{"title":"The predictive role of autonomic neuropathy in pre- and post-liver transplantation outcomes: a systematic review and meta-analysis.","authors":"Antonia Neonaki, Vasileios Lekakis, Evangelos Cholongitas","doi":"10.20524/aog.2024.0905","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Autonomic neuropathy (AN) in cirrhotic patients has been linked to a higher risk of cirrhosis-related complications and worse outcomes before, during or after liver transplantation (LT). However, only a few studies exist with inconsistent results.</p><p><strong>Methods: </strong>We searched for all articles published until September 2023 that described a diagnosis of AN based on cardiovascular autonomic reflex tests (CARTs), assessment of the rate-corrected QT interval (QTc), heart rate variability (HRV), and baroreflex sensitivity (BRS) tests, in order to evaluate the predictive role of AN in cirrhosis and/or peri-/post-LT prognosis.</p><p><strong>Results: </strong>Twenty-five studies were included: 5, 12, 9, and 1 study, respectively, assessed the predictive role of CARTs, prolonged QTc, HRV indices, and BRS in cirrhosis or peri-/post-LT prognosis. In CARTs-based analysis, the pre-LT pooled mortality rate was significantly higher in cirrhotics with AN compared to those without AN (20% vs. 6%; P=0.01). However, no difference was found between patients with and without pre-LT prolonged QTc in the pre-LT pooled mortality rates (41% vs. 18%; P=0.08), pooled peri-transplant risk of major complications (29% vs. 17%; P=0.08) or post-LT pooled mortality rates (15% vs. 12%; P=0.36). In HRV-based analysis, the standard deviation of normal-to-normal intervals was significantly lower in non-survivors, compared to survivors with cirrhosis: standardized mean difference -2.59, 95% confidence interval -4.75 to -0.43; P=0.04.</p><p><strong>Conclusions: </strong>The presence of CARTs- and HRV-based AN was a good predictor of mortality in the pre-LT setting. Preoperative prolonged QTc did not seem to be associated with the outcome before or after LT.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"37 5","pages":"588-601"},"PeriodicalIF":2.2000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11372533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2024.0905","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/12 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Autonomic neuropathy (AN) in cirrhotic patients has been linked to a higher risk of cirrhosis-related complications and worse outcomes before, during or after liver transplantation (LT). However, only a few studies exist with inconsistent results.
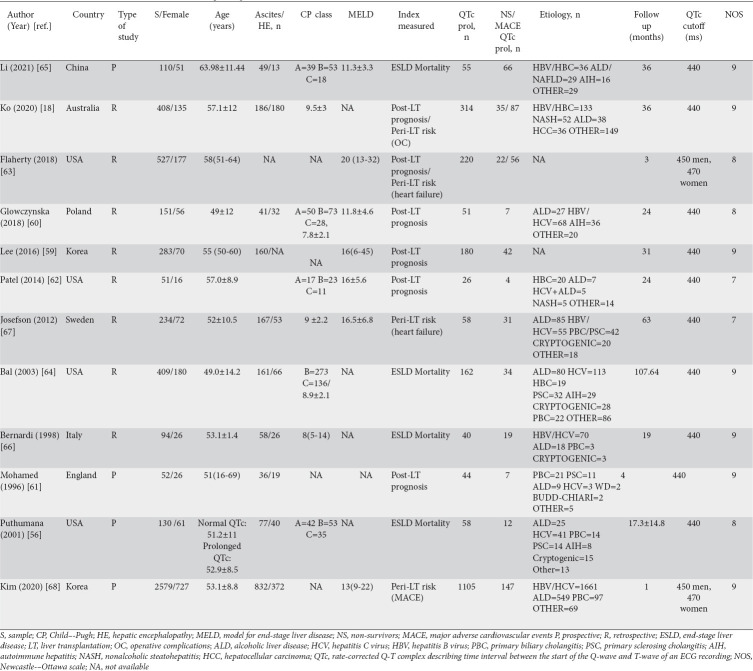
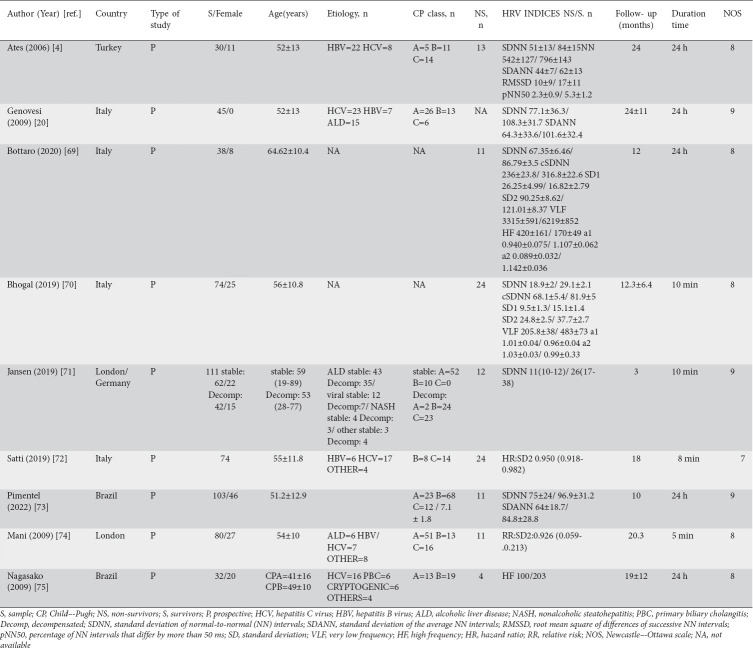
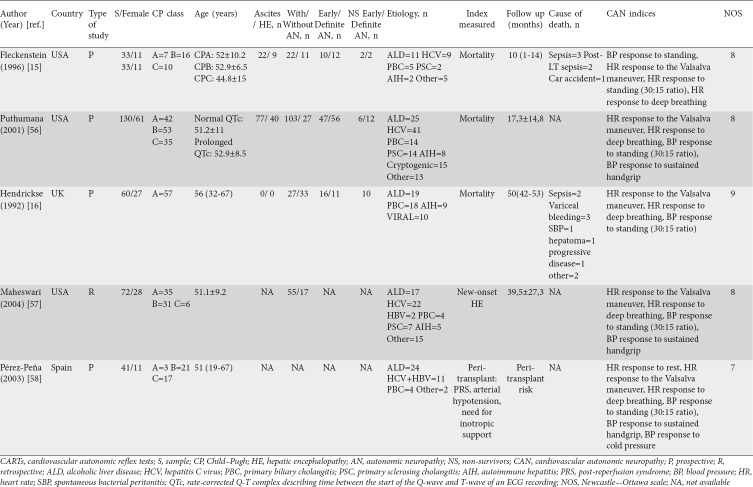
Methods: We searched for all articles published until September 2023 that described a diagnosis of AN based on cardiovascular autonomic reflex tests (CARTs), assessment of the rate-corrected QT interval (QTc), heart rate variability (HRV), and baroreflex sensitivity (BRS) tests, in order to evaluate the predictive role of AN in cirrhosis and/or peri-/post-LT prognosis.
Results: Twenty-five studies were included: 5, 12, 9, and 1 study, respectively, assessed the predictive role of CARTs, prolonged QTc, HRV indices, and BRS in cirrhosis or peri-/post-LT prognosis. In CARTs-based analysis, the pre-LT pooled mortality rate was significantly higher in cirrhotics with AN compared to those without AN (20% vs. 6%; P=0.01). However, no difference was found between patients with and without pre-LT prolonged QTc in the pre-LT pooled mortality rates (41% vs. 18%; P=0.08), pooled peri-transplant risk of major complications (29% vs. 17%; P=0.08) or post-LT pooled mortality rates (15% vs. 12%; P=0.36). In HRV-based analysis, the standard deviation of normal-to-normal intervals was significantly lower in non-survivors, compared to survivors with cirrhosis: standardized mean difference -2.59, 95% confidence interval -4.75 to -0.43; P=0.04.
Conclusions: The presence of CARTs- and HRV-based AN was a good predictor of mortality in the pre-LT setting. Preoperative prolonged QTc did not seem to be associated with the outcome before or after LT.
背景:肝硬化患者的自主神经病变(AN)与肝硬化相关并发症的高风险以及肝移植(LT)前、中或后的不良预后有关。然而,目前仅有少数几项研究,且结果不一致:我们检索了截至2023年9月发表的所有文章,这些文章描述了基于心血管自主神经反射测试(CARTs)、速率校正QT间期(QTc)评估、心率变异性(HRV)和巴反射敏感性(BRS)测试的AN诊断,以评估AN在肝硬化和/或肝移植前后预后中的预测作用:结果:共纳入 25 项研究:分别有5、12、9和1项研究评估了CARTs、QTc延长、心率变异指数和BRS对肝硬化或LT前后预后的预测作用。在基于 CARTs 的分析中,与无 AN 的肝硬化患者相比,有 AN 的肝硬化患者在 LT 前的总死亡率明显更高(20% 对 6%;P=0.01)。然而,在LT前集合死亡率(41% vs. 18%;P=0.08)、主要并发症围移植期集合风险(29% vs. 17%;P=0.08)或LT后集合死亡率(15% vs. 12%;P=0.36)方面,有和没有LT前QTc延长的患者没有差异。在基于心率变异的分析中,与患有肝硬化的幸存者相比,非幸存者的正常与正常间期的标准偏差显著较低:标准化平均差异为-2.59,95%置信区间为-4.75至-0.43;P=0.04:CARTs和基于心率变异的AN的存在能很好地预测LT术前的死亡率。术前QTc延长似乎与LT前后的结果无关。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


