Comparative efficacy of endoscopic ultrasound-guided biliary drainage versus endoscopic retrograde cholangiopancreatography as first-line palliation in malignant distal biliary obstruction: a systematic review and meta-analysis.
Shravya Reddy Ginnaram, Sudeep Nugooru, Dawood Tahir, Kara Devine, Ali Raza Shaikh, Pradeep Yarra, James Walter
{"title":"Comparative efficacy of endoscopic ultrasound-guided biliary drainage versus endoscopic retrograde cholangiopancreatography as first-line palliation in malignant distal biliary obstruction: a systematic review and meta-analysis.","authors":"Shravya Reddy Ginnaram, Sudeep Nugooru, Dawood Tahir, Kara Devine, Ali Raza Shaikh, Pradeep Yarra, James Walter","doi":"10.20524/aog.2024.0912","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malignant distal biliary obstruction (MDBO) is a challenging clinical condition commonly managed with endoscopic retrograde cholangiopancreatography (ERCP). However, endoscopic ultrasound-guided biliary drainage (EUS-BD) has emerged as an alternative, especially in complex cases where ERCP fails or is deemed risky. This study aimed to compare the efficacy, safety and cost-effectiveness of EUS-BD vs. ERCP in the palliation of MDBO.</p><p><strong>Methods: </strong>We conducted a systematic review and meta-analysis, following PRISMA guidelines. Three databases were searched up to December 2023, including MEDLINE/PubMed, OVID and the Cochrane Central Register of Controlled Trials, for studies comparing EUS-BD with ERCP. Primary outcomes were technical and clinical success rates, while secondary outcomes included procedural times, hospital stay duration, 30-day mortality, reintervention rates, and adverse events such as pancreatitis.</p><p><strong>Results: </strong>Seven studies involving 1245 patients met the inclusion criteria. The meta-analysis revealed that EUS-BD had a technical success rate of 92%, compared to 85% for ERCP. Clinical success rates were similar for both EUS-BD and ERCP, at approximately 89%. EUS-BD was associated with a significantly lower incidence of pancreatitis (2% vs. 10% for ERCP).</p><p><strong>Conclusions: </strong>EUS-BD offers a viable and potentially superior alternative to ERCP for the primary palliation of MDBO, particularly in terms of technical success and a lower risk of pancreatitis. These findings support the adoption of EUS-BD in clinical settings equipped to perform this technique, though future research should focus on long-term outcomes and further economic analysis to solidify these recommendations.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 5","pages":"602-609"},"PeriodicalIF":2.2000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11372544/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0912","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/19 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Malignant distal biliary obstruction (MDBO) is a challenging clinical condition commonly managed with endoscopic retrograde cholangiopancreatography (ERCP). However, endoscopic ultrasound-guided biliary drainage (EUS-BD) has emerged as an alternative, especially in complex cases where ERCP fails or is deemed risky. This study aimed to compare the efficacy, safety and cost-effectiveness of EUS-BD vs. ERCP in the palliation of MDBO.
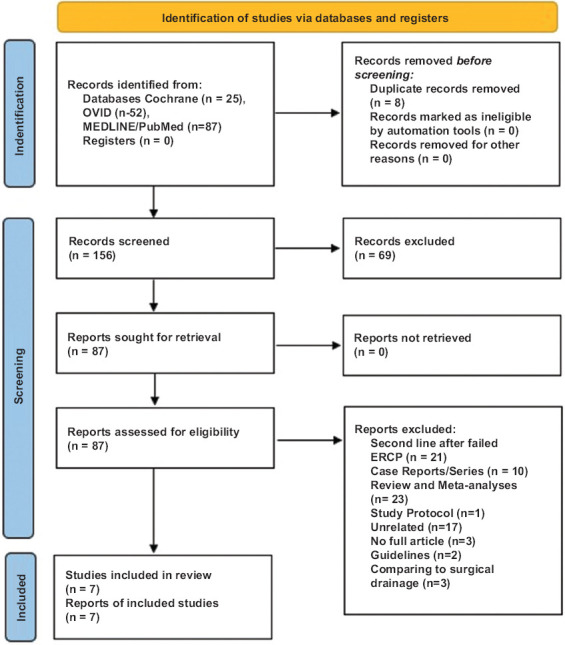
Methods: We conducted a systematic review and meta-analysis, following PRISMA guidelines. Three databases were searched up to December 2023, including MEDLINE/PubMed, OVID and the Cochrane Central Register of Controlled Trials, for studies comparing EUS-BD with ERCP. Primary outcomes were technical and clinical success rates, while secondary outcomes included procedural times, hospital stay duration, 30-day mortality, reintervention rates, and adverse events such as pancreatitis.
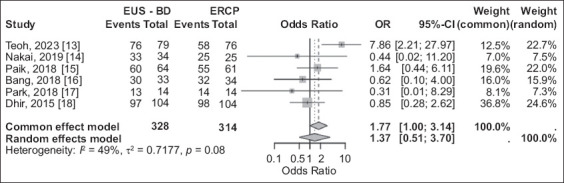
Results: Seven studies involving 1245 patients met the inclusion criteria. The meta-analysis revealed that EUS-BD had a technical success rate of 92%, compared to 85% for ERCP. Clinical success rates were similar for both EUS-BD and ERCP, at approximately 89%. EUS-BD was associated with a significantly lower incidence of pancreatitis (2% vs. 10% for ERCP).
Conclusions: EUS-BD offers a viable and potentially superior alternative to ERCP for the primary palliation of MDBO, particularly in terms of technical success and a lower risk of pancreatitis. These findings support the adoption of EUS-BD in clinical settings equipped to perform this technique, though future research should focus on long-term outcomes and further economic analysis to solidify these recommendations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


