Stepped-Wedge Trial of Decision Support for Acute Kidney Injury on Surgical Units
IF 8.3
2区 材料科学
Q1 MATERIALS SCIENCE, MULTIDISCIPLINARY
引用次数: 0
Abstract
Introduction
Acute kidney injury (AKI) is common in the perioperative setting and associated with poor outcomes. Whether clinical decision support improves early management and outcomes of AKI on surgical units is uncertain.
Methods
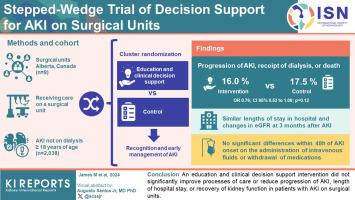
In this cluster-randomized, stepped-wedge trial, 8 surgical units in Alberta, Canada were randomized to various start dates to receive an education and clinical decision support intervention for recognition and early management of AKI. Eligible patients were aged ≥18 years, receiving care on a surgical unit, not already receiving dialysis, and with AKI.
Results
There were 2135 admissions of 2038 patients who met the inclusion criteria; mean (SD) age was 64.3 (16.2) years, and 885 (41.4%) were females. The proportion of patients who experienced the composite primary outcome of progression of AKI to a higher stage, receipt of dialysis, or death was 16.0% (178 events/1113 admissions) in the intervention group; and 17.5% (179 events/1022 admissions) in the control group (time-adjusted odds ratio, 0.76; 95% confidence interval [CI], 0.53–1.08; P = 0.12). There were no significant differences between groups in process of care outcomes within 48 hours of AKI onset, including administration of i.v. fluids, or withdrawal of medications affecting kidney function. Both groups experienced similar lengths of stay in hospital after AKI and change in estimated glomerular filtration rate (eGFR) at 3 months.
Conclusion
An education and clinical decision support intervention did not significantly improve processes of care or reduce progression of AKI, length of hospital stays, or recovery of kidney function in patients with AKI on surgical units.
手术室急性肾损伤决策支持的阶梯式楔形试验
急性肾损伤(AKI)是围手术期的常见病,与不良预后有关。临床决策支持是否能改善手术单位对 AKI 的早期管理和治疗效果尚不确定。在这项分组随机、阶梯式试验中,加拿大阿尔伯塔省的 8 家手术单位被随机分配到不同的起始日期,接受教育和临床决策支持干预,以识别和早期管理 AKI。符合条件的患者年龄≥18 岁,在手术室接受治疗,尚未接受透析,并患有 AKI。符合纳入标准的 2038 名患者中有 2135 人入院;平均(标清)年龄为 64.3(16.2)岁,885 人(41.4%)为女性。出现 AKI 进展到更高阶段、接受透析或死亡这一复合主要结局的患者比例在干预组为 16.0%(178 例/1113 例入院);在对照组为 17.5%(179 例/1022 例入院)(时间调整后的几率比为 0.76;95% 置信区间 [CI],0.53-1.08;= 0.12)。两组在 AKI 发病 48 小时内的护理结果(包括静脉输液或停用影响肾功能的药物)无明显差异。两组患者在发生 AKI 后的住院时间和 3 个月时估计肾小球滤过率(eGFR)的变化相似。教育和临床决策支持干预并未明显改善护理流程,也未减少手术室AKI患者的AKI进展、住院时间或肾功能恢复情况。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

ACS Applied Materials & Interfaces
工程技术-材料科学:综合
CiteScore
16.00
自引率
6.30%
发文量
4978
审稿时长
1.8 months
期刊介绍:
ACS Applied Materials & Interfaces is a leading interdisciplinary journal that brings together chemists, engineers, physicists, and biologists to explore the development and utilization of newly-discovered materials and interfacial processes for specific applications. Our journal has experienced remarkable growth since its establishment in 2009, both in terms of the number of articles published and the impact of the research showcased. We are proud to foster a truly global community, with the majority of published articles originating from outside the United States, reflecting the rapid growth of applied research worldwide.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


