{"title":"IBD Basic Science","authors":"","doi":"10.1111/jgh.16701","DOIUrl":null,"url":null,"abstract":"<p><b>93</b></p><p><b>The biogeography of the mucosa-associated microbiota is associated with the presence and symptom severity of inflammatory bowel disease, proton pump inhibitor usage, and visceral sensitivity</b></p><p>Peter Sternes<sup>3</sup>, <b>Ayesha Shah</b><sup>1,2</sup>, Camila Ayela Pintos<sup>3</sup>, Thomas Fairlie<sup>1</sup>, Natasha Koloski<sup>1</sup>, Seungha Kang<sup>2</sup>, Simon McIlroy<sup>3</sup>, Mark Morrison<sup>2</sup>, Gene Tyson<sup>3</sup> and Gerald Holtmann<sup>1,2</sup></p><p><sup>1</sup><i>Princess Alexandria Hospital, Metro South Health, Woolloongabba, Australia;</i> <sup>2</sup><i>University of Queensland, Brisbane, Australia;</i> <sup>3</sup><i>Queensland University of Technology, Brisbane, Australia</i></p><p><b><i>Background and Aims:</i></b> We aimed to assess and compare the biogeography of the mucosa associated microbiome (MAM) in patients with inflammatory bowel disease (IBD) and controls in different segments of the gastrointestinal tract, and explore the links between the MAM, gastrointestinal symptoms and use of proton pump inhibitors (PPI).</p><p><b><i>Methods:</i></b> We recruited 59 controls (without structural abnormalities and gastrointestinal symptoms),44 patients with ulcerative colitis (UC) and 31 with Crohn’s disease (CD). Biopsies from various segments of the upper and lower gastrointestinal tract were collected. Microbial composition was assessed via 16S rRNA gene amplicon analysis and the bacterial load of the mucosal biopsies were assessed via qPCR. The MAM was examined in the context of disease status, PPI usage, the severity of gastrointestinal symptoms, and the symptom response to a standardized nutrient challenge (SNC).</p><p><b><i>Results:</i></b> Microbial communities of the MAM in the upper and lower gastrointestinal tract are different. Compared to controls, IBD patients were characterised by relative and absolute depletion of numerous butyrate and/or propionate producing genera, with the largest differentiation being the depletion of <i>Faecalibacterium</i> in the lower GI tract of CD patients. PPI users had enrichment of <i>Faecalibacterium</i>in the lower GI tract. The severity of gastrointestinal symptoms, as well as the symptom response to the SNC, were significantly associated with MAM composition in the GI tract.</p><p><b><i>Conclusion:</i></b> The absolute and relative composition of the MAM is variable across different segments of the GI tract and is different in patients with IBD and controls. Gastrointestinal symptoms are associated with quantitative changes of bacterial taxa along the GI tract.</p><p><b>125</b></p><p><b>Frequency of NUDT15 polymorphisms in a multicultural Australian IBD population</b></p><p><b>Tessa Greeve</b><sup>1,2</sup>, Georgia Sun<sup>1</sup> and Gregory Moore<sup>1,2</sup></p><p><sup>1</sup><i>Monash Health, Melbourne, Australia;</i> <sup>2</sup><i>Monash University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Thiopurine medications are commonly used in the management of Inflammatory Bowel Disease (IBD), however can be associated with serious adverse effects including life threatening myelosuppression. Thiopurine S-methyltransferase (<i>TPMT</i>) and nudix hydrolase 15 <i>(NUDT15)</i> are enzymes important in thiopurine metabolism. Genetic variants, resulting in reduced or absence enzyme activity, can lead to an excess of cytotoxic metabolites and are strongly associated with myelosuppression (1). Variants in <i>NUDT15</i> occur more frequently in those of Asian ancestry, whilst <i>TPMT</i> variants are more common in those of European heritage (2). Australian guidelines recommend pre-treatment <i>TPMT</i> genotyping to help predict the risk of severe thiopurine-induced toxicity (3). However, though this risk exists and is even greater for those with variants in <i>NUDT15</i> (2), until recently this test has not been readily available in Australia. This study aimed to determine the frequency of <i>NUDT15</i> variants in the Australian IBD population.</p><p><b><i>Methods:</i></b> Participants were identified from a database of patients enrolled in a thiopurine monitoring service within a tertiary hospital in Melbourne. Participants underwent concomitant <i>NUDT15</i> and <i>TPMT</i> genotyping via a commercial pathology service. Presence of 8 <i>NUDT15</i> variants was assessed. Country of birth and ethnicity, where available, was obtained from medical records.</p><p><b><i>Results:</i></b> 93 individuals with IBD underwent combined <i>NUDT15</i> and <i>TPMT</i> testing. 54 participants (58.1%) were born in Australia, of the remaining participants the majority, 28 (30.1%), were born in Asia and 6 (6.5%) in Europe. Ethnic background was not routinely recorded and was available in a minority of participants (6.45%). 10 (10.75%) participants were found to have a variant in <i>NUDT15</i> whilst 3 (3.26%) participants had a variant in <i>TPMT</i>. The most common <i>NUDT15</i> variant identified was the *3 allele, with 6 participants heterozygotes (*1/*3) (Table 1). 2 participants were heterozygotes carrying the *6 allele. The *9 allele was found in 1 individual, whilst 1 individual had a variant identified as either *1/*2 or a compound homozygote *3/*6. Of those with <i>NUDT15</i> variants identified, 5/10 were born in Australia, with 1 individual born in each of Afghanistan, Bangladesh, China, India and Malaysia.</p><p><b><i>Conclusions:</i></b> The prevalence of <i>NUDT15</i> variants in our IBD population was significantly higher than that previously reported in an Australian IBD population (4) likely due to a predominance of European ancestry in the previously studied cohort. In this study, half of those with <i>NUDT15</i> alleles were born in Australia, likely representing ancestral migration from higher risk countries. These results suggest that given the multicultural nature of the Australian population, <i>TPMT</i> testing alone is inadequate to identify individuals at risk of thiopurine associated harm.</p><p>\n \n </p><p><b>References</b></p><p>\n 1. <span>Van Gennep, S</span>, <span>Konté, K</span>, <span>Meijer, B</span>, <span>Heymans, MW</span>, <span>D'Haens, GR</span>, <span>Löwenberg, M</span>, et al. <span>Systematic review with meta-analysis: risk factors for thiopurine-induced leukopenia in IBD</span>. <i>Aliment Pharmacol Ther.</i> <span>2019</span>; <span>50</span>(<span>5</span>): <span>484</span>-<span>506</span>.</p><p>\n 2. <span>Yang, S-K</span>, <span>Hong, M</span>, <span>Baek, J</span>, <span>Choi, H</span>, <span>Zhao, W</span>, <span>Jung, Y</span>, et al. <span>A common missense variant in NUDT15 confers susceptibility to thiopurine-induced leukopenia</span>. <i>Nature Genetics.</i> <span>2014</span>; <span>46</span>(<span>9</span>): <span>1017</span>-<span>20</span>.</p><p>\n 3. <span>Gastroenterological Society of Australia Inflammatory Bowel Disease Clinical Update 2018</span>. <span>2018</span>.</p><p>\n 4. <span>Afrin, S</span>, <span>Simms, LA</span>, <span>Lord, A</span>, <span>Radford-Smith, GL</span>. <span>Nudix hydrolase 15 (NUDT15) loss-of-function variants in an Australian inflammatory bowel disease population</span>. <i>Internal Medicine Journal</i> <span>2022</span>; <span>52</span>(<span>11</span>): <span>1971</span>-<span>7</span>.</p><p><b>254</b></p><p><b>Allosteric modulation of cannabinoid 1 receptor as a novel therapeutic strategy for inflammatory bowel disease</b></p><p><b>Dinesh Thapa</b><sup>1</sup>, Leon Warne<sup>1</sup>, Mohan Patil<sup>1</sup>, Marco Falasca<sup>2</sup> and Rodrigo Carlessi<sup>1</sup></p><p><sup>1</sup><i>Curtin University, Bentley, Australia;</i> <sup>2</sup><i>University of Parma, Parma, Italy</i></p><p><b><i>Background and Aim:</i></b> Novel therapies for inflammatory bowel disease (IBD) are urgently needed, as current treatments mainly provide symptomatic relief. The cannabinoid 1 receptor (CB1R), part of the endocannabinoid system, is shown to be dysregulated in IBD. While tetrahydrocannabinol (THC) has been shown to reduce IBD, mainly through orthosteric modulation of CB1R, their therapeutic applications are limited by behavioural side effects. Drugs targeting the allosteric site of CB1R have shown benefits in different diseases without behavioural side effects. This study investigated the role of the CB1R allosteric modulator ZCZ011, alone or in combination with sub-therapeutic THC, in treating IBD using a murine IBD model.</p><p><b><i>Methods:</i></b> Female BALB/c mice aged 8-10 weeks were challenged with 4% dextran sodium sulphate (DSS) in drinking water for 7 days, followed by three days of normal water. THC (2.5, 5 and 10mg/kg) and/or ZCZ011 (20, 30 and 40 mg/kg) were administered intraperitoneally (i.p.), alone or in combination, daily for 11 days. Body weight, stool consistency and the presence of occult blood/rectal bleeding were scored daily to calculate the disease activity index (DAI). On day 11, mice were euthanized, and colon, spleen, kidneys, and liver were assessed for inflammation using myeloperoxidase (MPO) activity assay as well as organ weight/length measurement. Cytokines and chemokines expressions in colon lysates were assessed using multiplex assay. Toxicological parameters including complete blood count (CBC) and liver/kidney biochemistry profiles were measured.</p><p><i><b>Results</b>:</i> DSS-challenged mice showed increased DAI score, inflammation, and pain behaviors with decreased colon length, increased MPO activity and cytokines expression and elevated Liver and spleen weights. THC at 10mg/kg, but not 2.5 and 5 mg/kg, significantly reduced IBD as indicated by decreased DAI score, MPO activity and increased colon length. The effects of ZCZ011 alone diminished after day 8. However, a combination of 2.5mg/kg THC and 20 mg/kg ZCZ011 significantly reduced IBD as evidenced by decreased DAI score, absence of pain behaviors, increased colon length and decreased MPO activity. Body and organ weights remained comparable to healthy controls. No toxicity was observed with THC and ZCZ011, specifically the combination of 2.5 mg/kg THC and 20 mg/kg ZCZ011.</p><p><b>262</b></p><p><b>Antigen-specific regulatory T cell therapy for inflammatory bowel disease</b></p><p>Marie Lee<sup>2</sup>, Indiana Zorkau<sup>2</sup>, Joshua Ooi<sup>2</sup>, Peter Eggenhuizen<sup>2</sup> and <b>Rimma Goldberg</b><sup>1</sup></p><p><sup>1</sup><i>Department of Gastroenterology, Monash Health, Clayton, Australia;</i> <sup>2</sup><i>Department of Medicine, Center for Inflammatory Diseases, Monash University, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> Inflammatory bowel disease (IBD) is driven by the imbalance of inflammatory effector T cell responses and regulatory T cells (Tregs) that are unable to adequately downregulate immune-mediated pathology. Current treatments for IBD, which focus on widespread immunosuppression or blockade of specific pro-inflammatory cytokines, fail in over half of patients as this imbalance in the T cell-based immune response is not adequately addressed. Previous Treg trials in IBD using thymic-derived Tregs (tTregs) has been shown to be a safe and efficacious option to reset the aberrant immune response without drug toxicities, however, a key barrier is the difficulty in isolating a sufficient number of Tregs as these cells only comprise 5-10% of circulating CD4+ T cells. We aimed to explore a novel therapeutic approach utilising gut-homing antigen-specific induced regulatory T cells (iTregs) for the treatment of IBD in <i>in vitro</i> studies.</p><p><b><i>Methods:</i></b> Naïve CD4+ T cells and tTregs were isolated from buffy coats of healthy donors and transduced with a gut-homing antigen-specific T cell receptor (TCR). tTregs were cultured in IL-2, rapamycin and aCD3/aCD28 Dynabeads, and naïve CD4+ T cells were differentiated into iTregs and cultured in the same additives and TGF-β for a total period of 14 days. Growth fold change from the start to end of culture was measured. Flow cytometry was used to phenotypically assess FOXP3 and TCR expression. Tregs were also assessed for IL-17 and IFN-γ production after a 5-day challenge with a pro-inflammatory cytokine cocktail (IL-2, TGF-β, IL-1β, IL-6, IL-21, IL-23) and 4-hour stimulation with phorbol 12-myristate 13-acetate, ionomycin and brefeldin A. Suppressive function of Tregs was assessed in 5-day <i>in vitro</i> co-cultures with antigen-specific effector T cells. P≤0.05 was considered statistically significant.</p><p><b><i>Results:</i></b> Samples were collected from a total of 7 healthy donors. Median growth fold change of antigen-specific TCR-transduced iTregs cultured over a period of 14-days was found to be significantly greater compared to tTregs (96.00 [72.00, 270.00] vs 43.67 [17.62, 102.00], P=0.0175), and at the end of 14-day culture, transduced iTregs demonstrated comparable FOXP3 expression compared to tTregs (85.20 [70.70, 98.80] vs 89.90 [60.50, 99.00], P = 0.9452). In the presence of a pro-inflammatory cytokine cocktail for a duration of 5 days and additional challenge with 4-hour stimulation, iTregs showed lower IFN-γ expression (0.4800 [0.19, 0.81] vs 2.470 [0.48, 14.70], P=0.2857) and lower IL-17 than tTregs (0.08300 [0.083, 0.680] vs 3.535 [2.71, 7.67], P=0.0571). In <i>in vitro</i> suppression assays, antigen-specific TCR-transduced iTregs demonstrated a trend of greater suppression than non-antigen-specific iTregs.</p><p><b>268</b></p><p><b>Multiomic modelling of antibiotic perturbed faecal microbial communities demonstrates reduced microbial resilience in inflammatory bowel disease</b></p><p><b>Sabrina Koentgen</b><sup>1</sup>, Fan Zhang<sup>1</sup>, Swisha Khadka<sup>1</sup>, Xiaotao Jiang<sup>1</sup>, Thisun Jayawardana<sup>1</sup>, Emma Allen-Vercoe<sup>2</sup>, Claire O'Brien<sup>3</sup> and Georgina Hold<sup>1</sup></p><p><sup>1</sup><i>Microbiome Research Centre, UNSW, Sydney, Australia;</i> <sup>2</sup><i>University of Guelph, Guelph, Canada;</i> <sup>3</sup><i>Australian National Univsersity, Canberra, Australia</i></p><p><b><i>Background and Aim:</i></b> Ciprofloxacin (CIP) and Metronidazole (MTZ) are two antibiotics commonly used in the treatment of bacterial gastroenteritis. Both CIP and MTX are commonly used as adjuvant therapeutics for inflammatory bowel disease (IBD). However, excessive antibiotic use is also often noted as a potential risk factor in IBD, due to the impact on gastrointestinal microbiota. Disruption of gut bacteria, commonly referred to as dysbiosis, is a widely described phenomena in IBD. The role this dysbiosis plays in IBD progression and severity is still unknown. Here we investigate the impact of these commonly prescribed antibiotics on gut microbiota structure/function in a healthy donor and a new-onset therapeutic naïve IBD patient. We also investigate the use of autologous faecal microbial transplant (aFMT) as a microbial therapeutic to assist recovery of the gut ecosystem after antibiotic-induced perturbation.</p><p><b><i>Methods:</i></b> <i>In vitro</i> modelling of gut microbial communities was achieved using continuous culture chemostat models. Donor faecal specimens (IBD or healthy control; collected as part of the Australian IBD Microbiome Study) were used to inoculate twin chemostat vessels (10% w/v) containing culture medium imitating an industrialised diet. The faecal microbial communities were allowed to stabilise for 15 days. On day 16, vessels were dosed daily with antibiotics (CIP or MTZ, for 7 days, therapeutic dosing levels). In the healthy donor vessel, 4 doses of aFMT were administered over 7 days (post antibiotics) followed by a 7-day recovery. In the IBD vessels no FMT was administered, and vessels were monitored for 7 days. Vessels were sampled daily to measure total bacterial counts, monitor microbial profiles (16S rRNA gene V3/4 profiles; Illumina MiSeq) and short chain fatty acid (SCFA) profiles (GC-MS). The Microbiome Research Centre 16S analysis pipeline and R studio were used for microbiome statistical analysis and data visualisation. Agilent MassHunter workstation was used for SCFA quantitation. Statistical analysis and visualisation were performed in R studio.</p><p><b><i>Results:</i></b> When 16S rRNA gene sequence and SCFA datasets were compared, stable state microbial profiles were very different between donors, however the stable state of replicate vessels from both the healthy and IBD donors were not significantly different (p>0.05) confirming the parallelism. CIP and MTZ dosing of the healthy donor vessel impacted SCFA profiles differently. CIP caused a significant depletion of several SCFAs including acetate, butyrate, and propionate, these metabolites remained significantly depleted following aFMT. During the recovery phase levels of acetate and propionate recovered whilst butyrate remained significantly depleted (p=0.004). In the healthy MTZ vessel, acetate increased during antibiotic dosing and was restored following aFMT remaining elevated during recovery. Butyrate and valerate decreased during MTZ administration and remained significantly decreased (p<0.011). Propionate levels also reduced following MTZ but were found in highest abundance during aFMT and recovery phases (p<0.038). CIP dosing of the healthy vessel resulted in an enrichment of <i>Escherichia-Shigella</i> and <i>Enterobacter</i> with an equivalent loss of <i>Akkermansia, Faecalibacterium</i> and <i>Bacteroides</i>. Differential abundance analysis highlighted increased <i>Parabacteroides</i> during MTZ dosing which subsequently decreased to match steady state by recovery. <i>Akkermansia</i> levels significantly increased in recovery phase compared to aFMT and stability phases. In the IBD donor vessels, CIP caused a significant reduction in 10 SCFAs and of several taxon signatures including those for <i>Bacteroides</i> and <i>Dialister</i> genera alongside an enrichment of <i>Enterococcus, Lachnospiraceae, Anaerofilum</i> and <i>Eisenbergiella</i>. MTZ treatment of the IBD vessel resulted in a much less dramatic reduction in SCFAs. Microbial community changes included an enrichment of <i>Escherichia-Shigella, Enterococcus and Parasutterella</i> and a depletion of <i>Alistipes</i> and <i>Dialister</i>.</p><p><i><b>Conclusion</b>:</i> The broad-spectrum action of CIP caused significant and consistent depletion of beneficial genera and SCFAs across donors. Neither donor community was able to restore composition or function to match the stable state during the experimental period. MTZ showed more complex interactions at play with only portions of the community targeted and overall less dramatic microbial changes. Both CIP and MTX significantly depleted levels of beneficial genera including <i>Akkermansia</i> and <i>Alistipes</i> and reduced the abundance of beneficial/anti-inflammatory SCFAs. Redundancy in the microbial community potentially allowed recovery from a less aggressive perturbation with MTZ. aFMT appeared to modulate the healthy donor microbial communities to a “new healthy”. Further investigation into long-term antibiotic treatment and the use of microbial therapeutics is needed to fully understand this relationship in the context of IBD.</p><p><b>307</b></p><p><b>Active maternal IBD does not affect infant immune cell development</b></p><p><b>Ralley Prentice</b><sup>1,2,3,4</sup>, Sally Bell<sup>1,2</sup>, Steven Cho<sup>2,4</sup>, Megan Burns<sup>1</sup>, Marie Lee<sup>4</sup>, Indiana Zorkau<sup>4</sup>, Claudia Nold<sup>2,4</sup>, Emily Wright<sup>2,5</sup>, Emma Flanagan<sup>2,5</sup>, Alyson Ross<sup>3</sup>, Marcel Nold<sup>2,4</sup> and Rimma Goldberg<sup>1,2,4</sup></p><p><sup>1</sup><i>Monash Health;</i> <sup>2</sup><i>Monash University;</i> <sup>3</sup><i>St Vincent's Hospital Melbourne;</i> <sup>4</sup><i>Hudson Institute of Medical Research;</i> <sup>5</sup><i>University of Melbourne</i></p><p><b><i>Background and Aim:</i></b> Maintaining control of inflammatory bowel disease in pregnancy with the use of pharmacotherapies is crucial to optimising obstetric and neonatal outcomes. A detailed understanding of the effect of specific therapies and active disease on maternal immunophenotype and infant immune development is lacking. With comprehensive flow cytometric assessment, we aimed to define how IBD, it’s treatment, and disease activity impact both maternal and infant immunophenotype and cytokine production.</p><p><b><i>Methods:</i></b> IBD and healthy control mother-infant dyads were recruited from Jan 2022- March 2023. IBD activity related data and peripheral blood for flow cytometry immunophenotyping and quantification of cytokine response to stimulation were obtained in each trimester of pregnancy (T1,2,3), at delivery (D) and at six weeks post-partum (PP). Active disease was defined by a fecal calprotectin >100ug/g. Cord and six-week peripheral blood samples were taken from resultant offspring.</p><p><b><i>Results:</i></b> Sixteen IBD (9/16 exposed to biologic and 9/16 with CD) and two healthy control mother-infant dyads were recruited. 6/16 IBD pregnancies had active disease. Two participants required biologic dose frequency escalation in first trimester. Another underwent infliximab induction. Rates of adverse obstetric, neonatal and infant outcomes were equivalent to the Australian population with 11/16 IBD-exposed infants breastfed at six weeks old. Overall, minimal differences in adult and infant immune cell profiles and activity were observed according to active disease and medical therapy exposure, and in comparison to healthy controls. However, there were important exceptions. Basal Treg population proportions were 46% lower in those participants exposed to ustekinumab in pregnancy (0.21% vs 0.39%, Wilcoxon rank-sum <i>P</i>=0.027), with a trend seen with PMA/Ionomycin stimulation (0.26% vs 0.60%, p=0.0513). The proportion of CD4<sup>+</sup> (p=0.036) and CD8<sup>+</sup> (<i>P</i>=0.0495) T cells expressing unbound α4β7<sup>+</sup> were lower in the participant exposed to vedolizumab. Basal (1.75% vs 0.47%, <i>P</i>=0.036) and responsiveness of cDCs and non-classical monocytes to LPS stimulation (72.2% vs 64.7%, <i>P</i>=0.028) were increased 3.7- and 1.1 fold respectively in those with an elevated faecal calprotectin. From T2 to T3, the proportion of IFN-γ<sup>+</sup> CD4<sup>+</sup> (T helper-1) (median 0.06% to 1.54%, paired t-test <i>P</i>=0.028) and IFN-γ<sup>+</sup> CD8<sup>+</sup> (0.05% to 1.54%, <i>P</i>=0.0012) T cells with PMA/INO stimulation increased 30-fold. The proportion of α4β7<sup>+</sup> cDC and non-classical monocytes following LPS stimulation increased four-fold from T2 to PP (2.5% to 10.5%, <i>P</i>=0.047). Maternal and infant α4β7<sup>+</sup> cDC and non-classical monocyte population proportion strongly correlated following LPS stimulation at delivery (r=0.82, p=0.0416). In infants, basal CD4<sup>+</sup>α4β7<sup>+</sup> (41.4% to 66.5%, <i>P</i>=0.0043) and CD8<sup>+</sup>α4β7<sup>+</sup> (81.2% to 93.6%, <i>P</i>=0.007) population proportions increased approximately 1.6- and 1.2-fold respectively from D to PP, whilst CD4<sup>+</sup>p40<sup>+</sup> population proportions decreased 58% (0.36% to 0.15%, <i>P</i>=0.022) and PMA/Ionomycin stimulated CD4<sup>+</sup> GATA3<sup>+</sup> (T helper-2) population proportions increased 2.75 fold (0.9% to 2.47%, <i>P</i>=0.024). In the infant exposed to vedolizumab, unbound α4β7 expression was negligible on CD4<sup>+</sup> and CD8<sup>+</sup> T cells (Figure 1), with no other significant differences in immune cell population proportions noted according to in-utero pharmacotherapy exposure.</p><p><b>387</b></p><p><b>Comparison of drug tolerant assays for the measurement of bound anti-infliximab antibodies in patient serum</b></p><p><b>Melissa Sam</b><sup>1,2,3</sup>, Karla Cameron<sup>6,7</sup>, Mark Ward<sup>6,7</sup>, Therese Rexhepi<sup>1,2,3</sup>, Bonita Gu<sup>2,5</sup>, Craig Haifer<sup>2,8</sup>, Susan J Connor<sup>2,5</sup>, David Harman<sup>4</sup>, William Donald<sup>2</sup> and Catherine Toong<sup>1,2,3,5</sup></p><p><sup>1</sup><i>NSW Health Pathology, Liverpool, Australia;</i> <sup>2</sup><i>University of New South Wales, Randwick, Australia;</i> <sup>3</sup><i>Ingham Institute of Applied Medical Research, Liverpool, Australia;</i> <sup>4</sup><i>Western Sydney University, Campbelltown, Australia;</i> <sup>5</sup><i>Liverpool Hospital, South-Western Sydney LHD, Liverpool, Australia;</i> <sup>6</sup><i>Monash University, Melbourne, Australia;</i> <sup>7</sup><i>Alfred Health, Melbourne, Australia;</i> <sup>8</sup><i>St Vincent's Hospital, Sydney, Australia</i></p><p><b><i>Background and Aim:</i></b> Anti-infliximab antibodies (ATI) are associated with immunogenic failure to infliximab and poor outcomes in patients with inflammatory bowel disease. Current drug sensitive ELISA tests cannot detect ATI in the presence of circulating IFX. Drug tolerant ELISAs offer the advantage of detecting total ATI, i.e. that which is bound to drug or non-neutralising ATIs. Up to 30% of patients have undetectable ATI levels on drug sensitive ELISA. The two methods tested were the anti-Lambda method (LAMBDA) and the acid-dissociation method (ACID). The LAMBDA method is based on the principle that IFX consists of only kappa light chains whereas in polyclonal human IgG, kappa and lambda light chains exist in a ratio of 2:1. ATIs bound to IFX on the plate are then detected using an anti-lambda detection antibody. The ACID method involves the breaking of IFX-ADA complexes by dropping the pH of the sample. Samples are neutralized prior to running a standard ELISA method. The aim of this study was to compare different drug tolerant methods in measuring ATI.</p><p><i><b>Methods:</b></i> Patient samples from an Australian tertiary centre (Ethics 2021/ETH012703) were included if they had > 6 months steroid free clinical (Harvey Bradshaw Index ≤ 4 / Partial Mayo Score ≤ 2) and biochemical remission (C-reactive protein <5 mg/L or faecal calprotectin <150 μ/g), and had either undergone immunomodulator withdrawal and continuation of intravenous (IV) infliximab monotherapy with a therapeutic drug monitoring sample collected within the 3 months prior, or continued on combination therapy with IV infliximab and an immunomodulator. Samples were tested using two previously published drug tolerant methods – an acid dissociation (ACID) and an anti-lambda detection (LAMBDA) method. Infliximab levels were assessed between samples positive on either of the drug tolerant methods.</p><p><b><i>Results:</i></b> There was no correlation between ATI positive samples on the anti-lambda detection method and the acid dissociation method (R<sup>2</sup> of 0.007) i.e. samples that were positive on the LAMBDA method were not positive on the ACID method with one exception in our cohort. Samples in the immunomodulator withdrawal group had a 16% positivity rate in the LAMBDA method (of total number tested n= 55) compared to 8% in the ACID method group (of total number tested n = 25). In the control group positivity rates were 8% and 0% in the LAMBDA method (of total number tested n = 57) and the ACID method (of n = 20) respectively. The LAMBDA method was able to detect positive ADAs at drug levels up to 22.8 mg/L compared to the ACID method at 3 mg/L. Mean drug level that reached positivity in the LAMBDA and the ACID methods were 5.7 mg/L ± 1.3 SEM vs 2.1mg/L ± 0.8 SEM respectively, however this was not significant due to the small sample size.</p><p><b><i>Conclusion:</i></b> Current assays offer no consensus on positivity for bound ATIs. The higher positivity rate in the LAMBDA method may be due to non-neutralising antibodies, the clinical significance of which is unclear. The ACID method involves the breaking of IFX-ADA complexes and detects neutralizing antibodies and so may provide more clinically relevant information. This method, however, is more sensitive to circulating IFX levels and is affected by the reassociation of complexes that form when neutralizing the sample prior to the ELISA method. Essentially, current methods are variable and produce discordant results. Further studies are required to investigate these assays and to develop further tests to provide more information on the development of ATIs and their clinical relevance. Our group is currently working on mass spectrometry methods to further clarify the development of ADAs and their effect on circulating drug levels.</p><p><b>453</b></p><p><b>Age-dependent dysregulation of the UPR in colonic epithelium: Implications for mucosal integrity</b></p><p><b>Thishan Illankoon</b><sup>1,2</sup>, Kuan Yau Wong<sup>1,2</sup>, Haressh Sajiir<sup>1,2</sup>, Alexandra Mueller<sup>1,2</sup>, Anna Amiss<sup>1,2</sup>, Jakob Begun<sup>1,2</sup>, Rabina Giri<sup>1,2</sup>, Lucy Burr<sup>1,2</sup> and Sumaira Hasnain<sup>1,2</sup></p><p><sup>1</sup><i>Mater Research Institute (Translational Research Institute), Brisbane, Australia;</i> <sup>2</sup><i>University of Queensland, Brisbane, Australia</i></p><p><b><i>Background and Aim:</i></b> Misfolded protein accumulation in the endoplasmic reticulum (ER) due to various endogenous and exogenous factors triggers ER stress, a hallmark of numerous diseases, including inflammatory bowel disease (IBD). Eukaryotic cells combat this stress via the unfolded protein response (UPR), a regulatory network that promotes correct protein folding and maintains cellular homeostasis. Age-related increases in protein aggregates, even in healthy individuals, suggest a decline in UPR function as a natural consequence of aging. Research has explored the UPR’s role in neurodegenerative diseases. However, the impact of an aging UPR on mucosal epithelial cells in the intestine remains largely unexplored. We hypothesise that the age-related UPR senescence contributes to the heightened susceptibility to infections and increased disease severity observed in aged individuals. In this study, we comprehensively characterized age-related changes in the UPR of intestinal epithelial cells from both healthy mice/humans and those with intestinal inflammation.</p><p><b><i>Methods:</i></b> To investigate our aims, both human samples and mouse models have been utilised. Human colon biopsies were accessed via the Mater Research IBD biobank which included a wide range of patient samples, both with and without IBD. They were sorted into three age groups (young = <25; middle aged = 30-50; aged = >65). For the mouse models, C57BL/6 (control) and <i>Winnie</i> (model of spontaneous colitis via a mutation in the <i>Muc2</i> gene) mice, intestinal epithelial cells were isolated from 4-, 8-, 12-, 24-, 44-, and 60-weeks old animals. qRT-PCR was utilized to assess the changes in the UPR-related genes, and histological analyses of intestinal proteins was conducted using immunohistochemistry and immunofluorescence.</p><p><b><i>Results:</i></b> qPCR analysis of colonic epithelial cells in aging C57BL/6 mice, revealed a significant upregulation of various UPR markers until around 44-weeks of age. This upregulation was followed by a decrease in specific markers at 60-weeks. Compared to age-matched controls, <i>Winnie</i> mice exhibited a significant reduction in the expression of downstream UPR markers, particularly in older age group. Mucin production in the C57BL/6 mice declined throughout aging, with a more pronounced decreased observed in <i>Winnie</i> mice. Analysis of human colon biopsies revealed an age-related increase in protein folding chaperones, suggesting heightened ER stress. Interestingly, there was a trend of decline in downstream UPR markers, potentially indicating a compromised UPR in older individuals.</p><p><i><b>Conclusion:</b></i> Our findings support the hypothesis that the UPR becomes less effective with age in colonic epithelial cells. This conclusion is based on the observed increase in ER stress markers alongside a decrease in downstream UPR activity and mucin production. These age-related changes may contribute to the increased susceptibility to infections and disease severity reported in older individuals. Further investigation is ongoing to elucidate the mechanisms behind this decline, with a particular emphasis on infection management, metabolic alterations, and epigenetic factors. This comprehensive approach will enhance understanding of the complex interplay between UPR dysfunction and aging in the colonic mucosa.</p><p><b>489</b></p><p><b>Deep functional analysis of a defined sulphide-reducing diet (4-SURE diet) as a novel therapy for ulcerative colitis demonstrates all specific luminal micro environmental objectives were achieved</b></p><p><b>Alice Day</b><sup>1,2,3</sup>, Rachael Slater<sup>4</sup>, Vanessa Marcelino<sup>5,6</sup>, Reuben Wheeler<sup>7</sup>, Remy Young<sup>5,8</sup>, Natasha Maddigan<sup>2,3</sup>, Samuel Forster<sup>5,8</sup>, Samuel Costello<sup>1,2,3</sup>, Wendy Uylaki<sup>1,3</sup>, Chris Probert<sup>4</sup>, Jane Andrews<sup>2,9</sup>, Chu K Yao<sup>10</sup>, Peter Gibson<sup>10</sup> and Robert Bryant<sup>1,2,3</sup></p><p><sup>1</sup><i>Inflammatory Bowel Disease Services, Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Adelaide, Australia;</i> <sup>2</sup><i>School of Medicine, Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;</i> <sup>3</sup><i>Basil Hetzel Research Institute, Adelaide, Australia;</i> <sup>4</sup><i>Institute of Systems, Molecular and Integrative Biology, Department of Molecular and Clinical Cancer, University of Liverpool, Liverpool, United Kingdom;</i> <sup>5</sup><i>Centre for Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Clayton, Australia;</i> <sup>6</sup><i>Melbourne Integrative Genomics, School of BioSciences & Department of Microbiology and Immunology at The Peter Doherty Institute, The University of Melbourne, Melbourne, Australia;</i> <sup>7</sup><i>College of Science and Engineering, Flinders University, Adelaide, Australia;</i> <sup>8</sup><i>Department of Molecular and Translational Sciences, Monash University, Clayton, Australia;</i> <sup>9</sup><i>Inflammatory Bowel Disease Service, Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;</i> <sup>10</sup><i>Department of Gastroenterology, School of Translational Research, Monash University & Alfred Health, Melbourne, Australia</i></p><p><b><i>Background and Aim:</i></b> As a dietary approach to reducing inflammation in ulcerative colitis (UC), the 4-SURE diet was designed to correct pathogenic alterations of excessive protein fermentation and hydrogen sulphide (H<sub>2</sub>S) production in the distal colon. The specific dietary objectives were achieved (Day et al, <i>J Nutr</i> 2022;152:1690<i>)</i> but it is uncertain whether these mechanistic objectives could be achieved with 8 weeks of diet. Therefore, we aimed to perform a deep functional analysis (microbial and metabolomic) of the faeces.</p><p><b><i>Methods:</i></b> Faecal samples of 28 adults with mild-moderately active UC were collected at week 0 and 8 of dietary intervention, processed and aliquoted. Shotgun metagenomic sequencing was used to identify genes involved in H<sub>2</sub>S metabolism. Metagenomic reads were trimmed and reads mapping to the human genome removed. Gene identification was performed using Diamond v2.1.9 for alignment against a database of genes involved in global sulphur cycling. Gas-chromatography mass-spectrometry was used to characterise volatile organic compounds (VOCs) with specific analysis of products of protein fermentation. Capacity of the microbiota to produce H<sub>2</sub>S was determined by incubating homogenates anaerobically for 24hours, then total H<sub>2</sub>S production was measured spectrophotometrically.</p><p><b><i>Results:</i></b> Majority of microbiome members at week 0 and 8 belonged to the <i>Bacteroidota</i> and <i>Bacillota phyla</i>. There were no differences in bacterial diversity (p=0.16). However, by Random Forest Plot Classifier, known H<sub>2</sub>S producers, <i>Odoribacter</i> and <i>Peptostreptococcaceae,</i> were taxa of highest importance in discriminating between beforediet and after-diet samples, where abundance was markedly lower. The capacity for H<sub>2</sub>S metabolism altered, with significant differences (p<0.05, Wilcoxon signed-rank with BenjaminiHochberg correction) in 6 of 23 analysed sulphur-metabolising genes involved in H<sub>2</sub>S cycling, including <i>iscS</i>, <i>cysK</i> (Fig. 1), <i>metC</i>, <i>luxS, asrC</i> and <i>sseA</i>. Composition of 173 identified faecal VOCs differed before and after diet; indole (a specific marker of protein fermentation) decreased from 0.42 [-0.25,0.61] at week 0 to -0.28 [-0.77,0.48] at week 8 (p=0.007, FDR correction; Fig. 1). Faecal H<sub>2</sub>S reduced from median 2.61 (interquartile range 2–4.96)μmol to 1.41 (0.81-2.27)μmol of H<sub>2</sub>S/g stool (wet weight) (p=0.002) (Fig. 1).</p><p><b>504</b></p><p><b>RNA sequencing of mucosal biopsies: an unbiased approach in the assessment of host molecular inflammatory state in the investigation of host-microbiota interactions in ulcerative colitis</b></p><p><b>Patricia Khoo</b><sup>1,2,3</sup>, Linden Gearing<sup>1,3</sup>, Jodee Gould<sup>1,3</sup>, Emily Rutten<sup>1,3</sup>, Samuel Forster<sup>1,3</sup> and Edward Giles<sup>1,2,3</sup></p><p><sup>1</sup><i>Centre for Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Clayton, Australia;</i> <sup>2</sup><i>Department of Paediatrics, Monash University, Clayton, Australia;</i> <sup>3</sup><i>Department of Molecular and Translational Sciences, Monash University, Clayton, Australia</i></p><p><b><i>Background and Aim:</i></b> Inflammatory bowel disease (IBD) is caused by an aberrant immune response in genetically susceptible individuals to the environment, including their microbiota. In recent years an explosion in microbiome research in IBD has yet to change diagnostic algorithms nor resulted in new treatments. The majority of studies have focused on stool samples, hence lacking the representation of mucosa-associated microbiota and the characterisation of host-microbiota interaction at the mucosal interface. To address these challenges, we propose an approach of paired measurement of site-specific host transcriptional response along with its mucosa-associated microbiota.</p><p><b><i>Methods:</i></b> Fresh rectal biopsies were obtained from adults with ulcerative colitis and controls at a tertiary gastroenterology endoscopy service. Four mucosal samples were obtained from each patient, at the site of inflammation if inflammation was observed. Two biopsies were sent for anatomical pathology review. Matched mucosal culturing of mucosa-associated bacteria (Figure 1a) and RNA sequencing of host transcriptional profiling were performed. RNA sequencing analysis was performed in R (v4.3.2). The Hallmark Inflammatory Response gene set from the Hallmark gene set collection was used to classify samples as molecularly inflamed or non-inflamed. Log<sub>2</sub> expression of the 164 detected inflammatory response genes were clustered using <i>k</i>-means, with <i>k</i>=2.</p><p><b><i>Results:</i></b> Samples were collected from a total of 98 patients: 52 with ulcerative colitis (UC) and 46 controls (CO). The mean age of UC patients was 36.3 years (21-75), and 42.3% were female. The mean age of CO patients was 36.4 years (18-56), and 54.3% were female. A multidimensional scaling (MDS) plot was constructed based on the top 500 most variable genes from the filtered and normalised data, coloured by variables. Principal coordinate analysis (PCA) plot was then generated using the Hallmark Inflammatory Response gene set. It demonstrated a cluster of molecularly inflamed (IR) samples, which comprised mostly of the histologically inflamed UC samples but there are some histologically inflamed samples that did not belong to the molecularly inflamed cluster. The first principal component of the PCA plot correlated very well with the first dimension of the MDS plot (Figure 1b), indicating that these inflammatory genes are a major source of variation across the data.</p><p><b>545</b></p><p><b>Topical upadacitinib is effective in distal ulcerative colitis: A case study and pre-clinical proof of concept</b></p><p><b>Rabina Giri</b><sup>1</sup>, Anna Amiss<sup>1</sup>, Bruce Riches<sup>2</sup>, Matheus Carpinelli de Jesus<sup>2</sup> and Jakob Begun<sup>1</sup></p><p><sup>1</sup><i>Mater Research Institute, Australia;</i> <sup>2</sup><i>School of Chemistry and Molecular Biosciences-University of Queensland, Australia</i></p><p><b><i>Background and Aim:</i></b> Ulcerative colitis (UC) is a chronic and relapsing inflammatory disease of the colon and rectum. Despite the availability of an increasing number of therapies, achieving short-term and long-term disease control remains challenging. Urgency due to distal inflammation is one of the more disabling symptoms reported by patients. Janus kinase (Jak) pathways regulate immune signaling and are implicated in UC pathogenesis. Upadacitinib, an oral Jak-1 selective inhibitor, has demonstrated efficacy in UC, but there are concerns about its use in older patients due to safety. Upadacitinib 45 mg daily is used for induction with maintenance dosing decreasing to 30 or 15 mg. In this study, we report a case on the use of upadacitinib (10mg) daily as a suppository in a patient with severe ulcerative proctitis that had previously failed multiple advanced therapies with pharmacokinetic measurements and discuss mechanistic outcomes in pre-clinical mouse models of colitis.</p><p><b><i>Methods:</i></b> Clinical data was collected from the electronic medical record. Serial endoscopic biopsies (ranging from 10cm – 50cm) were collected to examine a gradient of inflammatory changes and quantification of upadacitinib concentration. Single cell transcriptomics were performed to assess changes in inflammatory signatures associated with upadacitinib exposure. Comparison between oral and rectal administration of upadacitinib was determined in two colitis models: a spontaneous colitis model, Winnie, and chemically induced colitis model (DSS). Histological inflammation was assessed and correlated with tissue concentrations.</p><p><b><i>Results:</i></b> There was significant improvement in endoscopic disease activity and patient-reported outcome with gradient of inflammation diminishing in severity distally. Jak/STAT related gene expression and phosphorylation of STAT-3 was negatively co-related with Upadacitinib tissue concentrations. In the pre-clinical colitis model, rectal enema significantly improved disease activity index (comprising rectal bleeding, weight loss, diarrhea) compared to oral administration of Upadacitinib. This co-related with significant reduction in histological score of inflammation in distal colon.</p><p><b>547</b></p><p><b>The UC phenotype of a rare mutation in OTUD3 is exacerbated by high fat or high fructose diets in an experimental mouse model</b></p><p><b>Rabina Giri</b><sup>1</sup>, Anna Amiss<sup>1</sup>, Sumaira Hasnain<sup>1</sup>, Timothy Florin<sup>1</sup>, Manish Gala<sup>2</sup> and Jakob Begun<sup>1</sup></p><p><sup>1</sup><i>Mater Research Institute, Australia;</i> <sup>2</sup><i>Massachusetts General Hospital-Boston, US</i></p><p><b><i>Background:</i></b> Genome-wide association studies of ulcerative colitis (UC) have uncovered multiple variants with small effect sizes, however even taken together, the contribution of these variants to the overall pathogenesis of IBD remains modest in comparison to private gene mutations. We identified a family with multiple members affected by severe UC necessitating colectomy across three generations. We identified a likely causative missense mutation in a conserved residue of the <i>OTUD3</i> gene through exome sequencing. Mutations in <i>OTUD3</i> are more common in the South Asian population (0.1%) but are not associated with severe disease, suggesting an environmental modifier involved in the severe phenotype of this Australian family. Deletion of this gene in mice globally or specifically in the intestinal compartment led to a progressive spontaneous colitis by 12 weeks of age that was exacerbated by disruption of barrier function with DSS in drinking water.</p><p><b><i>Aim:</i></b> We hypothesised that a gene – environment interaction may have exacerbated colitis in our index family and tested whether dietary factors might explain the severe phenotype in this family.</p><p><b><i>Methods and Results:</i></b> C57BL/6 mice with heterozygous or homozygous, global or intestinal epithelial cell specific, <i>OTUD3</i> disruption, were fed High Fat Diet (HFD) or high fructose diet (HFrD) for 3 weeks. Disease activity including body weight loss, diarrhoea score and rectal bleeding were monitored and histological score of inflammation and changes in mRNA expression were assessed. We found that high fat diet (HFD) and high fructose diet (HFrD accelerated the spontaneous colitis phenotype as early as 6 weeks of age in OTUD3 deficient mice. Furthermore, the diet led to impaired barrier integrity in OTUD3<sup>-/-</sup> mice as measured by FITC dextran permeability and penetration of luminal bacteria deep into the colonic crypts and liver. Consistent with these findings, pro-inflammatory chemokines and cytokines were significantly upregulated in OTUD3<sup>-/-</sup> on HFD and HFrD.</p>","PeriodicalId":15877,"journal":{"name":"Journal of Gastroenterology and Hepatology","volume":"39 S1","pages":"146-154"},"PeriodicalIF":3.7000,"publicationDate":"2024-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgh.16701","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jgh.16701","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
93
The biogeography of the mucosa-associated microbiota is associated with the presence and symptom severity of inflammatory bowel disease, proton pump inhibitor usage, and visceral sensitivity
Peter Sternes3, Ayesha Shah1,2, Camila Ayela Pintos3, Thomas Fairlie1, Natasha Koloski1, Seungha Kang2, Simon McIlroy3, Mark Morrison2, Gene Tyson3 and Gerald Holtmann1,2
1Princess Alexandria Hospital, Metro South Health, Woolloongabba, Australia;2University of Queensland, Brisbane, Australia;3Queensland University of Technology, Brisbane, Australia
Background and Aims: We aimed to assess and compare the biogeography of the mucosa associated microbiome (MAM) in patients with inflammatory bowel disease (IBD) and controls in different segments of the gastrointestinal tract, and explore the links between the MAM, gastrointestinal symptoms and use of proton pump inhibitors (PPI).
Methods: We recruited 59 controls (without structural abnormalities and gastrointestinal symptoms),44 patients with ulcerative colitis (UC) and 31 with Crohn’s disease (CD). Biopsies from various segments of the upper and lower gastrointestinal tract were collected. Microbial composition was assessed via 16S rRNA gene amplicon analysis and the bacterial load of the mucosal biopsies were assessed via qPCR. The MAM was examined in the context of disease status, PPI usage, the severity of gastrointestinal symptoms, and the symptom response to a standardized nutrient challenge (SNC).
Results: Microbial communities of the MAM in the upper and lower gastrointestinal tract are different. Compared to controls, IBD patients were characterised by relative and absolute depletion of numerous butyrate and/or propionate producing genera, with the largest differentiation being the depletion of Faecalibacterium in the lower GI tract of CD patients. PPI users had enrichment of Faecalibacteriumin the lower GI tract. The severity of gastrointestinal symptoms, as well as the symptom response to the SNC, were significantly associated with MAM composition in the GI tract.
Conclusion: The absolute and relative composition of the MAM is variable across different segments of the GI tract and is different in patients with IBD and controls. Gastrointestinal symptoms are associated with quantitative changes of bacterial taxa along the GI tract.
125
Frequency of NUDT15 polymorphisms in a multicultural Australian IBD population
Tessa Greeve1,2, Georgia Sun1 and Gregory Moore1,2
1Monash Health, Melbourne, Australia;2Monash University, Melbourne, Australia
Background and Aim: Thiopurine medications are commonly used in the management of Inflammatory Bowel Disease (IBD), however can be associated with serious adverse effects including life threatening myelosuppression. Thiopurine S-methyltransferase (TPMT) and nudix hydrolase 15 (NUDT15) are enzymes important in thiopurine metabolism. Genetic variants, resulting in reduced or absence enzyme activity, can lead to an excess of cytotoxic metabolites and are strongly associated with myelosuppression (1). Variants in NUDT15 occur more frequently in those of Asian ancestry, whilst TPMT variants are more common in those of European heritage (2). Australian guidelines recommend pre-treatment TPMT genotyping to help predict the risk of severe thiopurine-induced toxicity (3). However, though this risk exists and is even greater for those with variants in NUDT15 (2), until recently this test has not been readily available in Australia. This study aimed to determine the frequency of NUDT15 variants in the Australian IBD population.
Methods: Participants were identified from a database of patients enrolled in a thiopurine monitoring service within a tertiary hospital in Melbourne. Participants underwent concomitant NUDT15 and TPMT genotyping via a commercial pathology service. Presence of 8 NUDT15 variants was assessed. Country of birth and ethnicity, where available, was obtained from medical records.
Results: 93 individuals with IBD underwent combined NUDT15 and TPMT testing. 54 participants (58.1%) were born in Australia, of the remaining participants the majority, 28 (30.1%), were born in Asia and 6 (6.5%) in Europe. Ethnic background was not routinely recorded and was available in a minority of participants (6.45%). 10 (10.75%) participants were found to have a variant in NUDT15 whilst 3 (3.26%) participants had a variant in TPMT. The most common NUDT15 variant identified was the *3 allele, with 6 participants heterozygotes (*1/*3) (Table 1). 2 participants were heterozygotes carrying the *6 allele. The *9 allele was found in 1 individual, whilst 1 individual had a variant identified as either *1/*2 or a compound homozygote *3/*6. Of those with NUDT15 variants identified, 5/10 were born in Australia, with 1 individual born in each of Afghanistan, Bangladesh, China, India and Malaysia.
Conclusions: The prevalence of NUDT15 variants in our IBD population was significantly higher than that previously reported in an Australian IBD population (4) likely due to a predominance of European ancestry in the previously studied cohort. In this study, half of those with NUDT15 alleles were born in Australia, likely representing ancestral migration from higher risk countries. These results suggest that given the multicultural nature of the Australian population, TPMT testing alone is inadequate to identify individuals at risk of thiopurine associated harm.
References
1. Van Gennep, S, Konté, K, Meijer, B, Heymans, MW, D'Haens, GR, Löwenberg, M, et al. Systematic review with meta-analysis: risk factors for thiopurine-induced leukopenia in IBD. Aliment Pharmacol Ther.2019; 50(5): 484-506.
2. Yang, S-K, Hong, M, Baek, J, Choi, H, Zhao, W, Jung, Y, et al. A common missense variant in NUDT15 confers susceptibility to thiopurine-induced leukopenia. Nature Genetics.2014; 46(9): 1017-20.
3. Gastroenterological Society of Australia Inflammatory Bowel Disease Clinical Update 2018. 2018.
4. Afrin, S, Simms, LA, Lord, A, Radford-Smith, GL. Nudix hydrolase 15 (NUDT15) loss-of-function variants in an Australian inflammatory bowel disease population. Internal Medicine Journal2022; 52(11): 1971-7.
254
Allosteric modulation of cannabinoid 1 receptor as a novel therapeutic strategy for inflammatory bowel disease
Dinesh Thapa1, Leon Warne1, Mohan Patil1, Marco Falasca2 and Rodrigo Carlessi1
1Curtin University, Bentley, Australia;2University of Parma, Parma, Italy
Background and Aim: Novel therapies for inflammatory bowel disease (IBD) are urgently needed, as current treatments mainly provide symptomatic relief. The cannabinoid 1 receptor (CB1R), part of the endocannabinoid system, is shown to be dysregulated in IBD. While tetrahydrocannabinol (THC) has been shown to reduce IBD, mainly through orthosteric modulation of CB1R, their therapeutic applications are limited by behavioural side effects. Drugs targeting the allosteric site of CB1R have shown benefits in different diseases without behavioural side effects. This study investigated the role of the CB1R allosteric modulator ZCZ011, alone or in combination with sub-therapeutic THC, in treating IBD using a murine IBD model.
Methods: Female BALB/c mice aged 8-10 weeks were challenged with 4% dextran sodium sulphate (DSS) in drinking water for 7 days, followed by three days of normal water. THC (2.5, 5 and 10mg/kg) and/or ZCZ011 (20, 30 and 40 mg/kg) were administered intraperitoneally (i.p.), alone or in combination, daily for 11 days. Body weight, stool consistency and the presence of occult blood/rectal bleeding were scored daily to calculate the disease activity index (DAI). On day 11, mice were euthanized, and colon, spleen, kidneys, and liver were assessed for inflammation using myeloperoxidase (MPO) activity assay as well as organ weight/length measurement. Cytokines and chemokines expressions in colon lysates were assessed using multiplex assay. Toxicological parameters including complete blood count (CBC) and liver/kidney biochemistry profiles were measured.
Results: DSS-challenged mice showed increased DAI score, inflammation, and pain behaviors with decreased colon length, increased MPO activity and cytokines expression and elevated Liver and spleen weights. THC at 10mg/kg, but not 2.5 and 5 mg/kg, significantly reduced IBD as indicated by decreased DAI score, MPO activity and increased colon length. The effects of ZCZ011 alone diminished after day 8. However, a combination of 2.5mg/kg THC and 20 mg/kg ZCZ011 significantly reduced IBD as evidenced by decreased DAI score, absence of pain behaviors, increased colon length and decreased MPO activity. Body and organ weights remained comparable to healthy controls. No toxicity was observed with THC and ZCZ011, specifically the combination of 2.5 mg/kg THC and 20 mg/kg ZCZ011.
262
Antigen-specific regulatory T cell therapy for inflammatory bowel disease
Marie Lee2, Indiana Zorkau2, Joshua Ooi2, Peter Eggenhuizen2 and Rimma Goldberg1
1Department of Gastroenterology, Monash Health, Clayton, Australia;2Department of Medicine, Center for Inflammatory Diseases, Monash University, Melbourne, Australia
Background and Aim: Inflammatory bowel disease (IBD) is driven by the imbalance of inflammatory effector T cell responses and regulatory T cells (Tregs) that are unable to adequately downregulate immune-mediated pathology. Current treatments for IBD, which focus on widespread immunosuppression or blockade of specific pro-inflammatory cytokines, fail in over half of patients as this imbalance in the T cell-based immune response is not adequately addressed. Previous Treg trials in IBD using thymic-derived Tregs (tTregs) has been shown to be a safe and efficacious option to reset the aberrant immune response without drug toxicities, however, a key barrier is the difficulty in isolating a sufficient number of Tregs as these cells only comprise 5-10% of circulating CD4+ T cells. We aimed to explore a novel therapeutic approach utilising gut-homing antigen-specific induced regulatory T cells (iTregs) for the treatment of IBD in in vitro studies.
Methods: Naïve CD4+ T cells and tTregs were isolated from buffy coats of healthy donors and transduced with a gut-homing antigen-specific T cell receptor (TCR). tTregs were cultured in IL-2, rapamycin and aCD3/aCD28 Dynabeads, and naïve CD4+ T cells were differentiated into iTregs and cultured in the same additives and TGF-β for a total period of 14 days. Growth fold change from the start to end of culture was measured. Flow cytometry was used to phenotypically assess FOXP3 and TCR expression. Tregs were also assessed for IL-17 and IFN-γ production after a 5-day challenge with a pro-inflammatory cytokine cocktail (IL-2, TGF-β, IL-1β, IL-6, IL-21, IL-23) and 4-hour stimulation with phorbol 12-myristate 13-acetate, ionomycin and brefeldin A. Suppressive function of Tregs was assessed in 5-day in vitro co-cultures with antigen-specific effector T cells. P≤0.05 was considered statistically significant.
Results: Samples were collected from a total of 7 healthy donors. Median growth fold change of antigen-specific TCR-transduced iTregs cultured over a period of 14-days was found to be significantly greater compared to tTregs (96.00 [72.00, 270.00] vs 43.67 [17.62, 102.00], P=0.0175), and at the end of 14-day culture, transduced iTregs demonstrated comparable FOXP3 expression compared to tTregs (85.20 [70.70, 98.80] vs 89.90 [60.50, 99.00], P = 0.9452). In the presence of a pro-inflammatory cytokine cocktail for a duration of 5 days and additional challenge with 4-hour stimulation, iTregs showed lower IFN-γ expression (0.4800 [0.19, 0.81] vs 2.470 [0.48, 14.70], P=0.2857) and lower IL-17 than tTregs (0.08300 [0.083, 0.680] vs 3.535 [2.71, 7.67], P=0.0571). In in vitro suppression assays, antigen-specific TCR-transduced iTregs demonstrated a trend of greater suppression than non-antigen-specific iTregs.
268
Multiomic modelling of antibiotic perturbed faecal microbial communities demonstrates reduced microbial resilience in inflammatory bowel disease
Sabrina Koentgen1, Fan Zhang1, Swisha Khadka1, Xiaotao Jiang1, Thisun Jayawardana1, Emma Allen-Vercoe2, Claire O'Brien3 and Georgina Hold1
1Microbiome Research Centre, UNSW, Sydney, Australia;2University of Guelph, Guelph, Canada;3Australian National Univsersity, Canberra, Australia
Background and Aim: Ciprofloxacin (CIP) and Metronidazole (MTZ) are two antibiotics commonly used in the treatment of bacterial gastroenteritis. Both CIP and MTX are commonly used as adjuvant therapeutics for inflammatory bowel disease (IBD). However, excessive antibiotic use is also often noted as a potential risk factor in IBD, due to the impact on gastrointestinal microbiota. Disruption of gut bacteria, commonly referred to as dysbiosis, is a widely described phenomena in IBD. The role this dysbiosis plays in IBD progression and severity is still unknown. Here we investigate the impact of these commonly prescribed antibiotics on gut microbiota structure/function in a healthy donor and a new-onset therapeutic naïve IBD patient. We also investigate the use of autologous faecal microbial transplant (aFMT) as a microbial therapeutic to assist recovery of the gut ecosystem after antibiotic-induced perturbation.
Methods:In vitro modelling of gut microbial communities was achieved using continuous culture chemostat models. Donor faecal specimens (IBD or healthy control; collected as part of the Australian IBD Microbiome Study) were used to inoculate twin chemostat vessels (10% w/v) containing culture medium imitating an industrialised diet. The faecal microbial communities were allowed to stabilise for 15 days. On day 16, vessels were dosed daily with antibiotics (CIP or MTZ, for 7 days, therapeutic dosing levels). In the healthy donor vessel, 4 doses of aFMT were administered over 7 days (post antibiotics) followed by a 7-day recovery. In the IBD vessels no FMT was administered, and vessels were monitored for 7 days. Vessels were sampled daily to measure total bacterial counts, monitor microbial profiles (16S rRNA gene V3/4 profiles; Illumina MiSeq) and short chain fatty acid (SCFA) profiles (GC-MS). The Microbiome Research Centre 16S analysis pipeline and R studio were used for microbiome statistical analysis and data visualisation. Agilent MassHunter workstation was used for SCFA quantitation. Statistical analysis and visualisation were performed in R studio.
Results: When 16S rRNA gene sequence and SCFA datasets were compared, stable state microbial profiles were very different between donors, however the stable state of replicate vessels from both the healthy and IBD donors were not significantly different (p>0.05) confirming the parallelism. CIP and MTZ dosing of the healthy donor vessel impacted SCFA profiles differently. CIP caused a significant depletion of several SCFAs including acetate, butyrate, and propionate, these metabolites remained significantly depleted following aFMT. During the recovery phase levels of acetate and propionate recovered whilst butyrate remained significantly depleted (p=0.004). In the healthy MTZ vessel, acetate increased during antibiotic dosing and was restored following aFMT remaining elevated during recovery. Butyrate and valerate decreased during MTZ administration and remained significantly decreased (p<0.011). Propionate levels also reduced following MTZ but were found in highest abundance during aFMT and recovery phases (p<0.038). CIP dosing of the healthy vessel resulted in an enrichment of Escherichia-Shigella and Enterobacter with an equivalent loss of Akkermansia, Faecalibacterium and Bacteroides. Differential abundance analysis highlighted increased Parabacteroides during MTZ dosing which subsequently decreased to match steady state by recovery. Akkermansia levels significantly increased in recovery phase compared to aFMT and stability phases. In the IBD donor vessels, CIP caused a significant reduction in 10 SCFAs and of several taxon signatures including those for Bacteroides and Dialister genera alongside an enrichment of Enterococcus, Lachnospiraceae, Anaerofilum and Eisenbergiella. MTZ treatment of the IBD vessel resulted in a much less dramatic reduction in SCFAs. Microbial community changes included an enrichment of Escherichia-Shigella, Enterococcus and Parasutterella and a depletion of Alistipes and Dialister.
Conclusion: The broad-spectrum action of CIP caused significant and consistent depletion of beneficial genera and SCFAs across donors. Neither donor community was able to restore composition or function to match the stable state during the experimental period. MTZ showed more complex interactions at play with only portions of the community targeted and overall less dramatic microbial changes. Both CIP and MTX significantly depleted levels of beneficial genera including Akkermansia and Alistipes and reduced the abundance of beneficial/anti-inflammatory SCFAs. Redundancy in the microbial community potentially allowed recovery from a less aggressive perturbation with MTZ. aFMT appeared to modulate the healthy donor microbial communities to a “new healthy”. Further investigation into long-term antibiotic treatment and the use of microbial therapeutics is needed to fully understand this relationship in the context of IBD.
307
Active maternal IBD does not affect infant immune cell development
Ralley Prentice1,2,3,4, Sally Bell1,2, Steven Cho2,4, Megan Burns1, Marie Lee4, Indiana Zorkau4, Claudia Nold2,4, Emily Wright2,5, Emma Flanagan2,5, Alyson Ross3, Marcel Nold2,4 and Rimma Goldberg1,2,4
1Monash Health;2Monash University;3St Vincent's Hospital Melbourne;4Hudson Institute of Medical Research;5University of Melbourne
Background and Aim: Maintaining control of inflammatory bowel disease in pregnancy with the use of pharmacotherapies is crucial to optimising obstetric and neonatal outcomes. A detailed understanding of the effect of specific therapies and active disease on maternal immunophenotype and infant immune development is lacking. With comprehensive flow cytometric assessment, we aimed to define how IBD, it’s treatment, and disease activity impact both maternal and infant immunophenotype and cytokine production.
Methods: IBD and healthy control mother-infant dyads were recruited from Jan 2022- March 2023. IBD activity related data and peripheral blood for flow cytometry immunophenotyping and quantification of cytokine response to stimulation were obtained in each trimester of pregnancy (T1,2,3), at delivery (D) and at six weeks post-partum (PP). Active disease was defined by a fecal calprotectin >100ug/g. Cord and six-week peripheral blood samples were taken from resultant offspring.
Results: Sixteen IBD (9/16 exposed to biologic and 9/16 with CD) and two healthy control mother-infant dyads were recruited. 6/16 IBD pregnancies had active disease. Two participants required biologic dose frequency escalation in first trimester. Another underwent infliximab induction. Rates of adverse obstetric, neonatal and infant outcomes were equivalent to the Australian population with 11/16 IBD-exposed infants breastfed at six weeks old. Overall, minimal differences in adult and infant immune cell profiles and activity were observed according to active disease and medical therapy exposure, and in comparison to healthy controls. However, there were important exceptions. Basal Treg population proportions were 46% lower in those participants exposed to ustekinumab in pregnancy (0.21% vs 0.39%, Wilcoxon rank-sum P=0.027), with a trend seen with PMA/Ionomycin stimulation (0.26% vs 0.60%, p=0.0513). The proportion of CD4+ (p=0.036) and CD8+ (P=0.0495) T cells expressing unbound α4β7+ were lower in the participant exposed to vedolizumab. Basal (1.75% vs 0.47%, P=0.036) and responsiveness of cDCs and non-classical monocytes to LPS stimulation (72.2% vs 64.7%, P=0.028) were increased 3.7- and 1.1 fold respectively in those with an elevated faecal calprotectin. From T2 to T3, the proportion of IFN-γ+ CD4+ (T helper-1) (median 0.06% to 1.54%, paired t-test P=0.028) and IFN-γ+ CD8+ (0.05% to 1.54%, P=0.0012) T cells with PMA/INO stimulation increased 30-fold. The proportion of α4β7+ cDC and non-classical monocytes following LPS stimulation increased four-fold from T2 to PP (2.5% to 10.5%, P=0.047). Maternal and infant α4β7+ cDC and non-classical monocyte population proportion strongly correlated following LPS stimulation at delivery (r=0.82, p=0.0416). In infants, basal CD4+α4β7+ (41.4% to 66.5%, P=0.0043) and CD8+α4β7+ (81.2% to 93.6%, P=0.007) population proportions increased approximately 1.6- and 1.2-fold respectively from D to PP, whilst CD4+p40+ population proportions decreased 58% (0.36% to 0.15%, P=0.022) and PMA/Ionomycin stimulated CD4+ GATA3+ (T helper-2) population proportions increased 2.75 fold (0.9% to 2.47%, P=0.024). In the infant exposed to vedolizumab, unbound α4β7 expression was negligible on CD4+ and CD8+ T cells (Figure 1), with no other significant differences in immune cell population proportions noted according to in-utero pharmacotherapy exposure.
387
Comparison of drug tolerant assays for the measurement of bound anti-infliximab antibodies in patient serum
Melissa Sam1,2,3, Karla Cameron6,7, Mark Ward6,7, Therese Rexhepi1,2,3, Bonita Gu2,5, Craig Haifer2,8, Susan J Connor2,5, David Harman4, William Donald2 and Catherine Toong1,2,3,5
1NSW Health Pathology, Liverpool, Australia;2University of New South Wales, Randwick, Australia;3Ingham Institute of Applied Medical Research, Liverpool, Australia;4Western Sydney University, Campbelltown, Australia;5Liverpool Hospital, South-Western Sydney LHD, Liverpool, Australia;6Monash University, Melbourne, Australia;7Alfred Health, Melbourne, Australia;8St Vincent's Hospital, Sydney, Australia
Background and Aim: Anti-infliximab antibodies (ATI) are associated with immunogenic failure to infliximab and poor outcomes in patients with inflammatory bowel disease. Current drug sensitive ELISA tests cannot detect ATI in the presence of circulating IFX. Drug tolerant ELISAs offer the advantage of detecting total ATI, i.e. that which is bound to drug or non-neutralising ATIs. Up to 30% of patients have undetectable ATI levels on drug sensitive ELISA. The two methods tested were the anti-Lambda method (LAMBDA) and the acid-dissociation method (ACID). The LAMBDA method is based on the principle that IFX consists of only kappa light chains whereas in polyclonal human IgG, kappa and lambda light chains exist in a ratio of 2:1. ATIs bound to IFX on the plate are then detected using an anti-lambda detection antibody. The ACID method involves the breaking of IFX-ADA complexes by dropping the pH of the sample. Samples are neutralized prior to running a standard ELISA method. The aim of this study was to compare different drug tolerant methods in measuring ATI.
Methods: Patient samples from an Australian tertiary centre (Ethics 2021/ETH012703) were included if they had > 6 months steroid free clinical (Harvey Bradshaw Index ≤ 4 / Partial Mayo Score ≤ 2) and biochemical remission (C-reactive protein <5 mg/L or faecal calprotectin <150 μ/g), and had either undergone immunomodulator withdrawal and continuation of intravenous (IV) infliximab monotherapy with a therapeutic drug monitoring sample collected within the 3 months prior, or continued on combination therapy with IV infliximab and an immunomodulator. Samples were tested using two previously published drug tolerant methods – an acid dissociation (ACID) and an anti-lambda detection (LAMBDA) method. Infliximab levels were assessed between samples positive on either of the drug tolerant methods.
Results: There was no correlation between ATI positive samples on the anti-lambda detection method and the acid dissociation method (R2 of 0.007) i.e. samples that were positive on the LAMBDA method were not positive on the ACID method with one exception in our cohort. Samples in the immunomodulator withdrawal group had a 16% positivity rate in the LAMBDA method (of total number tested n= 55) compared to 8% in the ACID method group (of total number tested n = 25). In the control group positivity rates were 8% and 0% in the LAMBDA method (of total number tested n = 57) and the ACID method (of n = 20) respectively. The LAMBDA method was able to detect positive ADAs at drug levels up to 22.8 mg/L compared to the ACID method at 3 mg/L. Mean drug level that reached positivity in the LAMBDA and the ACID methods were 5.7 mg/L ± 1.3 SEM vs 2.1mg/L ± 0.8 SEM respectively, however this was not significant due to the small sample size.
Conclusion: Current assays offer no consensus on positivity for bound ATIs. The higher positivity rate in the LAMBDA method may be due to non-neutralising antibodies, the clinical significance of which is unclear. The ACID method involves the breaking of IFX-ADA complexes and detects neutralizing antibodies and so may provide more clinically relevant information. This method, however, is more sensitive to circulating IFX levels and is affected by the reassociation of complexes that form when neutralizing the sample prior to the ELISA method. Essentially, current methods are variable and produce discordant results. Further studies are required to investigate these assays and to develop further tests to provide more information on the development of ATIs and their clinical relevance. Our group is currently working on mass spectrometry methods to further clarify the development of ADAs and their effect on circulating drug levels.
453
Age-dependent dysregulation of the UPR in colonic epithelium: Implications for mucosal integrity
Thishan Illankoon1,2, Kuan Yau Wong1,2, Haressh Sajiir1,2, Alexandra Mueller1,2, Anna Amiss1,2, Jakob Begun1,2, Rabina Giri1,2, Lucy Burr1,2 and Sumaira Hasnain1,2
1Mater Research Institute (Translational Research Institute), Brisbane, Australia;2University of Queensland, Brisbane, Australia
Background and Aim: Misfolded protein accumulation in the endoplasmic reticulum (ER) due to various endogenous and exogenous factors triggers ER stress, a hallmark of numerous diseases, including inflammatory bowel disease (IBD). Eukaryotic cells combat this stress via the unfolded protein response (UPR), a regulatory network that promotes correct protein folding and maintains cellular homeostasis. Age-related increases in protein aggregates, even in healthy individuals, suggest a decline in UPR function as a natural consequence of aging. Research has explored the UPR’s role in neurodegenerative diseases. However, the impact of an aging UPR on mucosal epithelial cells in the intestine remains largely unexplored. We hypothesise that the age-related UPR senescence contributes to the heightened susceptibility to infections and increased disease severity observed in aged individuals. In this study, we comprehensively characterized age-related changes in the UPR of intestinal epithelial cells from both healthy mice/humans and those with intestinal inflammation.
Methods: To investigate our aims, both human samples and mouse models have been utilised. Human colon biopsies were accessed via the Mater Research IBD biobank which included a wide range of patient samples, both with and without IBD. They were sorted into three age groups (young = <25; middle aged = 30-50; aged = >65). For the mouse models, C57BL/6 (control) and Winnie (model of spontaneous colitis via a mutation in the Muc2 gene) mice, intestinal epithelial cells were isolated from 4-, 8-, 12-, 24-, 44-, and 60-weeks old animals. qRT-PCR was utilized to assess the changes in the UPR-related genes, and histological analyses of intestinal proteins was conducted using immunohistochemistry and immunofluorescence.
Results: qPCR analysis of colonic epithelial cells in aging C57BL/6 mice, revealed a significant upregulation of various UPR markers until around 44-weeks of age. This upregulation was followed by a decrease in specific markers at 60-weeks. Compared to age-matched controls, Winnie mice exhibited a significant reduction in the expression of downstream UPR markers, particularly in older age group. Mucin production in the C57BL/6 mice declined throughout aging, with a more pronounced decreased observed in Winnie mice. Analysis of human colon biopsies revealed an age-related increase in protein folding chaperones, suggesting heightened ER stress. Interestingly, there was a trend of decline in downstream UPR markers, potentially indicating a compromised UPR in older individuals.
Conclusion: Our findings support the hypothesis that the UPR becomes less effective with age in colonic epithelial cells. This conclusion is based on the observed increase in ER stress markers alongside a decrease in downstream UPR activity and mucin production. These age-related changes may contribute to the increased susceptibility to infections and disease severity reported in older individuals. Further investigation is ongoing to elucidate the mechanisms behind this decline, with a particular emphasis on infection management, metabolic alterations, and epigenetic factors. This comprehensive approach will enhance understanding of the complex interplay between UPR dysfunction and aging in the colonic mucosa.
489
Deep functional analysis of a defined sulphide-reducing diet (4-SURE diet) as a novel therapy for ulcerative colitis demonstrates all specific luminal micro environmental objectives were achieved
Alice Day1,2,3, Rachael Slater4, Vanessa Marcelino5,6, Reuben Wheeler7, Remy Young5,8, Natasha Maddigan2,3, Samuel Forster5,8, Samuel Costello1,2,3, Wendy Uylaki1,3, Chris Probert4, Jane Andrews2,9, Chu K Yao10, Peter Gibson10 and Robert Bryant1,2,3
1Inflammatory Bowel Disease Services, Department of Gastroenterology and Hepatology, The Queen Elizabeth Hospital, Adelaide, Australia;2School of Medicine, Faculty of Health Sciences, University of Adelaide, Adelaide, Australia;3Basil Hetzel Research Institute, Adelaide, Australia;4Institute of Systems, Molecular and Integrative Biology, Department of Molecular and Clinical Cancer, University of Liverpool, Liverpool, United Kingdom;5Centre for Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Clayton, Australia;6Melbourne Integrative Genomics, School of BioSciences & Department of Microbiology and Immunology at The Peter Doherty Institute, The University of Melbourne, Melbourne, Australia;7College of Science and Engineering, Flinders University, Adelaide, Australia;8Department of Molecular and Translational Sciences, Monash University, Clayton, Australia;9Inflammatory Bowel Disease Service, Department of Gastroenterology and Hepatology, Royal Adelaide Hospital, Adelaide, Australia;10Department of Gastroenterology, School of Translational Research, Monash University & Alfred Health, Melbourne, Australia
Background and Aim: As a dietary approach to reducing inflammation in ulcerative colitis (UC), the 4-SURE diet was designed to correct pathogenic alterations of excessive protein fermentation and hydrogen sulphide (H2S) production in the distal colon. The specific dietary objectives were achieved (Day et al, J Nutr 2022;152:1690) but it is uncertain whether these mechanistic objectives could be achieved with 8 weeks of diet. Therefore, we aimed to perform a deep functional analysis (microbial and metabolomic) of the faeces.
Methods: Faecal samples of 28 adults with mild-moderately active UC were collected at week 0 and 8 of dietary intervention, processed and aliquoted. Shotgun metagenomic sequencing was used to identify genes involved in H2S metabolism. Metagenomic reads were trimmed and reads mapping to the human genome removed. Gene identification was performed using Diamond v2.1.9 for alignment against a database of genes involved in global sulphur cycling. Gas-chromatography mass-spectrometry was used to characterise volatile organic compounds (VOCs) with specific analysis of products of protein fermentation. Capacity of the microbiota to produce H2S was determined by incubating homogenates anaerobically for 24hours, then total H2S production was measured spectrophotometrically.
Results: Majority of microbiome members at week 0 and 8 belonged to the Bacteroidota and Bacillota phyla. There were no differences in bacterial diversity (p=0.16). However, by Random Forest Plot Classifier, known H2S producers, Odoribacter and Peptostreptococcaceae, were taxa of highest importance in discriminating between beforediet and after-diet samples, where abundance was markedly lower. The capacity for H2S metabolism altered, with significant differences (p<0.05, Wilcoxon signed-rank with BenjaminiHochberg correction) in 6 of 23 analysed sulphur-metabolising genes involved in H2S cycling, including iscS, cysK (Fig. 1), metC, luxS, asrC and sseA. Composition of 173 identified faecal VOCs differed before and after diet; indole (a specific marker of protein fermentation) decreased from 0.42 [-0.25,0.61] at week 0 to -0.28 [-0.77,0.48] at week 8 (p=0.007, FDR correction; Fig. 1). Faecal H2S reduced from median 2.61 (interquartile range 2–4.96)μmol to 1.41 (0.81-2.27)μmol of H2S/g stool (wet weight) (p=0.002) (Fig. 1).
504
RNA sequencing of mucosal biopsies: an unbiased approach in the assessment of host molecular inflammatory state in the investigation of host-microbiota interactions in ulcerative colitis
Patricia Khoo1,2,3, Linden Gearing1,3, Jodee Gould1,3, Emily Rutten1,3, Samuel Forster1,3 and Edward Giles1,2,3
1Centre for Innate Immunity and Infectious Diseases, Hudson Institute of Medical Research, Clayton, Australia;2Department of Paediatrics, Monash University, Clayton, Australia;3Department of Molecular and Translational Sciences, Monash University, Clayton, Australia
Background and Aim: Inflammatory bowel disease (IBD) is caused by an aberrant immune response in genetically susceptible individuals to the environment, including their microbiota. In recent years an explosion in microbiome research in IBD has yet to change diagnostic algorithms nor resulted in new treatments. The majority of studies have focused on stool samples, hence lacking the representation of mucosa-associated microbiota and the characterisation of host-microbiota interaction at the mucosal interface. To address these challenges, we propose an approach of paired measurement of site-specific host transcriptional response along with its mucosa-associated microbiota.
Methods: Fresh rectal biopsies were obtained from adults with ulcerative colitis and controls at a tertiary gastroenterology endoscopy service. Four mucosal samples were obtained from each patient, at the site of inflammation if inflammation was observed. Two biopsies were sent for anatomical pathology review. Matched mucosal culturing of mucosa-associated bacteria (Figure 1a) and RNA sequencing of host transcriptional profiling were performed. RNA sequencing analysis was performed in R (v4.3.2). The Hallmark Inflammatory Response gene set from the Hallmark gene set collection was used to classify samples as molecularly inflamed or non-inflamed. Log2 expression of the 164 detected inflammatory response genes were clustered using k-means, with k=2.
Results: Samples were collected from a total of 98 patients: 52 with ulcerative colitis (UC) and 46 controls (CO). The mean age of UC patients was 36.3 years (21-75), and 42.3% were female. The mean age of CO patients was 36.4 years (18-56), and 54.3% were female. A multidimensional scaling (MDS) plot was constructed based on the top 500 most variable genes from the filtered and normalised data, coloured by variables. Principal coordinate analysis (PCA) plot was then generated using the Hallmark Inflammatory Response gene set. It demonstrated a cluster of molecularly inflamed (IR) samples, which comprised mostly of the histologically inflamed UC samples but there are some histologically inflamed samples that did not belong to the molecularly inflamed cluster. The first principal component of the PCA plot correlated very well with the first dimension of the MDS plot (Figure 1b), indicating that these inflammatory genes are a major source of variation across the data.
545
Topical upadacitinib is effective in distal ulcerative colitis: A case study and pre-clinical proof of concept
Rabina Giri1, Anna Amiss1, Bruce Riches2, Matheus Carpinelli de Jesus2 and Jakob Begun1
1Mater Research Institute, Australia;2School of Chemistry and Molecular Biosciences-University of Queensland, Australia
Background and Aim: Ulcerative colitis (UC) is a chronic and relapsing inflammatory disease of the colon and rectum. Despite the availability of an increasing number of therapies, achieving short-term and long-term disease control remains challenging. Urgency due to distal inflammation is one of the more disabling symptoms reported by patients. Janus kinase (Jak) pathways regulate immune signaling and are implicated in UC pathogenesis. Upadacitinib, an oral Jak-1 selective inhibitor, has demonstrated efficacy in UC, but there are concerns about its use in older patients due to safety. Upadacitinib 45 mg daily is used for induction with maintenance dosing decreasing to 30 or 15 mg. In this study, we report a case on the use of upadacitinib (10mg) daily as a suppository in a patient with severe ulcerative proctitis that had previously failed multiple advanced therapies with pharmacokinetic measurements and discuss mechanistic outcomes in pre-clinical mouse models of colitis.
Methods: Clinical data was collected from the electronic medical record. Serial endoscopic biopsies (ranging from 10cm – 50cm) were collected to examine a gradient of inflammatory changes and quantification of upadacitinib concentration. Single cell transcriptomics were performed to assess changes in inflammatory signatures associated with upadacitinib exposure. Comparison between oral and rectal administration of upadacitinib was determined in two colitis models: a spontaneous colitis model, Winnie, and chemically induced colitis model (DSS). Histological inflammation was assessed and correlated with tissue concentrations.
Results: There was significant improvement in endoscopic disease activity and patient-reported outcome with gradient of inflammation diminishing in severity distally. Jak/STAT related gene expression and phosphorylation of STAT-3 was negatively co-related with Upadacitinib tissue concentrations. In the pre-clinical colitis model, rectal enema significantly improved disease activity index (comprising rectal bleeding, weight loss, diarrhea) compared to oral administration of Upadacitinib. This co-related with significant reduction in histological score of inflammation in distal colon.
547
The UC phenotype of a rare mutation in OTUD3 is exacerbated by high fat or high fructose diets in an experimental mouse model
Rabina Giri1, Anna Amiss1, Sumaira Hasnain1, Timothy Florin1, Manish Gala2 and Jakob Begun1
1Mater Research Institute, Australia;2Massachusetts General Hospital-Boston, US
Background: Genome-wide association studies of ulcerative colitis (UC) have uncovered multiple variants with small effect sizes, however even taken together, the contribution of these variants to the overall pathogenesis of IBD remains modest in comparison to private gene mutations. We identified a family with multiple members affected by severe UC necessitating colectomy across three generations. We identified a likely causative missense mutation in a conserved residue of the OTUD3 gene through exome sequencing. Mutations in OTUD3 are more common in the South Asian population (0.1%) but are not associated with severe disease, suggesting an environmental modifier involved in the severe phenotype of this Australian family. Deletion of this gene in mice globally or specifically in the intestinal compartment led to a progressive spontaneous colitis by 12 weeks of age that was exacerbated by disruption of barrier function with DSS in drinking water.
Aim: We hypothesised that a gene – environment interaction may have exacerbated colitis in our index family and tested whether dietary factors might explain the severe phenotype in this family.
Methods and Results: C57BL/6 mice with heterozygous or homozygous, global or intestinal epithelial cell specific, OTUD3 disruption, were fed High Fat Diet (HFD) or high fructose diet (HFrD) for 3 weeks. Disease activity including body weight loss, diarrhoea score and rectal bleeding were monitored and histological score of inflammation and changes in mRNA expression were assessed. We found that high fat diet (HFD) and high fructose diet (HFrD accelerated the spontaneous colitis phenotype as early as 6 weeks of age in OTUD3 deficient mice. Furthermore, the diet led to impaired barrier integrity in OTUD3-/- mice as measured by FITC dextran permeability and penetration of luminal bacteria deep into the colonic crypts and liver. Consistent with these findings, pro-inflammatory chemokines and cytokines were significantly upregulated in OTUD3-/- on HFD and HFrD.
期刊介绍:
Journal of Gastroenterology and Hepatology is produced 12 times per year and publishes peer-reviewed original papers, reviews and editorials concerned with clinical practice and research in the fields of hepatology, gastroenterology and endoscopy. Papers cover the medical, radiological, pathological, biochemical, physiological and historical aspects of the subject areas. All submitted papers are reviewed by at least two referees expert in the field of the submitted paper.
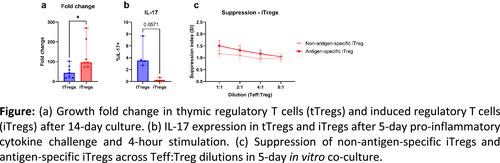
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


