Peter Lin, Nilay T Argon, Qian Cheng, Christopher S Evans, Benjamin Linthicum, Yufeng Liu, Abhishek Mehrotra, Laura Murphy, Mehul D Patel, Serhan Ziya
{"title":"Identifying Patient Subpopulations with Significant Race-Sex Differences in Emergency Department Disposition Decisions.","authors":"Peter Lin, Nilay T Argon, Qian Cheng, Christopher S Evans, Benjamin Linthicum, Yufeng Liu, Abhishek Mehrotra, Laura Murphy, Mehul D Patel, Serhan Ziya","doi":"10.1177/11786329241277724","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>The race-sex differences in emergency department (ED) disposition decisions have been reported widely. Our objective is to identify demographic and clinical subgroups for which this difference is most pronounced, which will facilitate future targeted research on potential disparities and interventions.</p><p><strong>Methods: </strong>We performed a retrospective analysis of 93 987 White and African-American adults assigned an Emergency Severity Index of 3 at 3 large EDs from January 2019 to February 2020. Using random forests, we identified the Elixhauser comorbidity score, age, and insurance status as important variables to divide data into subpopulations. Logistic regression models were then fitted to test race-sex differences within each subpopulation while controlling for other patient characteristics and ED conditions.</p><p><strong>Results: </strong>In each subpopulation, African-American women were less likely to be admitted than White men with odds ratios as low as 0.304 (95% confidence interval (CI): [0.229, 0.404]). African-American men had smaller admission odds compared to White men in subpopulations of 41+ years of age or with very low/high Elixhauser scores, odds ratios being as low as 0.652 (CI: [0.590, 0.747]). White women were less likely to be admitted than White men in subpopulations of 18 to 40 or 41 to 64 years of age, with low Elixhauser scores, or with Self-Pay or Medicaid insurance status with odds ratios as low as 0.574 (CI: [0.421, 0.784]).</p><p><strong>Conclusions: </strong>While differences in likelihood of admission were lessened by younger age for African-American men, and by older age, higher Elixhauser score, and Medicare or Commercial insurance for White women, they persisted in all subgroups for African-American women. In general, patients of age 64 years or younger, with low comorbidity scores, or with Medicaid or no insurance appeared most prone to potential disparities in admissions.</p>","PeriodicalId":12876,"journal":{"name":"Health Services Insights","volume":"17 ","pages":"11786329241277724"},"PeriodicalIF":2.5000,"publicationDate":"2024-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378179/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11786329241277724","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objectives: The race-sex differences in emergency department (ED) disposition decisions have been reported widely. Our objective is to identify demographic and clinical subgroups for which this difference is most pronounced, which will facilitate future targeted research on potential disparities and interventions.
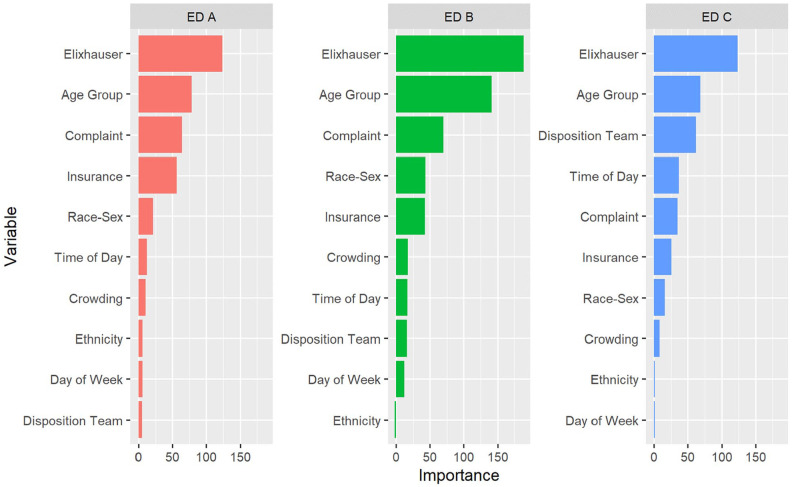
Methods: We performed a retrospective analysis of 93 987 White and African-American adults assigned an Emergency Severity Index of 3 at 3 large EDs from January 2019 to February 2020. Using random forests, we identified the Elixhauser comorbidity score, age, and insurance status as important variables to divide data into subpopulations. Logistic regression models were then fitted to test race-sex differences within each subpopulation while controlling for other patient characteristics and ED conditions.
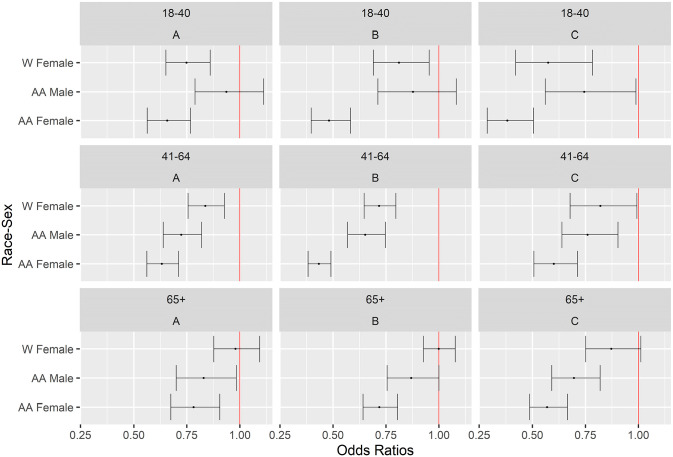
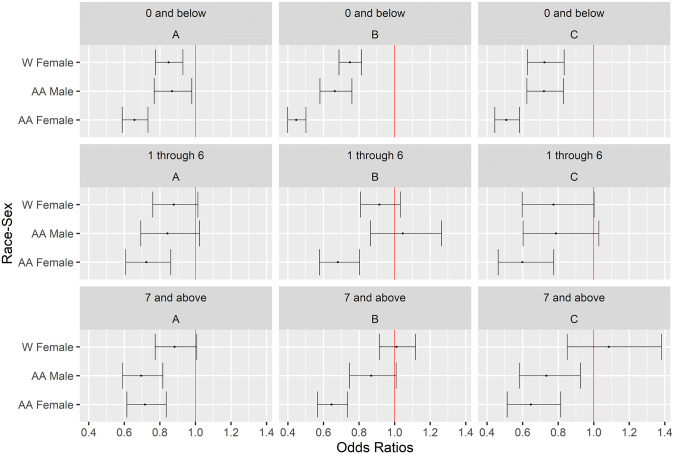
Results: In each subpopulation, African-American women were less likely to be admitted than White men with odds ratios as low as 0.304 (95% confidence interval (CI): [0.229, 0.404]). African-American men had smaller admission odds compared to White men in subpopulations of 41+ years of age or with very low/high Elixhauser scores, odds ratios being as low as 0.652 (CI: [0.590, 0.747]). White women were less likely to be admitted than White men in subpopulations of 18 to 40 or 41 to 64 years of age, with low Elixhauser scores, or with Self-Pay or Medicaid insurance status with odds ratios as low as 0.574 (CI: [0.421, 0.784]).
Conclusions: While differences in likelihood of admission were lessened by younger age for African-American men, and by older age, higher Elixhauser score, and Medicare or Commercial insurance for White women, they persisted in all subgroups for African-American women. In general, patients of age 64 years or younger, with low comorbidity scores, or with Medicaid or no insurance appeared most prone to potential disparities in admissions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


