Hadjer Dahel, Najla Tabbara, Lisa Burry, Gabrielle Hornstein, David Williamson, Han Ting Wang
{"title":"Optimizing Subsequent CARdiovascular Medication Reintroduction in the Intensive Care Unit.","authors":"Hadjer Dahel, Najla Tabbara, Lisa Burry, Gabrielle Hornstein, David Williamson, Han Ting Wang","doi":"10.1177/20543581241276361","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Hospital admission for a critical illness episode creates communication breakpoints and can lead to medication discrepancies during hospital stays. Due to the patient's underlying condition and the care setting, chronic medications such as cardiovascular medication are often held, discontinued, or changed to alternative administration routes. Unfortunately, data on the optimal timing of cardiovascular drug reinitiation among intensive care unit (ICU) survivors are lacking.</p><p><strong>Objective: </strong>The primary objective of this study was to describe the prevalence of chronic cardiovascular medication taken before hospital admission and discontinued at ICU discharge and hospital discharge for critically ill patients. A secondary objective was to assess factors associated with medication discontinuation.</p><p><strong>Design setting and participants: </strong>We conducted a multicentered retrospective cohort study at 2 tertiary academic hospitals in Canada. All adult patients taking cardiovascular medication before ICU admission and surviving to hospital discharge between April 1, 2016, and April 1, 2017, were eligible.</p><p><strong>Main outcomes and measures: </strong>The main outcome of the study was the discontinuation of cardiovascular medication prescribed before ICU admission. The outcome was assessed through participants' chart review.</p><p><strong>Results: </strong>We included 352 patients with a median age of 71.0 years. A total of 155 patients (44.03%) had at least 1 cardiovascular medication discontinued during their stay. Our adjusted model uncovered 3 factors associated with cardiovascular medication discontinuation: male sex (odds ratio [OR] = 0.564, 95% confidence interval [CI] = 0.346-0.919), number of cardiovascular medications taken preadmission (OR = 1.669, 95% CI = 1.003-2.777 for 2 medications and OR = 3.170, 95% CI = 1.325-7.583), and the use of vasopressors (OR = 1.770, 95% CI = 1.045-2.997).</p><p><strong>Conclusion: </strong>Our study uncovered that cardiovascular medication discontinuation for ICU patients is frequent, especially for renin-angiotensin system (RAS) blockers. Data from our study could be used to reinforce site-specific protocols of medication reconciliation and optimization, as well as inform future protocols aimed at RAS blocker reinitiation follow-up.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241276361"},"PeriodicalIF":1.5000,"publicationDate":"2024-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378200/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241276361","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Hospital admission for a critical illness episode creates communication breakpoints and can lead to medication discrepancies during hospital stays. Due to the patient's underlying condition and the care setting, chronic medications such as cardiovascular medication are often held, discontinued, or changed to alternative administration routes. Unfortunately, data on the optimal timing of cardiovascular drug reinitiation among intensive care unit (ICU) survivors are lacking.
Objective: The primary objective of this study was to describe the prevalence of chronic cardiovascular medication taken before hospital admission and discontinued at ICU discharge and hospital discharge for critically ill patients. A secondary objective was to assess factors associated with medication discontinuation.
Design setting and participants: We conducted a multicentered retrospective cohort study at 2 tertiary academic hospitals in Canada. All adult patients taking cardiovascular medication before ICU admission and surviving to hospital discharge between April 1, 2016, and April 1, 2017, were eligible.
Main outcomes and measures: The main outcome of the study was the discontinuation of cardiovascular medication prescribed before ICU admission. The outcome was assessed through participants' chart review.
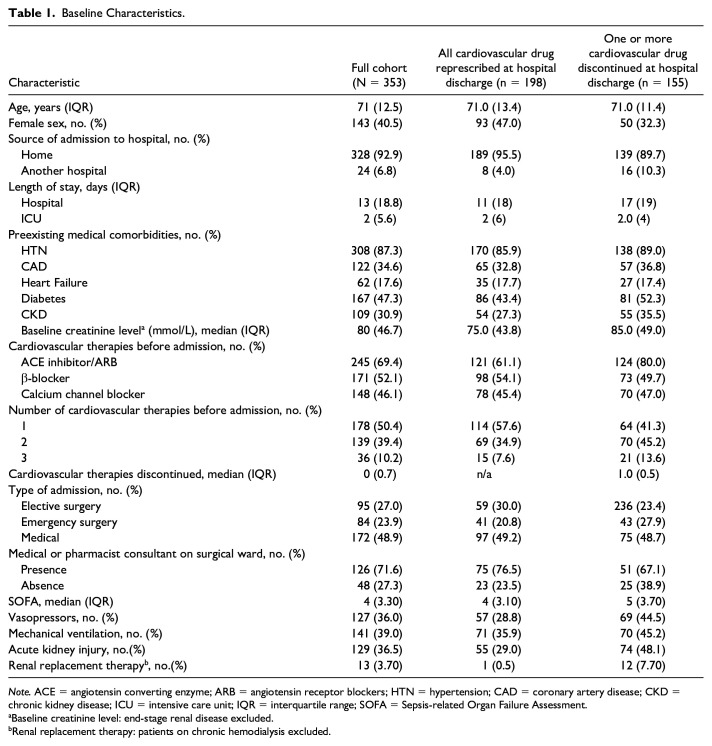
Results: We included 352 patients with a median age of 71.0 years. A total of 155 patients (44.03%) had at least 1 cardiovascular medication discontinued during their stay. Our adjusted model uncovered 3 factors associated with cardiovascular medication discontinuation: male sex (odds ratio [OR] = 0.564, 95% confidence interval [CI] = 0.346-0.919), number of cardiovascular medications taken preadmission (OR = 1.669, 95% CI = 1.003-2.777 for 2 medications and OR = 3.170, 95% CI = 1.325-7.583), and the use of vasopressors (OR = 1.770, 95% CI = 1.045-2.997).
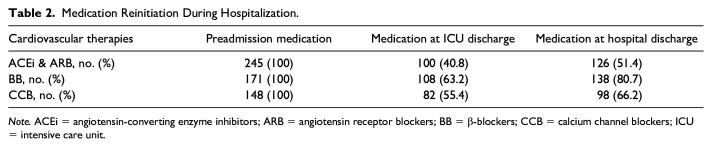
Conclusion: Our study uncovered that cardiovascular medication discontinuation for ICU patients is frequent, especially for renin-angiotensin system (RAS) blockers. Data from our study could be used to reinforce site-specific protocols of medication reconciliation and optimization, as well as inform future protocols aimed at RAS blocker reinitiation follow-up.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


