{"title":"Editorial: Adult Allergy Action Plan","authors":"Steve Till, Katherine Powrie, Shifa Shaikh","doi":"10.1111/cea.14559","DOIUrl":null,"url":null,"abstract":"<p>Allergy Action Plans (AAPs) represent an essential tool in management of patients with severe allergies who are at risk of anaphylaxis. Such plans must provide clear and concise guidance on how to recognise and treat severe allergic reactions including anaphylaxis, and should align where possible, with the latest clinical treatment guidelines. Although allergic reactions may occur at any age, historically most AAPs have included information to facilitate recognition by parents or carers of allergic symptoms that are more relevant to children such as ‘change in behaviour’ or becoming ‘floppy’. These plans are not appropriate for adults, for whom self-recognition of symptoms as well as self-administration of adrenaline autoinjectors is far more likely to be needed.</p><p>Adults may be exposed to allergens in various settings, such as at work, social gatherings or while travelling. The purpose of an AAP is to provide clear instruction to ensure that adults are prepared to handle allergic reactions promptly and effectively. To do this, the AAP should provide information which enables adults to recognise the symptoms of anaphylaxis so that they know <i>when</i> to treat an allergic reaction with adrenaline, such as in the event of difficulty breathing or dizziness, and when repeat administration with a second device is necessary [<span>1</span>]. Conversely, an AAP can help adults differentiate anaphylaxis from mild/moderate allergic reactions that need not require adrenaline, such as hives, or symptoms of a more non-specific nature, such as throat tightness. The plan also advises on additional measures that need to be taken, that is, calling emergency services and mitigating hypotension by lying flat with leg elevation.</p><p>A national audit in 2017 by the BSACI Nurses Committee found that 46% of adults prescribed an adrenaline autoinjector were not provided with an accompanying written emergency treatment plan to support its use. One potential reason for this is a lack of access to adult-specific AAPs, including those that are up to date with current anaphylaxis management guidelines as well as being aligned with UK Medicines and Healthcare Products Regulatory Agency (MHRA) recommendations [<span>2</span>].</p><p>For this reason, the BSACI undertook to develop an open-access Adult AAP in collaboration with national allergy patient charities, Allergy UK and Anaphylaxis UK, with oversight from the BSACI Standards of Care Committee (SOCC).</p><p>An initial assessment of existing anaphylaxis plans was undertaken, including those from the American Academy of Allergy, Asthma and Immunology, Australasian Society of Allergy and Clinical Immunology, the BSACI Paediatric Allergy Plans, manufacturer proprietary plans and the latest MHRA guidance on the use of autoinjectors. Following this evaluation, additional elements identified for inclusion were pictorial device-specific instructions, positioning advice and a health professional signature to validate the advice provided.</p><p>Initially, the option of modifying the current BSACI paediatric allergy plans was explored. However, it was felt that whereas the paediatric plan served to guide adults treating children, this was not suited to adults self-managing anaphylaxis.</p><p>A consensus emerged during the consultation that clinicians could specify the antihistamine patients should take, with a recommendation that first-generation sedating forms should be avoided. Discussions about respiratory symptom recognition arrived at a consensus on describing airway compromise as involving difficulty talking/hoarseness, difficult or noisy breathing and wheezing or persistent cough. There were differing views regarding whether emergency treatment should include the use of Salbutamol for inhaler-carrying patients. However, to minimise the risk of delaying administering adrenaline, this recommendation was omitted, although there was extensive discussion about this and acknowledgement that in some instances a selective beta-2 agonist might be a better first-line option than IM adrenaline in those primarily experiencing bronchospasm. The original plan was then amended to fit the instructions for use from the manufacturers of each individual AAI device, eventually resulting in the development of three individual plans for each autoinjector available in the UK.</p><p>The plan underwent review by the Standards of Care Committee (SOCC), with feedback relayed to the BSACI Nurses Committee, Adult Allergy Committee and the Transition Group. The Paediatric Committee also contributed insights. During this final process, the main contention was the extent to which the plan should mirror the paediatric action plans, with the aim of easing of transition. Finally, some components of the paediatric AAPs were retained alongside key points considered more relevant to adults. The plan was signed off by the SOCC in March 2023 (Figures 1 and 2).</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 9","pages":"644-646"},"PeriodicalIF":6.3000,"publicationDate":"2024-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14559","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14559","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Allergy Action Plans (AAPs) represent an essential tool in management of patients with severe allergies who are at risk of anaphylaxis. Such plans must provide clear and concise guidance on how to recognise and treat severe allergic reactions including anaphylaxis, and should align where possible, with the latest clinical treatment guidelines. Although allergic reactions may occur at any age, historically most AAPs have included information to facilitate recognition by parents or carers of allergic symptoms that are more relevant to children such as ‘change in behaviour’ or becoming ‘floppy’. These plans are not appropriate for adults, for whom self-recognition of symptoms as well as self-administration of adrenaline autoinjectors is far more likely to be needed.
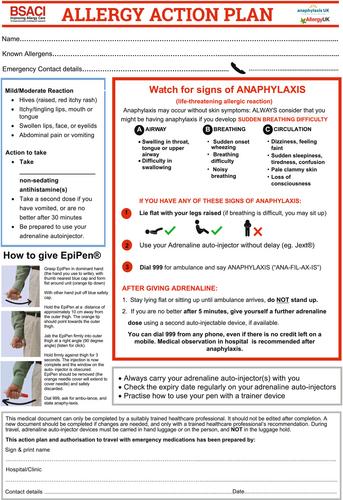
Adults may be exposed to allergens in various settings, such as at work, social gatherings or while travelling. The purpose of an AAP is to provide clear instruction to ensure that adults are prepared to handle allergic reactions promptly and effectively. To do this, the AAP should provide information which enables adults to recognise the symptoms of anaphylaxis so that they know when to treat an allergic reaction with adrenaline, such as in the event of difficulty breathing or dizziness, and when repeat administration with a second device is necessary [1]. Conversely, an AAP can help adults differentiate anaphylaxis from mild/moderate allergic reactions that need not require adrenaline, such as hives, or symptoms of a more non-specific nature, such as throat tightness. The plan also advises on additional measures that need to be taken, that is, calling emergency services and mitigating hypotension by lying flat with leg elevation.
A national audit in 2017 by the BSACI Nurses Committee found that 46% of adults prescribed an adrenaline autoinjector were not provided with an accompanying written emergency treatment plan to support its use. One potential reason for this is a lack of access to adult-specific AAPs, including those that are up to date with current anaphylaxis management guidelines as well as being aligned with UK Medicines and Healthcare Products Regulatory Agency (MHRA) recommendations [2].
For this reason, the BSACI undertook to develop an open-access Adult AAP in collaboration with national allergy patient charities, Allergy UK and Anaphylaxis UK, with oversight from the BSACI Standards of Care Committee (SOCC).
An initial assessment of existing anaphylaxis plans was undertaken, including those from the American Academy of Allergy, Asthma and Immunology, Australasian Society of Allergy and Clinical Immunology, the BSACI Paediatric Allergy Plans, manufacturer proprietary plans and the latest MHRA guidance on the use of autoinjectors. Following this evaluation, additional elements identified for inclusion were pictorial device-specific instructions, positioning advice and a health professional signature to validate the advice provided.
Initially, the option of modifying the current BSACI paediatric allergy plans was explored. However, it was felt that whereas the paediatric plan served to guide adults treating children, this was not suited to adults self-managing anaphylaxis.
A consensus emerged during the consultation that clinicians could specify the antihistamine patients should take, with a recommendation that first-generation sedating forms should be avoided. Discussions about respiratory symptom recognition arrived at a consensus on describing airway compromise as involving difficulty talking/hoarseness, difficult or noisy breathing and wheezing or persistent cough. There were differing views regarding whether emergency treatment should include the use of Salbutamol for inhaler-carrying patients. However, to minimise the risk of delaying administering adrenaline, this recommendation was omitted, although there was extensive discussion about this and acknowledgement that in some instances a selective beta-2 agonist might be a better first-line option than IM adrenaline in those primarily experiencing bronchospasm. The original plan was then amended to fit the instructions for use from the manufacturers of each individual AAI device, eventually resulting in the development of three individual plans for each autoinjector available in the UK.
The plan underwent review by the Standards of Care Committee (SOCC), with feedback relayed to the BSACI Nurses Committee, Adult Allergy Committee and the Transition Group. The Paediatric Committee also contributed insights. During this final process, the main contention was the extent to which the plan should mirror the paediatric action plans, with the aim of easing of transition. Finally, some components of the paediatric AAPs were retained alongside key points considered more relevant to adults. The plan was signed off by the SOCC in March 2023 (Figures 1 and 2).
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


