis is a relatively common complication but often managed conservatively. The long-term significance post-EFTR fistulas remains unclear. Caution should be exercised when considering EFTR in a patient with prior regional surgery.
352
Endoscopic full thickness resection is a viable alternative to endoscopic submucosal dissection (ESD) for high-risk colonic lesions
Oliver Cronin1,2,3,4, Kayla Meys2, Sean Hacking2, Mouyed Alawad2, Sofia Yuen2, Jonathan Cohen2, Tamas Gonda2, Michael J Bourke3,4 and Gregory Haber2
1Northern Hospital, Melbourne, Australia;2NYU Langone, New York, USA;3University of Sydney, Sydney, Australia;4Westmead Hospital, Sydney, Australia
Background and Aims: Endoscopic submucosal dissection (ESD) is the primary resection technique recommended for high-risk colonic lesions to ensure an R0 resection. Endoscopic full-thickness resection (EFTR) offers a viable alternative. There is little available data on technique, efficacy and cure. We aimed to evaluate outcomes of patients with lesions containing high-grade dysplasia (HGD) and invasive cancer, resected by EFTR.
Patients and Methods: Consecutive non-lifting lesions referred to a single tertiary centre with suspected localised advanced pathology for consideration of EFTR were prospectively studied. Multiple data points were recorded including technical success, EFTR histopathological data, complications, and follow-up surveillance data.
Results: Over a 4 year period to July 2023, 39 lesions were considered eligible for EFTR as an alternative to EMR or ESD, of which 33 (85%) underwent EFTR. 18/33 (55%) lesions contained cancer and 15/33 (45%) lesions contained HGD only. The median size of cancer was 7mm [Interquartile range (IQR) 4-10mm] contained within a median lesion size of 30mm (IQR 21-31mm). The median depth of invasion was 2550μm (IQR 1625-3075μm) and the deepest resected layer contained sub-serosal fat. Of the lesions containing cancer removed by FTR, 17/18 (94%) had an R0 resection. The case without an R0 resection had deep margin involvement, resected to the sub-serosa (depth 4000μm). At 6 month [Interquartile range (IQR) 5-7 months] surveillance colonoscopy, there was 1/23 (4%) case with recurrence, successfully re-resected with FTR, with cure confirmed on second surveillance colonoscopy. Of the patients with cancer who were referred for surgical resection post-FTR, no (0/7, 0%) cases had residual cancer within the surgical specimen.
Conclusions: EFTR offers a viable, safe and effective alternative to ESD for lesions with advanced pathology. Resection options need to be individualised and clearly outlined to the patient.
372
One parathyroidectomy and a cyst-gastrostomy later: an unusual case of hypercalcaemic pancreatitis as a first presentation of primary hyperparathyroidism
Eloise James, Tessa Greeve, Gregory Moore and Fiona Pavan
Monash Health, Melbourne, Australia
Introduction: Acute pancreatitis is a common presenting complaint in the Emergency Department, often with a clear aetiology. Here we present the case of acute necrotising pancreatitis, requiring emergency endoscopic drainage, as a first presentation of primary hyperparathyroidism (PHPT) in a young female patient.
Case report: A young woman presented to the Emergency Department with abdominal pain and a reduced level of consciousness. Initial investigations revealed a serum lipase level of 8184 U/L (reference range 0-60U/L) suggestive of pancreatitis. Specific screening for causes found only raised serum adjusted calcium (2.89 mmol/L, reference range 2.1-2.6mmol/L). There was no ultrasound evidence of cholelithiasis or choledocholithiasis. She had no history of alcohol use, and no significant medical history. This suggested hypercalcaemia related acute pancreatitis, and further investigations found raised serum PTH (7.7pmol/L, reference range 1.5-7.0pmol/L) and neck imaging showed a parathyroid mass. She became febrile, and abdominal MR imaging showed necrotising pancreatitis with haemorrhagic collections, initially conservatively managed with broad spectrum antibiotics. Further CT imaging showed increasing size of collections (figure 1) with gastric outlet obstruction, and due to worsening sepsis she underwent endoscopic ultrasound (EUS) guided cyst-gastrostomy on day 18 of admission, and her clinical status improved. Contemporaneous medical management of PHPT-hypercalcaemia failed to reduce calcium levels, increasing to a maximum of 3.4mmol/L (reference range 2.1-2.6mmol/L). Due to this, she underwent a parathyroidectomy on day 19 of admission, and serum calcium levels reduced to within normal range. The relationship between pancreatitis and PHPT-hypercalcemia is debatable, and case reports in the literature suggest notably higher levels of serum calcium than this case, with less severe pancreatitis. Increasing serum calcium level in this case was not associated with worsening clinical or biochemical markers of pancreatitis, following definitive endoscopic management of associated pancreatic collections. This suggests that serum calcium level is not directly related to clinical course of pancreatitis, beyond a possible trigger threshold level as suggested in literature. However, calcium sequestration can be a feature of early pancreatitis, which in a case of PHPT may hinder interpretation of calcium levels.
379
Introducing innovative low-code/no-code applications in endoscopy: An app for streamlining triage, enhancing safety, and building regional connectivity for endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound (EUS) at a high volume, tertiary referral hospital
Clarence Kerrison, Brian Lam, Anthony Whitfield, Julia Gauci, Anthony Sakiris, Francesco V Mandarino, Eric Y Lee, Stephen Williams, Nicholas Burgess and Michael J Bourke
Westmead Hospital, Sydney, Australia
Background and Aim: Low-code/no-code (LCNC) applications remain underutilised as a clinician-driven solution for daily hospital tasks. Existing paper-based systems used for triage and booking of endoscopy referrals are inefficient, prone to documentation errors, and contribute to paper wastage. Our objective was to create an online referral pathway and real-time tracking board for ERCP and EUS to replace the current paper-based system at a large tertiary referral hospital.
Methods: Using Microsoft’s Power Platform™, PowerApps™, and Power Automate™, gastroenterology clinicians developed an online referral system, bookings and management board, and automated notifications centre for inpatient and outpatient ERCP and EUS referrals. The system went live in May 2023. Results were monitored to April 2024, when referrers were surveyed on the application’s usability.
Results: 1,392 requests for ERCP and EUS were monitored using the online board, 762 (55%) originating from the new online referral pathway, 405 (29%) manually uploaded from existing paper requests and 225 (16%) re-bookings facilitated by a re-request feature in the application. Of the total requests, 1030 (74%) were tracked to completion, with 219 pending procedures and 103 awaiting future surveillance, while 32 were declined and 8 on hold. Of the online referrals, 170 triggered high suspicion of cancer notifications, with 90% prioritised to first procedure dates within 2 weeks. Online referrals additionally had 100% documentation of patient co-morbidities, anti-platelet/anti-coagulant history through mandatory user input, this compared to 44% of the original paper-based requests (Pearson X2 = 530.24, p < 0.001). The boards real-time interface provides a full patient journey overview. On average 187 automated email and push notifications per month informed referrers of confirmed booking dates and delayed or completed procedures. 21 of 165 referring doctors responded to a survey representing six referring hospitals, 100% found the online referral system very or somewhat easy to fill out, 95% found the automated messages helpful, and one third booked a follow-up appointment after receiving a completed notification. 100% of responders recommended continuing with the system.
Conclusion: The use of LCNC applications for triage and booking of ERCP and EUS procedures enhances clinical decision making and efficiency in high volume referral centres, whilst coordinating feedback to referrers and endoscopy staff. The LCNCs application ensured 100% compliance with pre-procedural safety checks. This application was created using existing and accessible Microsoft 365™ business licencing and can be securely integrated into other hospitals with ease.
386
Diagnostic yield of rapid onsite evaluation and cell block in endoscopic ultrasound-guided fine needle biopsy of gastrointestinal lesions
Mohammad Shir Ali, Donna Gillies, Juan Olivares, Dane Cook and Stephen Philcox
John Hunter Hospital, Newcastle, Australia
Background and Aim: Endoscopic ultrasound (EUS)-guided fine needle biopsy (FNB) often incorporates in-room cytology, commonly referred to as rapid onsite evaluation (ROSE), where cytology slides are prepared and assessed in real-time. In contrast, the cell block (CB) technique uses tissue fragments to create a paraffin block, enabling multiple sections to be cut for in-lab analysis and immunostaining. Despite the advantages of ROSE, the advent of advanced fine-needle biopsy and utilisation of macroscopic on-site evaluation (MOSE) raises questions about the necessity of ROSE. This study examines the effectiveness of ROSE and CB in EUS-guided biopsy at our institution.
Methods: We retrospectively reviewed medical records of patients aged 16 or older who underwent an EUS at our institution over the past five years. We included patients who received an EUS-guided FNB of any gastrointestinal lesion.
Results: 617 patients underwent EUS with 256 scheduled for an EUS FNB. Out of these, 226 underwent the biopsy. ROSE was performed in 204 cases. Biopsies targeted pancreatic lesions (163), luminal (23), hepatobiliary (11), and other including lymph nodes (28). Out of 204 patients who underwent EUS FNB with ROSE, 104 (51%) had malignant or neoplastic cytology on ROSE. However, this number increased to 127 (62.2%) upon in-lab evaluation. This increase was primarily due to 21 cases where cytology initially identified as atypical during ROSE was reclassified as malignant or neoplastic after laboratory analysis. Additionally, while 18 out of 204 samples (8.8%) were deemed inadequate during the ROSE evaluation, upon in-lab analysis the final tissue adequacy rate was 97.6% (Table 1). Additionally, 120 patients underwent EUS-guided biopsies of solid pancreatic lesions. Of these, cytology slides were diagnostic in 100 cases, resulting in a diagnostic yield of 83.3%. In contrast, CB had a lower diagnostic yield of 39%. Although fewer patients had EUS-guided biopsies of luminal lesions or lymph nodes, the diagnostic yield for cytology slides and CB were relatively consistent across these groups (Table 2).
Conclusion: Our study underscores the significance of ROSE in enhancing the diagnostic yield of EUS-guided FNB for solid pancreatic lesions, with cytology slides proving highly effective in obtaining definitive diagnoses. While CBs appeared to have a lower diagnostic yield, this may be influenced by cases where a conclusive diagnosis was already achieved through cytology slides, suggesting that the potential utility of CBs could be underrepresented. To comprehensively assess these findings, prospective randomised trials comparing outcomes with and without ROSE are recommended.
405
Impact of margins ablation on the efficacy of cold-forceps avulsion with snare-tip soft coagulation (CAST) for non-lifting large non-pedunculated colorectal polyps
Francesco V Mandarino1, Tim O'Sullivan1,2, Julia Gauci1, Renato Medas1, Clarence Kerrison1,2, Anthony Whitfield1,2, Brian Lam1, Varan Perananthan1, Sunil Gupta1,2, Stephen J Williams1, Oliver Cronin1,2, Eric Y Lee1, Nicholas Burgess1,2 and Michael J Bourke1,2
1Gastroenterology and Hepatology, Westmead Hospital;2University of Sydney, Sydney, Australia
Background and Aim: Endoscopic Mucosal Resection (EMR) with Margin Thermal Ablation by Snare-tip Soft Coagulation (MTA) is effective to treat Large (>20mm) Non-Pedunculated Colorectal Polyps (LNPCP) with recurrence in large studies at <2%. Non-lifting LNPCP (NL-LNPCP) account for approximately 10% of LNPCP and are well managed by EMR with adjunctive Cold-forceps Avulsion with adjuvant Snare-Tip soft coagulation (CAST) for non-lifting areas, however recurrence occurs in >10%. We sought to evaluate the effect of MTA on NL-LNPCPs treated by EMR and CAST.
Methods: Prospective observational data on consecutive patients with NL-LNPCPs treated by EMR and CAST at a single tertiary center was evaluated. Two cohorts were established: the pre-MTA period (January 2012-June 2017) and the MTA period, (July 2017-October 2023). The primary outcome was the comparison of recurrence rates between the two groups at first surveillance colonoscopy at 6 months (SC1).
Results: From January 2012 to October 2023, 298 NL-LNPCPs in 298 patients (median age 69.1 years, interquartile range [IQR] 61.5-76.7 years, 43.4% male) underwent EMR and CAST (median size 36.0mm, IQR 24.7-54.2mm): 72 lesions pre-MTA and 226 with MTA. The MTA cohort had a higher rate of NL-LNPCP in complex locations (ileocecal valve, ano-rectal junction, appendiceal orifice) (18.6% vs 5.6%, p=0.02), granular lesions (61.9% vs 41.7%, p=0.01), and lesions with submucosal fibrosis (87.2% vs 72.2%, p=0.05). No differences were observed in procedural time. At SC1, recurrence was lower in the MTA cohort compared to the pre-MTA cohort (2.7% vs 9.7%, p<.001). Deep mural injury type III-V (4.4% vs 4.2%, p=.93) and post-procedural bleeding (5.3 vs 4.2%, p=.94) was similar between the MTA and pre-MTA cohort respectively. There was one case of delayed perforation in the pre-MTA group.
Conclusion: The implementation of MTA significantly reduced recurrence at SC1 for NL-LNPCP treated by EMR with CAST. The refinement of CAST and addition of MTA in recent years has enabled the treatment of more complex lesions with greater effectiveness without compromising safety.
Table 1
408
Outcomes of endoscopic submucosal dissection for the treatment of oesophageal squamous dysplasia and early squamous cell carcinoma in the West
Sunil Gupta1,2, Francesco V Mandarino1, Julia Gauci1, Anthony Whitfield1,2, Timothy O'Sullivan1,2, Oliver Cronin1,2, Clarence Kerrison1,2, Andrew Tang1, Eric Y Lee1, Stephen J Williams1, Nicholas Burgess1,2 and Michael J Bourke1,2
1Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;2University of Sydney, Sydney, Australia
Background and Aim: Endoscopic submucosal dissection (ESD) has evolved to become a viable treatment option for oesophageal squamous dysplasia (SD) and early squamous cell carcinoma (ESCC). Although enbloc, R0, excision has the potential to yield an endoscopic cure, surgery remains the standard of care in the West. Furthermore, Western data pertaining to endoscopic outcomes is limited. We aimed to assess the efficacy and safety of ESD for SD and ESCC in a single tertiary referral centre.
Methods: We conducted a prospective observational cohort study over 87 months until November 2023 in consecutive patients undergoing ESD for SD or ESCC. The primary outcomes were enbloc, R0 and curative resection rates. Secondary outcomes included procedure duration, tumor recurrence and adverse events.
Results: 112 consecutive patients were referred for treatment and underwent ESD (median age 73 [IQR 68-78]; 50% male; Table 1). Median lesion size was 30 mm (IQR 20-50mm) and Paris IIa was the most common morphology (58.9%). Enbloc resection was achieved in 109 (97.3%) and R0 excision in 87 (77.7%). Curative resection in cases of LGD and HGD, where margins were clear of dysplasia, was 7/11 (63.6%) and 31/34 (91.2%) respectively. In those with T1a/T1b SCC, the curative resection rate was 20/61 (32.8%). In T1a SCC lesions, 11/20 (55.0%) had a curative ESD. Of the remainder, 6/9 were poorly differentiated, 1/9 had LVI, and 2/9 had positive margins (1 deep, 1 peripheral). In T1b SCC lesions, 9/41 were curative (22.0%). The remainder were either poorly differentiated, >T1b-SM1, LVI positive or a combination. In those with T1a/T1b disease, without adverse tumor biology, ESD achieved curative resection in 20/22 (90.9%). In the 41/61 (67.2%) T1a/T1b patients that did not meet criteria for cure, subsequent treatment included surgery (n=5), radiotherapy (n=5) and chemoradiotherapy (n=1). After MDT discussion, the remaining 30 were managed conservatively, due to advanced age or comorbidities. In these, recurrence occurred in 6/30 patients (1 local, 3 nodal, 2 metastatic) at a median follow up of 12 months (6-18 months). The median hospital length of stay was 1 day (IQR 1-3). Oesophageal strictures occurred in 46 patients (41.1%), requiring a median of 3 dilations (IQR 1-8). There were 2 cases of delayed bleeding. There were no perforations.
Conclusion: ESD is curative for low and high-grade dysplasia. In a Western setting, ESD offers definitive T-staging and has the potential to yield a cure in almost 33% of T1a and T1b SCC cases. Due to a high risk of disease recurrence, adjuvant therapy should be considered in cases of a non-curative resection.
Table 1
416
Five-year clinical outcomes after per oral endoscopy myotomy (POEM) for achalasia
Varan Perananthan1,2, Lucy Bracken1, Andrea Huang3,4, Francesco V Mandarino1, Brian Lam1, Julia Gauci1, Clarence Kerrison1, Sunil Gupta1,2, Nicholas Burgess1,2, Spiro Raftopoulos5, Bronte Holt6, Luke Hourigan3,4 and Michael J Bourke1,2
1Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;2Westmead Clinical School, University of Sydney, Sydney, Australia;3Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Brisbane, Australia;4Gallipoli Medical Research Institute, School of Medicine, The University of Queensland, Brisbane, Australia;5Department of Gastroenterology and Hepatology, Sir Charles Gairdner Hospital, Perth, Australia;6Department of Gastroenterology, St Vincent's Hospital, Melbourne, Australia
Background and Aim: Per oral endoscopic myotomy (POEM) is a well-established treatment for achalasia with clinical success exceeding 90%. However, the durability of this response is unknown. We sought to evaluate the long-term outcomes of POEM for achalasia 5 years and beyond in a multi-centre setting.
Methods: Patients who underwent POEM for achalasia types 1, 2, and 3 were prospectively enrolled in a multi-centre observational study with data collected on technical aspects and short-term outcomes. Eckardt scores were calculated before treatment and at 6 months and 2 years after POEM. Among this cohort, patients who underwent POEM before June 2019 were contacted to assess long-term outcomes. The primary outcome was to evaluate the long-term clinical success at 5 years or beyond defined by an Eckart score ≤ 3 without the need for re-intervention. Secondary outcomes included identifying factors associated with re-intervention and subsequent management strategies.
Results: A total of 237 patients underwent POEM for achalasia in four Australian tertiary centres between January 2014 to June 2019. Median follow up was 6.0 years, (IQR 5.2 – 7.1 years). 47.6% of patients had Type 1, 35.9% had Type 2 and 16.5% had Type 3 achalasia. Previous treatments prior to POEM included Hellers myotomy; 12.6%, pneumatic balloon dilatation; 50.4% and botulinum toxin injection; 8.7%. The median Eckardt score prior to POEM was 8.0 (IQR 6.0 – 9.0) and at 6 months post-POEM was 0.0 (IQR 0.0 – 1.0, p<0.001). At 2 and 5 years follow up scores were 1.0 (IQR 0.00 – 2.00, p<0.001) and 0.0 (IQR 0.0 – 2.0, p<0.001) respectively. Five-year freedom from intervention was 87.6%. 6.2% required a re-do POEM at a median of 14 months post-POEM (IQR13.0 – 24.0) and 8.9% required a pneumatic dilatation at a median of 18 months post-POEM IQR (9.0 – 24.0). Type III achalasia was a risk factor for re-intervention, relative risk (RR) 1.41 (95% CI 1.17 – 1.60, p=0.04). Previous Heller’s was not a risk factor for re-intervention, RR 1.07 (95%CI 0.27 – 3.58), however pneumatic dilatation prior to initial POEM increased the risk of re-intervention, RR 1.71 (95% CI 1.12 – 2.33, p=0.02). Intra-procedural complications (such as major bleeding) were not risk factors for re-intervention, RR 0.97 95% CI (0.16 – 5.35).
444
Prevalence of endoscopically curable low-risk cancer amongst large non-pedunculated colorectal polyps
Julia Gauci1, Anthony Whitfield1,2, Renato Medas3,4, Clarence Kerrison1,2, Francesco V Mandarino1, David Gibson5, Timothy O'Sullivan1,2, Oliver Cronin1,2, Sunil Gupta1,2, Brian Lam1, Varan Perananthan1, Luke Hourigan6, Simon Zanati5, Rajvinder Singh7, Spiro Raftopoulos8, Alan Moss5, Gregor Brown5, Amir Klein9, Lobke Desomer10, David Tate11,12, Steven Williams1, Eric Y Lee1,2, Nicholas Burgess1,2 and Michael J Bourke1,2
1Westmead Hospital;2University of Sydney Medical School, Sydney;3Department of Gastroenterology and Hepatology, The Alfred Hospital, Department of Gastroenterology and Hepatology, Epworth Hospital, Melbourne;4Department of Gastroenterology, Princess Alexandra Hospital (Queensland Health), Brisbane;5Department of Gastroenterology and Hepatology, Lyell McEwin Hospital, Adelaide, South Australia, Australia;6Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia;7Centro Hospitalar e Universitario Sao Joao, Porto, Portugal;8Faculty of Medicine of University of Porto, Portugal;9Ambam Heath Care Campus, Rappaport Faculty of Medicine, Technion Institute of Technology, Haifa, Israel;10AZ Delta Roeselare, Ghent, Belgium;11Department of Gastroenterology and Hepatology, University Hospital of Ghent, Ghent, Belgium;12Faculty of Medicine, University of Ghent, Ghent, Belgium
Background and Aims: Endoscopic submucosal dissection (ESD) is increasingly promoted for the treatment of all large non-pedunculated colorectal polyps (LNPCP), to cure potential low-risk cancers (superficial submucosal invasion without additional high-risk histopathological features). The effect of a universal en bloc strategy on oncological outcomes for the treatment of LNPCP in the right colon is unknown. We evaluated this in a large Western population.
Methods: A prospective cohort of patients referred for endoscopic resection (ER) of LNPCP was analysed. Patients found to have cancer after ER and those referred directly to surgery were included. The primary outcome was to determine the proportion of right colon LNPCP with low-risk cancer.
Results: Over 180 months until June 2023, 3294 sporadic right colon LNPCP in 2956 patients were referred for ER at 7 sites (median size 30mm [IQR 15]). 63 (2.1%) patients were referred directly to surgery and cancer was proven in 56 (88.9%). 2851/2956 (96.4%) LNPCP underwent ER (median size 35mm [IQR 20]) of which 75 (2.6%) were cancers. The overall prevalence of cancer in the right colon was 4.4% (131/2956). Detailed histopathological analysis was possible in 115/131 (88%) cancers (71 after ER, 44 direct to surgery). After excluding missing histopathological data, 23/2940 (0.78%) sporadic right colon LNPCP were low-risk cancers.
Conclusions: The proportion of right colon LNPCP referred for ER containing low-risk cancer amenable to endoscopic cure was <1%, in a large, multicentre Western cohort. A universal ESD strategy for the management of right colon LNPCP is unlikely to yield improved patient outcomes given the minimal impact on oncological outcomes.
Endoscopic resection related duodenal strictures: Prevalence, risk factors, management and outcomes
Julia Gauci1, Renato Medas2,3, Francesco V Mandarino1, Clarence Kerrison1,4, Anthony Whitfield1,4, Sunil Gupta1,4, Hunter Wang4, Mayenaaz Sidhu1,4, Brian Lam1, Lucy Bracken1, Varan Perananthan1, Timothy O'Sullivan1,4, Oliver Cronin1,4, Steven Williams1,4, Eric Y Lee1,4, Nicholas Burgess1,4 and Michael J. Bourke1,4
1Westmead Hospital, Sydney, Australia;2The University of Sydney, Westmead Clinical School of Medicine, Sydney, Australia;3Centro Hospitalar e Universitario Sao Joao, Porto, Portugal;4Faculty of Medicine of University of Porto, Porto, Portugal
Background and Aim: Endoscopic resection (ER) of large (≥15mm) duodenal laterally spreading lesions (D-LSLs) is now standard of care. Data on prevalence, risk factors and management of strictures after ER of D-LSL are absent; we sought to evaluate this is in a large tertiary referral cohort.
Patients and Methods: A prospective cohort of D-LSLs treated by ER in an expert tissue resection centre was analysed. Strictures were considered "severe" if patients experienced obstructive symptoms, "moderate" if an adult gastroscope (diameter 9.9mm) could not pass the stenosis, or "mild" if there was resistance on successful passage. When necessary, dilatation was performed every 2-4 weeks, until scope passage without resistance was achieved. Primary outcomes included stricture prevalence, risk factors and management.
Results: Over 193 months until February 2023, 246 lesions in 239 patients were included (51.2% male, median age 70 years [IQR 14], median size 35mm [IQR 25]). 30 (12.2%) resections resulted in stenosis; 14 mild (46.7%), 4 moderate (13.3%) and 12 severe (40%). 18 (7.3%) required balloon dilation (median number of sessions, 2 [IQR 6]). After multivariable analysis, post ER-defect circumference ≥80% was the strongest independent predictor for stricture formation (OR 62.96 [confidence interval 17.9-276.7], p<0.001). The incidence of stricture formation with an ER-defect ≥80%, 60-79% and <60% was 72.2% (n=26/36), 12.5% (n=4/32) and 0% (n=0/178) respectively. All severe strictures (12/12, 100%) occurred in ER-defects ≥80%.
Conclusions: ER-defect circumference strongly predicts stricture formation following ER of D-LSL. These findings can be used to guide informed consent and post-procedural care.
447
Safety and efficacy of endoscopic retrograde cholangiopancreatography in nonagenarians - A retrospective cohort study
Amirah Etchegaray1, Sanjivan Mudaliar1, Kimberley Ryan1, Karen Hay2, Jason Hwang1, Benedict Devereaux1, Mark Appleyard1 and Florian Grimpen1
1Royal Brisbane and Women's Hospital, Brisbane, Australia;2QIMR Berghofer Medical Research Institute, Brisbane, Australia
Background and Aim: Increasing numbers of older patients with pancreatobiliary disease are undergoing Endoscopic Retrograde Cholangiopancreatography (ERCP). Older patients may be at higher risk of post-ERCP complications due to age and comorbidities, however, data to support this claim is lacking. The aim of this study was to evaluate long-term mortality, procedural outcomes, and safety of ERCP in nonagenarian patients aged 90 years and older.
Methods: A retrospective study of consecutive patients aged ≥90 years that underwent ERCP at a single adult tertiary hospital between March 2011 and April 2023. Subjects were identified from a prospectively maintained endoscopy database (Provation MD). Endoscopic records were reviewed for procedural factors, including successful biliary cannulation, sphincterotomy, and stent placement. The primary outcome was long-term survival. Secondary outcomes included procedural success and adverse events. Post-ERCP adverse events were classified according to the American Society for Gastrointestinal Endoscopy (ASGE) guidelines. Logistic regression was used to analyse procedural outcomes, survival explored using Kaplan-Meier methods and factors predictive of survival identified using Cox proportional hazard modelling.
Results: 159 consecutive ERCP were performed in 115 nonagenarian patients. The mean age of the cohort was 92.3 (SD ± 2.1); 67% of patients were referred from a rural or regional hospital with a steady increase in ERCPs performed throughout the study period (Figure 1A). Choledocholithiasis with cholangitis (78.6%) was the most common indication, followed by malignant biliary obstruction (MBO, 18.9%), and bile leak (2.5%). Majority [88%] of nonagenarians with benign pathology were symptomatic (cholangitis and/or raised pre-procedure bilirubin >20μmol/L) at first ERCP, including 9% with a non-native papilla. Survival was significantly reduced with malignancy, with a 30-day, 3-month and 1 year survival of 78%, 52% and 9% respectively, compared to 98%, 94% and 89% for choledocholithiasis (p=<0.001, Figure 1B). Technical success was achieved in 91% of index ERCPs including 95% of procedures for benign pathology and 67% for MBO (p=<0.001). Complications occurred in 5% of procedures, most commonly cardiorespiratory (1.8%), bleeding (1.2%) and pancreatitis (0.6%). The 30-day mortality in patients that experienced a complication was 13.4% (n=1, choledocholithiasis with cholangitis).
Conclusion: Our data suggests that therapeutic ERCP is a safe, effective and clinically relevant intervention for benign and malignant pathology in select nonagenarians. Age does not constitute a barrier to the performance of ERCP in appropriately selected patients. Nonagenarians may be counselled for a success and complication rate equivocal to younger populations.
449
Impact of margin thermal ablation on recurrence after endoscopic mucosal resection of large (≥40mm) colorectal lesions
Julia Gauci1, Clarence Kerrison1,2, Anthony Whitfield1,2, Timothy O'Sullivan1,2, Sunil Gupta1, Francesco V Mandarino1, Brian Lam1, Varan Perananthan1, Oliver Cronin1, Renato Medas1, Eric Y Lee1, Nicholas Burgess1,2 and Michael J Bourke1,2
1Westmead Hospital;2Westmead Clinical School of Medicine, The University of Sydney, Sydney, Australia
Background and Aim: Endoscopic mucosal resection (EMR) of large (≥20mm) non-pedunculated colorectal polyps (LNPCP) ≥40mm is complex, and associated with an increased risk of recurrent or residual adenoma (RRA). Margin Thermal Ablation to the EMR defect margin using snare-tip soft coagulation (MTA) reduces the rate of RRA. Its impact on this high-risk LNPCP subgroup is unknown. We sought to analyse its effect in a large prospective cohort of LNPCP ≥40mm.
Methods: We retrospectively analysed a prospectively collected cohort of consecutive patients who underwent conventional EMR in an expert tissue resection centre. MTA technique was developed in 2012. Enrolment for the MTA randomised control trial took place between July 2013-May 2016 and became standard practice from mid-2017. The cohort was divided into three phases: ‘pre-MTA’; July 2008- June 2012, ‘MTA adoption’; July 2012-June 2017 and ‘standardised MTA’; July 2017-July 2023. RRA was defined as adenomatous tissue detected at the first surveillance colonoscopy (SC1) and confirmed on histology. MTA was defined as complete application of snare-tip soft coagulation to the entire EMR defect margin. The primary outcome was to compare the RRA rate between the three time periods.
Results: Over 15 years until July 2023, 1023 LNPCP ≥40mm in 1023 patients underwent EMR (median lesion size 50mm, IQR 20mm) of which 936 (91.5%) were successful. 836 patients (median lesion size 50mm, IQR 20) underwent SC1 at a median of 6 months (IQR 4). The rates of RRA in the pre-MTA, MTA-adoption and standardised-MTA phases were 20.3% (n=45/221), 19.2% (n=59/308) and 4.9% (n=15/307) respectively (p=<0.001). The rates of complete MTA in the pre-MTA, MTA adoption and standardised-MTA phases were 0, 37.7% (n=116/308) and 94.5% (n=290/307). 17 (5.5%) of cases within the standardised-MTA did not receive MTA due to difficult access (n=7), concern for stricture formation in fully circumferential LNPCP (n=8) or sedation-related issues (n=2). The rate of RRA in this group was 22.2% (n=4/18).
Conclusion: Margin thermal ablation post-EMR of LNPCP ≥40mm (median size 50mm) significantly reduced the rate of RRA in a large, prospective cohort. When MTA was not applied, RRA was similar across the three time periods (p=0.1), indicating that the main impact on RRA reduction was the use of MTA with snare-tip soft coagulation, rather than a factor of EMR technique improvement over time.
455
Endoscopic ultrasound-guided gallbladder drainage compared to percutaneous cholecystostomy drainage: observational cohort study to assess safety and outcomes in non-operative candidates
Michael Chieng1, Rees Cameron2, Estella Johns2, Jerry Chin1 and Frank Weilert1
1Health New Zealand, Hamilton, New Zealand;2Health New Zealand, Wellington, New Zealand
Background and Aim: Cholecystectomy is the definitive treatment for cholecystitis but many patients are not surgical candidates or require bridging treatments before surgical candidacy. Percutaneous cholecystostomy (PC) is the current standard-of-care for achieving gallbladder decompression in non-surgical cholecystitis (NSC) but has risks of incomplete drainage, tube displacement, and disease recurrence. Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) is an emerging intervention that allows for insertion of wider drainage internal stents. We compared the outcomes of EUS-GBD with PC to determine safety, feasibility, and risks of re-intervention for both approaches in NSC.
Methods: Outcomes of 19 EUS-GBD cases were retrospectively compared with a randomized sample of 27 PC cases performed between January 2010 and January 2023 at two tertiary referral centres in New Zealand. Demographic and outcome data were recorded including technical success, clinical success, length of hospital stay (LOS), adverse events, and re-interventions. Clinical success was defined by clinical improvement (resolution of fever, improvement in biochemistry, and symptoms) within 72 hours of the procedure. Median follow up of the cohorts was 24 months.
Results: Age, gender and ethnicity data were balanced between groups. Technical and clinical success were complete in both EUS-GBD (n=19/19) and PC (n=27/27) cohorts, with no intra-procedural complications. EUS-GBD cases allowed for insertion of a wider diameter drainage device (10mm vs 3mm, p=<0.0001). There were significantly fewer adverse events in the EUS-GBD group (15.8% vs 51.9%, p=0.03) and proportionally fewer re-interventions, although this did not reach statistical significance (3/19 [15.8%] EUS-GBD vs 9/27 [33.3%] PC, p=0.21). EUS-GBD achieved significantly earlier discharge than the PC group (LOS: 4 days vs 12 days, p=0.006). EUS-GBD adverse events included cholangitis (1) and recurrent cholecystitis (2). PC adverse events included cholangitis (3), GB haemorrhage (1), PC displacement (2), PC blockage (2), recurrent cholecystitis (4), peritonitis (1), and pain requiring hospitalisation (1). There was no requirement for emergent surgery in the EUS-GBD cohort, however, three surgeries performed in the PC group related to complications of PC tube dysfunction.
Conclusion: Compared with traditional PC for the treatment of cholecystitis in non-surgical candidates, EUS-GBD was technically comparable and safe with significantly fewer adverse events, reduced hospital stay, and lower need for emergent surgery.
463
Endoscopic ultrasound-guided gallbladder drainage for malignant biliary obstruction in patients who have failed ERCP and EUS-guided choledochoduodenostomy: safety and outcomes
Michael Chieng1, Rees Cameron2, Estella Johns2, Jerry Chin1 and Frank Weilert1
1Health New Zealand, Hamilton, New Zealand;2Health New Zealand, Wellington, New Zealand
Background and Aim: Endoscopic ultrasound-guided gallbladder drainage (EUS-GBD) is described as a rescue therapy for patients with malignant biliary obstruction who fail biliary access with ERCP and/or EUS-guided choledochoduodenostomy (EUS-CDD). The traditional approach in this setting has been percutaneous transhepatic cholangiogram (PTC) but this carries risks. There have been few small series reporting outcomes of EUS-GBD for this indication. We report a multi-centre review of outcomes for malignant biliary drainage utilising EUS-GBD in non-surgical patients.
Methods: A review of a prospectively collected cohort of 28 EUS-GBD cases was performed between January 2017 and January 2024 at two tertiary referral centres in New Zealand. A transduodenal approach was universal, using electrocautery-enhanced lumen apposing metal stents (LAMS), and anaesthesia-assisted sedation. Demographic and outcome data were recorded including technical success, clinical success, length of hospital stay (LOS), adverse events, re-interventions, and survival. Clinical success was defined by clinical improvement (resolution of fever, improvement in biochemistry, and symptoms) within 72 hours of the procedure. Re-interventions were split into early procedures, deemed necessary within 7 days, or late procedures occurring beyond 7 days. Median follow up was 36 months.
Results: Mean age of the cohort was 74 years (SD=9) with 9/28 (32.1%) females, and 5/28 (17.9%) Māori ethnicity. Pancreatic cancer was the most common diagnosis in 78.6% (22/28). Technical and clinical success was achieved in all 28 cases (100%). Stent size ranged from 8 – 15mm, with a median of 10mm. There were no procedural complications and no early re-interventions. Mean length of hospital stay was 4 days (SD=4). Adverse events were recorded in 14/28 (50%) with the majority (9/14, 64.3%) being infectious and managed conservatively with antibiotics; except for one patient who underwent PTC. There was one mortality 4 days following EUS-GBD, which was attributable to peritonitis from stent maldeployment of previously attempted EUS-CDD. EUS-GBD was performed as a rescue therapy in this setting and occurred without complication. 17.9% (5/28) cases required re-intervention over the follow up period. Recurrent biliary obstruction occurred in 3 cases (10.7%), with 1 case of cholangitis (3.57%), and stent obstruction (3.57%). These were treated with PTC (n=3), ERCP (n=1) and stent removal (n=1) respectively. Median survival was 135 days.
Conclusion: EUS-GBD is technically and clinically successful at treating malignant biliary obstruction offering a short hospital stay and excellent procedural adverse event profile. Late adverse events occurred as shown in previous series, but more than 82% of cases did not require any invasive reintervention. In a cohort of non-surgical candidates with advanced malignancy, planning a definitive treatment that avoids further intervention is paramount and EUS-GBD decompression appears to offer a safe, effective, and durable alternative to PTC in this setting.
468
Risk of bleeding after X-Tack closure of large mucosal defects in high risk patients: A case series
Peter Litwin1, Kelly Tam2, Kathryn Sharley1, Amanda H Lim1,3, Jeevinesh Naidu3 and William Tam1,3
1Royal Adelaide Hospital, Adelaide, Australia;2Bond University, Robina, Australia;3University of Adelaide, Adelaide, Australia
Background and Aim: There is evolving literature on the risk of bleeding in large mucosal defects after polypectomy in patients on anticoagulant and antiplatelet medications. We report our experience of using X-tack, a through-the-scope suture-based device to close large, irregularly shaped mucosal defects after polypectomy of upper and lower gastrointestinal lesions in an elderly cohort with high rates of antithrombotic use.
Methods: Data were collected from prospective cases performed by 2 endoscopists at three institutions. The X-Tack device was used to close large irregular mucosal defects and in circumstances where the endoscopist considered post-procedural bleeding risk to be high. Where relevant, antiplatelet medication was continued, whilst anticoagulation was held for 48 hours pre-procedure (or where renal function mandated otherwise) and re-commenced on the day of procedure.
Results: Fourteen patients (median age: 74 years, IQR: 19) underwent the X-tack procedure. Defects were closed in the stomach (n=1), duodenum (n=1), proximal colon (n=9) and distal colon (n=3). Diathermy snare was utilised in mucosal resection in all but one case (duodenal adenoma). Median size of the lesions was 33mm (IQR: 31), with histology demonstrating 10 tubular or tubulo-villous adenomas, 2 sessile serrated lesions, 1 neuroendocrine tumour and 1 invasive adenocarcinoma. Nine of the fourteen patients were on anti-coagulant (n=4) or anti-platelet (n=5) therapy. Technical success of device deployment was 93%, with one device malfunctioning requiring closure using clips. Ten of the fourteen patients achieved defect closure using a single X-Tack device alone. Two patients required a second X-Tack kit and four (including patient with failed X-Tack deployment) required additional clips to close the respective mucosal defects. Clinical success was 86% over a median 10 month follow up period, with no incidents of perforation but two patients (one on anticoagulant, one on antiplatelet) did experience mild, delayed post-procedural bleeding at day 4 and day 8 respectively. Both patients were managed conservatively without the need for repeat endoscopy, blood transfusion, interventional radiology or surgery.
473
Safety and efficacy of Kaffes intraductal self-expanding metal stents in the management of post-liver transplant anastomotic strictures
Chee Lim1, Jonathan Ng1, Babak Sarraf1, Rhys Vaughan1,2, Marios Efthymiou1,2, Leonardo Zorron Cheng Tao Pu1,2 and Sujievvan Chandran1,2
1Austin Health, Australia;2Melbourne Medical School, The University of Melbourne, Melbourne, Australia
Background and Aim: Endoscopic management is the first-line therapy for post-liver-transplant anastomotic strictures. Although the optimal duration of treatment with plastic stents has been reported to be 8-12 months, data on safety and duration for metal stents in this setting is scarce. Due to limited access to endoscopic retrograde cholangiopancreatography (ERCP) during the coronavirus disease 2019 pandemic in our centre, there was a change in practice towards increased usage and length-of-stay of the Kaffes biliary intraductal self-expanding stent in patients with suitable anatomy. This was mainly due to the theoretical benefit of Kaffes stents allowing for longer indwelling periods compared to the traditional plastic stents. We aimed to compare the safety and efficacy profile of different stenting durations using Kaffes stents.
Methods: Adult liver transplant recipients aged 18 years and above who underwent ERCP were retrospectively identified during a 10-year period through a database query. Unplanned admissions post-Kaffes stent insertion were identified manually through electronic and scanned medical records. The main outcome was the incidence of complications when stents were left indwelling for 3 months vs 6 months. Stent efficacy was calculated via rates of stricture recurrence between patients that had stenting courses for ≤ 120 d or > 120 d.
Results: During the study period, a total of 66 ERCPs with Kaffes insertion were performed in 54 patients throughout their stenting course. In 33 ERCPs, the stent was removed or exchanged on a 3-month interval. No pancreatitis, perforations or deaths occurred. Minor post-ERCP complications were similar between the 3-month (abdominal pain and intraductal migration) and 6-month (abdominal pain, septic shower and embedded stent) groups - 6.1% vs 9.1% respectively, P = 0.40. All strictures resolved at the end of the stenting course, but the stenting course was variable from 3 to 22 months. The recurrence rate for stenting courses lasting for up to 120 d was 71.4% and 21.4% for stenting courses of 121 d or over (P = 0.03). There were 28 patients that were treated with a single ERCP with Kaffes, 21 with removal after 120 d and 7 within 120 d. There was a significant improvement in stricture recurrence when the Kaffes was removed after 120 d when a single ERCP was used for the entire stenting course (71.0% vs 10.0%, P = 0.01).
Conclusion: Utilising a single Kaffes intraductal fully-covered metal stent for at least 4 months is safe and efficacious for the management of post-transplant anastomotic strictures.
490
The west catching up with the east: high-magnification NBI is an accurate tool for the diagnosis of gastric neoplasia in a western population
Edward Young1,2, Nicholas Wan1,2, Andrew Ruszkiewicz1,3 and Rajvinder Singh1,2
1Lyell McEwin Hospital, Northern Adelaide Local Health Network;2Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, Australia;3SA Pathology, Adelaide, Australia
Introduction: Gastric cancer is the third leading cause of cancer-related death worldwide.1 In high-incidence countries such as Korea and Japan, nationwide gastric cancer screening programs have reduced the incidence of advanced gastric cancer by facilitating detection of lesions at an early stage amenable to endoscopic resection.2 Accurate endoscopic prediction of histology and invasion depth is critical for guiding endoscopic or surgical resection techniques. In these high-incidence countries, high-magnification narrow band imaging (M-NBI) has been established as an effective form of advanced mucosal imaging for diagnosis and prediction of invasion depth.3, 4 Data is lacking on the applicability of this technique in western populations where early gastric cancer is less frequently encountered.
Methods: This is an analysis of a prospectively collected database of gastric lesions that were assessed and either biopsied or resected by an interventional endoscopist at a single Australian Public Hospital between 2009 and 2023. All lesions were assessed endoscopically using M-NBI and a determination made at the time of reporting whether the lesion was neoplastic or non-neoplastic, as well as histological prediction between adenoma, early gastric cancer, invasive adenocarcinoma and ‘other neoplastic’ lesions. This was then correlated with the final histology. 95% confidence intervals of classification statistics were obtained based on binomial proportions and a kappa statistic was calculated to assess the agreement between M-NBI histological prediction.
Results: A total of 232 lesions in 183 patients were included in the final analysis, including 35 adenomas, 29 early gastric cancers, 6 invasive adenocarcinomas, 137 non-neoplastic lesions and 25 ‘other neoplastic’ lesions (including neuroendocrine tumours and lymphoma). For differentiating neoplastic versus non-neoplastic lesions, M-NBI had a sensitivity of 97.9% (CI 92.6-99.7%) and specificity of 97.1% (CI 92.7-99.2%), with a PPV of 98.52% (CI 94.8-99.8%) and NPV of 95.9% (CI 89.8-98.9%). The overall accuracy of M-NBI was 97.4% (CI 94.5-99.1%). M-NBI also had high specificity (97.1%, CI 92.7-99.2%) for identifying lesions suitable for endoscopic resection, with a PPV of 96.9% (CI 89.2-99.6%). The observed agreement between the M-NBI predicted histology and the final pathological diagnosis was 91.81% with a derived kappa statistic of 0.865, indicating excellent agreement.
Conclusion: M-NBI can be used with a high degree of accuracy in western populations, equivalent to the accuracy demonstrated by experts in eastern countries. When used by a proceduralist trained in advanced mucosal imaging M-NBI is highly specific for identifying appropriate lesions for endoscopic resection.
References
1. Bray, F, Ferlay, J, Soerjomataram, I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin2018; 68: 394-424.
2. Narii, N, Sobue, T, Zha, L, et al. Effectiveness of endoscopic screening for gastric cancer: The Japan Public Health Center-based Prospective Study. Cancer Sci2022; 113: 3922-3931.
3. Kato, M, Kaise, M, Yonezawa, J, et al. Magnifying endoscopy with narrow-band imaging achieves superior accuracy in the differential diagnosis of superficial gastric lesions identified with white-light endoscopy: a prospective study. Gastrointest Endosc2010; 72: 523-9.
4. Kobara, H, Mori, H, Fujihara, S, et al. Prediction of invasion depth for submucosal differentiated gastric cancer by magnifying endoscopy with narrow-band imaging. Oncol Rep2012; 28: 841-7.
500
Intraductal papillary mucinous neoplasm of bile duct: A case report of the challenges of diagnosis and management
Michael Christmas1, Wilson Siu1, Perveen Aslam1, Shivendra Lalloo1, Mitali Fadia1, Ngee-Soon Lau1 and Vipul Aggarwal1,2
1ACT Health, Canberra, Australia;2Australian National University, Canberra, Australia
Introduction: Intraductal papillary mucinous neoplasm of the bile duct (IPMN-B) is a rare tumour arising from biliary epithelial tissue and recognized as a precursor lesion to cholangiocarcinoma. IPMN-B are characterized by intraluminal hypersecretion of mucin that can intermittently impede bile flow, leading to repeated episodes of cholangitis and biliary obstruction1. Diagnosis can be challenging particularly due to the lack of defining features on imaging2. Surgical resection remains the definitive treatment3. Here we present a case of the endoscopic challenges prior to surgical resection.
Case presentation: A 78 year old male originally from Laos, with a background of non-insulin dependent diabetes, chronic obstructive pulmonary disease and transient ischaemic attack. Presented to our institution with cholangitis, serum bilirubin 190 umol/L and CRP 55mg/L. This is in the setting of recent admission one month earlier with painless jaundice (serum bilirubin 50 umol/L) where he was treated as cholangitis and his initial investigation had not revealed a cause for biliary obstruction. With improving bilirubin (39 umol/L) and clinical improvement, he was discharged with plan for ongoing outpatient investigations. On admission he was commenced on antibiotics and similar to his initial, Magnetic Resonance Cholangiopancreatography (MRCP) revealed dilated and tortuous intrahepatic biliary ducts in both lobes of the liver. No choledocholithiasis nor mass lesion was seen. An initial Endoscopic Retrograde Cholangiopancreatography (ERCP) removed a significant amount of pus from the CBD, but no stones or sludge, a 10 French 7 cm straight plastic stent was placed. Subsequent CT imaging did not show decompression of the intrahepatic ducts, there was no significant decline in the serum bilirubin (206 umol/L). This prompted repeat ERCP for placement of longer stents into the Left Intrahepatic Duct (LIHD) and Right Intrahepatic Duct (RIHD) raising possibility of RIHD stricture. We opted to insert 10 Fr 10cm and 10 Fr 12cm straight plastic stents, respectively. Despite these measures, the biliary obstruction persisted (bilirubin 291 umol/L). The team then opted for a RIHD percutaneous transhepatic cholangiostomy (PTC) for drainage of the biliary system. There was initially reasonable output from the PTC and decline in serum bilirubin (256 umol/L) that plateaued with time, a repeat CT scan showed the PTC drain to be in an appropriate position. The decision was then made to proceed with a combined gastroenterology and interventional radiology case. Endoscopic technique: Through the existing right Percutaneous Transhepatic Biliary Drainage (PTBD), a long 0.035 inch wire was introduced into the periampullary duodenum for endoscopic capture. The original PTC drain was removed and replaced by 10 French Cook sheath. ERCP was performed with removal of the 2 previous plastic stents and capture of the wire. With balloon sweep, copious drainage of viscous mucopurulent material was expelled through the ampulla. Interval cholangiogram revealed partial clearing of filling defect in the CHD/CBD with improved contrast passage. Subsequent over the wire passage of Spyglass choledochoscope system confirmed accumulation of mucoid material at the hilar confluence and CHD, and a flat, villous lesion was revealed at the confluence of the right liver sectoral ducts, the anterior more affected. Several biopsy samples obtained with spybite microforceps with biopsies confirming IPMN-B with low-grade dysplasia. Finally, a 15 cm 10 Fr plastic stent was deployed over the PTC placed guidewire, the rostral end shown to be favourably positioned in the anterior sectoral duct on final cholangiogram obtained through upsized 12 French internal/external drain. The latter also demonstrated considerable clearance of prior mucoid filling defects in the CHD/CBD. Post procedure, the patient’s bilirubin remained stubbornly elevated (200 umol/L). A flushing technique of the PTC was employed where a flush of 10mL normal saline was delivered every 8 hours and increasing to every 6 hours finally resulting in declining bilirubin (84 umol/L at discharge). The patient’s family was taught how to continue this until the patient’s planned surgery. The patient did not require any further admissions to hospital prior to having his extended right hemihepatectomy.
Conclusions: Technical challenges exist with the diagnosis and early management of IPMN B. Techniques in diagnosis and therapy to alleviate the burden of mucinous obstruction prior to surgical resection are described here.
References
1. Yeh, TS, et al. Cholangiographic spectrum of intraductal papillary mucinous neoplasm of the bile ducts. Ann Surg.2006 Aug; 244(2): 248-53.
2. Kung, JWC, et al. Intraductal papillary neoplasm of the bile duct: the role of single-operator cholangioscopy. VideoGIE.2017 Dec 13; 3(2): 55-57.
3. Ohtsuka, M, et al. Intraductal papillary neoplasms of the bile duct. Int J Hepatol.2014; 2014: 4590-91.
505
Cold vs hot snare endoscopic mucosal resection for large (≥15mm) flat non-pedunculated colorectal polyps: A randomized controlled trial
Timothy O'Sullivan1,2, Oliver Cronin1,2, Arnout Van Hattem3, Francesco V Mandarino1, Julia Gauci1, Clarence Kerrison1, Anthony Whitfield1,2, Sunil Gupta1,2, Eric Y Lee1, Stephen Williams1, Nicholas Burgess1,2 and Michael J Bourke1,2
1Department of Gastroenterology and Hepatology, Westmead Hospital, Sydney, Australia;2Westmead Clinical School, University of Sydney, Sydney, Australia;3Department of Gastroenterology and Hepatology, Netherlands Cancer Institute, Amsterdam, Netherlands
Background and Aim: Endoscopic mucosal resection (EMR) is standard of care for the management of large (≥20mm) non-pedunculated colonic polyps (LNPCPs). Its efficacy and cost effectiveness were limited by recurrence. Margin thermal ablation (MTA) to the post-EMR defect, has greatly mitigated this problem. However, electrocautery-related complications of delayed bleeding and perforation incur significant morbidity. Cold snare polypectomy is effective and safe for the resection of small polyps with negligible recurrence rates. Application of cold snare resection to LNPCPs, while an attractive alternative, lacks high-quality evidence. We conducted a randomized trial to compare the efficacy and safety of cold EMR (C-EMR) to conventional (H-EMR).
Methods: A prospective single-centre randomized controlled trial was conducted at an Australian tertiary referral centre for flat, 15-50mm adenomatous LNPCPs referred for endoscopic resection. Prior to resection, eligible LNPCPs were randomly assigned to EMR using a dedicated cold snare or conventional H-EMR with margin thermal ablation (control). First surveillance colonoscopy (SC1) was conducted 6 months following resection. Scars were evaluated with high-definition white-light, narrow-band imaging and biopsy. The primary outcome was endoscopically visible and/or histologically confirmed recurrence at SC1. Secondary outcomes were clinically significant post-EMR bleeding (CSPEB), delayed perforation and technical success.
Results: 920 LNPCPs were referred for endoscopic resection between November 2019-September 2023. 177 LNPCPs in 177 patients were randomized to either the C-EMR arm (n=87) or H-EMR arm (n=90). Treatment groups were equivalent with no significant difference in lesion size or technical success (86/87 (98.9%) vs 90/90 (100%); p=0.31). One C-EMR required conversion to H-EMR due to unexpected submucosal fibrosis. Following exclusions, 147 LNPCPs undertook SC1 (77 C-EMR, 70 H-EMR). On intention to treat and per protocol analysis, recurrence was significantly greater in C-EMR (16/87, 18.4% vs 1/90, 1.1%; RR 16.6, 95%CI 2.24-122; p<0.001 and 16/76 (21.1%) vs 1/70 (1.4%); p<0.001 respectively). Significant deep mural injury (27/90 (30%) vs 0; p<0.001) and delayed perforation (1/90 (1.1%) vs 0; p=0.32) only occurred in the H-EMR group. CSPEB and intraprocedural bleeding were significantly greater in the H-EMR arm (7/90 (7.8%) vs 1/87 (1.1%); RR 6.77, 95% CI 0.85-53.9; p = 0.034 and 12/90 (13.3%) vs 1/87 (1.1%); p=0.002 respectively).
Conclusion: Compared to conventional H-EMR, C-EMR for flat, adenomatous LNPCPs, demonstrates superior safety with equivalent technical success. However, endoscopic recurrence is significantly greater for cold snare resection and is currently a limitation of the technique.
508
Multicentre prospective evaluation of the Hot Spaxus lumen apposing metal stent for EUS-guided drainage of pancreatic walled off necrosis
Tony He1, Nicholas Burgess2, Milan S Bassan3, Benedict Devereaux4 and Bronte Holt1
1St Vincent's Hospital Melbourne, Melbourne;2Westmead Hospital;3Liverpool Hospital, Sydney;4Royal Brisbane and Women's Hospital, Brisbane, Australia
Background and Aims: Endoscopic ultrasound (EUS)-guided drainage of pancreatic walled off necrosis (WON) with cautery-assisted lumen-apposing metal stents (LAMS) has a high technical and clinical success rate of 53-100%1,2. This study aims to prospectively evaluate a new cautery-assisted LAMS (Hot Spaxus, Taewoong Medical, Korea) to inform on the safety and efficacy of the device in the treatment of WON.
Methods: This is a prospective, multicenter cohort study conducted at four tertiary care hospitals in Australia, including patients with symptomatic pancreatic WON requiring EUS-guided drainage. Procedures were performed with anaesthetic support and intravenous antibiotics, under EUS and fluoroscopy control. Decision for and timing of direct endoscopic necrosectomy was based on degree of necrosis. LAMS were removed at 4 weeks, with clinical and radiologic follow up at 1 and 3 months. Primary outcomes were technical success, intra-procedural and 30-day major adverse events. Secondary outcomes included clinical success, stent-related complications, procedural time and number of reinterventions.
Results: 20 patients (mean (SD) age 54.6 (15.6); females 55%; mean (SD) WON size 12.8cm (4.6); 10% had >50% solid necrosis, 55% had 21-50% necrosis, 35% had <20% necrosis) were enrolled and included in the final analysis. Primary indication for EUS-guided drainage was abdominal pain (80%). Technical success was 100% with no intra-procedural complications. One patient (5%) had a splenic artery pseudoaneurysm bleed 29 days post-LAMS insertion, treated by radiologically guided embolization. The median (IQR) time for stent deployment was 10 minutes (5, 10). The mean (SD) number of endoscopic interventions to clear the cavity was 2.95 (1.7). The LAMS was removed at a mean (SD) time of 29.3 days (6.5), replaced by double pigtail stents in 95% of patients for long term drainage. 10% of patients had a likely disconnected duct on EUS or CT/MRI. At 3-months, 95% of patients had resolution of pre-intervention symptoms and 90% had WON resolution on CT/MRI.
Conclusion: The new cautery-assisted LAMS has a high technical and clinical success rate for the treatment of pancreatic WON, with no intra-procedural complications, and a similar post-procedural adverse event profile to alternative devices. Randomized prospective studies comparing the available cautery-assisted LAMs in the treatment of pancreatic WON are required.
References
1. Chandrasekhara, V, Barthet, M, Devière, J, et al. Safety and efficacy of lumen-apposing metal stents versus plastic stents to treat walled-off pancreatic necrosis: systematic review and meta-analysis. Endosc Int Open.2020; 8: E1639–E1653.
2. Baron, TH, DiMaio, CJ, Wang, AY, Morgan, KA. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology. 2020; 158(1): 67-75.e1.
509
Impact of margin thermal ablation after endoscopic mucosal resection of large (≥20mm) non-pedunculated colonic polyps on long term recurrence
Timothy O'Sullivan1,2, Francesco V Mandarino1, Julia Gauci1, Anthony Whitfield1,2, Clarence Kerrison1
Catarina Neto do Nascimento, Sunil Gupta1,2, Oliver Cronin1,2, Anthony Sakiris1, Juan F Prieto Aparicio1, Sophie Arndtz3, Gregor Brown3, Spiro Raftopoulos4, David Tate5,6, Eric Y Lee1, Stephen Williams1, NICHOLAS BURGESS1,2, MICHAEL J BOURKE1,2
1Department of Gastroenterology and Hepatology, Westmead Hospital, Australia;2Westmead Clinical School, University of Sydney, Sydney, Australia;3Department of Gastroenterology and Hepatology, The Alfred Hospital, Melbourne, Australia;4Department of Gastroenterology, Sir Charles Gairdner Hospital, Perth, Australia;5Department of Gastroenterology and Hepatology, University Hospital of Ghent, Ghent, Belgium;6University of Ghent, Ghent, Belgium
Background and Aim: EMR is the standard of care for the management of large (≥20mm) non-pedunculated colonic polyps (LNPCPs). However, its efficacy and cost effectiveness, are limited by recurrence and the necessity for scheduled surveillance. Consequently, current surveillance intervals are conservative. Margin thermal ablation (MTA) after EMR for LNPCPs has dramatically reduced the incidence of recurrence at first surveillance colonoscopy at six-months (SC1). If this effect is durable, then subsequent surveillance intervals in patients who have been cleared of synchronous polyps could be substantially lengthened. We prospectively evaluated long-term surveillance outcomes in a cohort of LNPCPs that have undergone MTA.
Methods: Consecutive patients with LNPCPs undergoing EMR and MTA from four academic endoscopy centres were prospectively recruited. All patients that underwent successful endoscopic resection received SC1 six months post resection. EMR scars were carefully evaluated with high-definition white light, narrow band imaging with near focus and biopsy. In the absence of recurrence, second surveillance (SC2) colonoscopy was conducted at a subsequent interval of 12 months with the scar evaluation process repeated. A historical control arm was generated from LNPCPs that underwent EMR without MTA. The primary outcome was recurrence at SC2 in all LNPCPs with a recurrence-free scar at SC1.
Results: 1315 LNPCPs referred for EMR were enrolled over 90 months until October 2022. Following exclusions, 1148 LNPCPs underwent EMR with complete MTA. 238 LNPCPs formed the control arm from January 2012-May 2016. 852 LNPCPs underwent SC1. 31 additional synchronous LNPCPs were cleared at this procedure. 26/852 (3.1%) LNPCPs demonstrated recurrence. 472 LNPCPs free of recurrence at SC1 underwent SC2 at a mean interval of 23.1 months (95%CI 22.1-24.2) after the index EMR. 471 demonstrated a bland scar without recurrence. Only one recurrence occurred related to a 0-IIa+Is 20mm granular TVA located on the ileocaecal valve. Recurrence at SC2 was significantly less in the MTA arm vs controls (1/472 (0.2%) vs 9/238 (3.8%); p <0.001).
Conclusion: LNPCPs that have undergone successful EMR with MTA and are free of recurrence at SC1 are very unlikely to develop recurrence in subsequent surveillance out to 2 years. Following EMR of LNPCPs with MTA, patients who are cleared of synchronous neoplasia and demonstrate no recurrence after careful scar examination, can potentially undergo next surveillance in 3-5 years. Such an approach would reduce costs and enhance patient compliance.
515
Efficacy and safety of EUS-guided drainage of post-surgical fluid collections
Michael MacIsaac1, Tony He1, Tulio Soares1, Fiona Jones1, Lena Tabbaa2, Daniel Croagh2 and Bronte Holt1
1St Vincent's Hospital Melbourne, Australia;2Monash Health, Melbourne, Australia
Introduction: Post-surgical fluid collections (PSFCs) are a common complication of gastrointestinal (GI) surgery and are usually managed by percutaneous drainage. Emerging data suggests that endoscopic ultrasound (EUS) guided drainage of PSFCs may be a safe and effective alternative, which can similarly be performed early after PSFC development (≤4 weeks).
Methods: Retrospective, multi-centre cohort study of all patients referred for EUS-guided drainage of symptomatic PSFCs after hepatobiliary, upper GI or colorectal surgery at two tertiary referral centres in Melbourne, Australia over a 7-year period from 1st January 2016 to 31st December 2022. Patients were identified using hospital databases, multi-disciplinary meeting records and review of all EUS cases, with electronic medical record data extraction. Primary outcome measures were technical success (ability to access and drain a PSFC by placement of a transmural stent), clinical success (complete clinical resolution of symptoms and reduction/resolution of PSCF on CT at 3 months) and rate of adverse events, with major adverse events defined as grade III or above on the Clavien Dindo Classification.
Results: 42 patients were referred for EUS-guided drainage of PSFCs (median age 61 years (IQR, 46–71); 25 (60%) male). The most common index surgery was pancreatic (N=19, 45%) and the primary indication for drainage was sepsis (N=29, 69%). Mean collection size was 6.1cm (range 1.7–13.5cm). EUS was performed at a median of 30 days (IQR, 19-69 days) post-surgery; 19 (45%) were done in ≤4 weeks of PSFC development. EUS-guided drainage was attempted in 34 (81%) patients with 100% technical success. Eight patients were excluded at EUS due to unsuitable collection morphology (PSFC too small or not identified, N=5; immature PSFC wall, N=2; PSFC not abutting the GI lumen, N=1). Clinical success was achieved in 33/34 (97%) patients who underwent EUS-guided drainage; one patient had symptom resolution post drainage however follow up CT showed an increase in the size of the PSFC. A single EUS-guided drainage was performed in 29 patients; 5 patients required >1 endoscopic procedure (range 2–4). There were no intra-procedural complications. Nine (26%) post-procedural adverse events occurred, of which three were classified as major adverse events.
Conclusions: EUS-guided drainage of PSFCs is technically feasible, can be safely performed early following PSFC formation in a significant proportion of patients and achieves high rates of clinical success with few major adverse events. It is a minimally invasive alternative to percutaneous drainage, avoiding the need for an external drain with attendant risk of blockage, dislodgement, and infection. EUS-guided drainage should be considered as a therapeutic option for patients with PSFCs after GI surgery.
534
Endoscopic ultrasound related adverse events at a tertiary hospital
Deepu David1,2, Michael Ma2, Vanoo Jayasekeran2 and Andre Chong2
1Sunshine Coast University Hospital Sunshine coast, Australia; 2Fiona Stanley hospital, Perth, Australia
Background and Aim: Endoscopic ultrasound (EUS) is a commonly used procedure in Gastroenterology. Although EUS complication rate is presumed to be low, scarce data exists from Australia. Aim of this study was to assess the complication rates and the factors influencing the complications in patients undergoing EUS.
Methods: A retrospective review of all adult patients who underwent EUS examination between Dec 2014 and June 2022 June were conducted. Patients needing inpatient admission within 5 days of undergoing the procedure were included in the study. Data including the demographics, details of the procedure and the adverse events were collected.
Results: A total of 1868 patients had undergone EUS during the period. 135 patients needed admission within 5 days post-procedure after undergoing EUS-guided FNA. 21 patient admissions were for complications related to the EUS procedure. The most common complication was acute pancreatitis, and all cases were mild in severity (33.33%). One patient with pancreatitis had undergone a concomitant ERCP, along with EUS. Other complications noted were duodenal ulcer-associated hematemesis, duodenal perforation, retroperitoneal hematoma, splenic vein thrombosis, mucinous cyst fluid leak into the peritoneal cavity, and cholangitis. A trainee was present in less than one-third of the procedures (31.5%) with complications. None of the patients with complications were on regular anticoagulants peri-procedure. There was no mortality associated with any of the complications.
Conclusion: The incidence of complications was extremely low. The most common complication was acute pancreatitis.
Table 1
550
Show me your PEC: Endoscopic ultrasound, histological features and management of an exceedingly rare pancreatic perivascular epithelioid cell tumour (PEComa)
Angus Ferguson1,2, Daniel Saitta1, Sharon Wallace1,3 and Dileep Mangira1,3
1Grampians Health Ballarat, Ballarat, Australia;2Western Health, Australia;3Dorevitch Pathology, Melbourne, Australia
Background: Perivascular Epithelioid Cell tumours (PEComas) are rare mesenchymal tumours, including angiomyolipomas, clear cell ‘sugar’ tumours, and lymphangioleiomyomas. These tumours are usually benign but may occasionally be malignant (1). Pancreatic PEComas are extremely rare, with only 35 cases reported in the literature as of 2024 (2). They are 4.5 times more common in women and typically present with vague or no symptoms (1). Noteworthy features of this case include utilisation of endoscopic ultrasound (EUS) in diagnosis of a PEComa.
Case: A 45-year-old woman, with a history of hemithyroidectomy, uterine fibroids, and depression, was admitted following a motor vehicle accident. An abdominal CT scan revealed a 14mm incidental arterial hyperenhancing focus at the head of the pancreas, initially suspected to be a neuroendocrine tumour. Follow-up MRI confirmed a T2 hyperenhancing 14x12.2x13.5mm hypervascular lesion. Serum investigations including FBE, UEC’s, LFTs and TFT’s, and tumour markers Chromogranin A, Ca 19-9, 5-HIAA were also within normal limits. EUS described a 16x14mm well-circumscribed mass at the head of the pancreas and subsequent fine needle aspiration biopsies showed epithelioid cells with glycogen-rich cytoplasm. Immunohistochemistry was positive for SMA, Caldesmon, HMB-45, Melan-A, and PR. The Ki-67 index was approximately 10%. Due to anatomical location, rarity of tumour and uncertain future malignant potential, this patient underwent a curative pancreaticoduodenectomy without adjuvant chemo/radiotherapy. She is now 6 months post procedure without evidence of recurrence.
Discussion: The immunohistochemical profile and morphological features confirmed the diagnosis of PEComa. Whilst PEComas are commonly benign some have malignant potential. The main clinical challenge lies in differentiating PEComas malignant potential to determine further management. Typically, classification utilises Folpe et al.’s criteria which assesses the presence of 6 features: Size >5cm; Infiltrative lesion; High nuclear grade and cellularity; Mitotic rate ≥1/50 HPF; Presence of necrosis; Presence of vascular invasion (3). The presence of 2 or more of these ‘worrisome’ features indicates a ‘Malignant' lesion; one feature indicates ‘Uncertain Malignant Potential’ and no features suggests a ‘Benign’ lesion. Given the rarity of pancreatic PEComas treatment guidelines are not well-established. However, surgical excision remains the standard approach, as seen in this case.
Conclusion: This case highlights an extremely rare differential of a pancreatic mass lesions. Early sampling and immunohistochemical analysis are crucial for accurate diagnosis and determining malignancy potential. This case emphasizes the role of endoscopic ultrasound in diagnosing this rare condition. Given their rarity, patient centred multidisciplinary management is essential. Surgical excision with pancreaticoduodenectomy is an extremely invasive procedure, so prior accurate diagnosis is a critical step before subjecting patients to such an invasive surgical approach. An ability to recognise and potential monitor for malignant radiological, EUS, and/or fine needle aspirate features may represent a viable alternative to surgery given their predominantly benign nature.
2. Sixto, MN, Iglesias, RC, Fernández, SE, Pereira, CR, Santos, RS. Pancreatic PEComa, a not so uncommon neoplasm? Systematic review and therapeutic update. Gastroenterol Hepatol2024; 47: 93-100.
3. Folpe, AL, Mentzel, T, Lehr, HA, Fisher, C, Balzer, BL, Weiss, SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol2005; 29: 1558–1575.
583
Outcomes of endoscopic resection of gastro-oesophageal junction high grade dysplastic and adenocarcinoma lesions
David Law, Marcus Chin and Niroshan Muwanwella
Royal Perth Hospital, Perth, Australia
Background and Aim: The incidence of oesophageal adenocarcinoma has been increasing in recent years with Barrett’s oesophagus being the main identified precursor. The gastro-oesophageal junction (GOJ) has a high rate of oesophageal adenocarcinoma. Defining the GOJ can be difficult with guidelines such as the Kyoto consensus proposed to help identification. Similarly, guidance on the surveillance of GOJ pre-cancerous lesions lacks clarity in existing Barrett’s oesophagus screening protocols. We reviewed the outcomes and histology of endoscopic resected GOJ lesions to identify whether pre-cancerous changes were present, which could help guide endoscopic screening of the GOJ.
Methods: Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) of GOJ lesions performed from May 2013 to December 2023 were captured through the local endoscopy reporting programme ProcRep. Details including patients’ characteristics, histology reports and follow-up procedures were obtained via electronic records. Patients with histology showing high grade dysplasia (HGD) or adenocarcinoma were included in the study, whilst non-dysplastic lesions were excluded.
Results: A total of 27 patients received endoscopic resection for GOJ lesions with HGD or adenocarcinomas, 13 underwent EMR and 14 underwent ESD. 15 of the 27 patients had T1a lesions, none of whom developed recurrence. 6 patients had T1b lesions, 5 proceeded with oesophagectomy or chemoradiotherapy. The remaining 1 patient declined further treatment, with no local recurrence on surveillance endoscopies. 13 patients were known with Barrett’s oesopahgus prior endoscopic resection, all of whom had short segment Barrett’s oesophagus. Of the remaining 14 patients, 7 had resection histology showing Barrett’s dysplastic changes, whilst 7 had no features of Barrett’s oesophagus.
Conclusion: Patients in our study achieved high clinical success from endoscopic resection with no case of recurrence. The majority of patients in our cohort had preceding Barrett’s oesophagus. However, 25.9% were noted with Barrett’s on histology only and another 25.9% had no Barrett’s oesophagus on endoscopy or histology. This highlights the importance of a thorough examination of the GOJ even in the absence of overt Barrett’s oesophagus. Further studies should be carried out to review the histology of GOJ adenocarcinomas without Barrett’s mucosal changes, to provide improved guidance on the screening of the GOJ and identifying pre-cancerous lesions.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
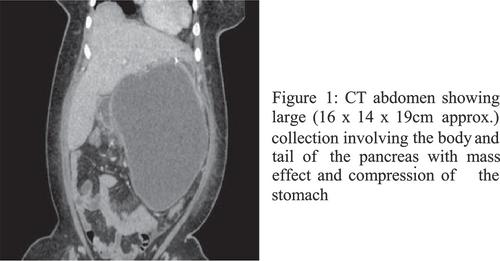
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


