Michael L. Savage BAppSc, Karen Hay BVSc, PhD, William Vollbon BAppSc, Dale J. Murdoch MBBS, FRACP, Christopher Hammett MBChB, MD, FRACP, James Crowhurst BSc (Hons), PhD, Karl Poon MBBS, FRACP, Rohan Poulter MBBS, FRACP, Darren L. Walters MBBS, FRACP, MPhil, Russell Denman MBBS, FRACP, Isuru Ranasinghe MBChB, MMed, PhD, FRACP, Owen Christopher Raffel MB, CHB, FRACP
{"title":"Differences between sexes in STEMI treatment and outcomes with contemporary primary PCI","authors":"Michael L. Savage BAppSc, Karen Hay BVSc, PhD, William Vollbon BAppSc, Dale J. Murdoch MBBS, FRACP, Christopher Hammett MBChB, MD, FRACP, James Crowhurst BSc (Hons), PhD, Karl Poon MBBS, FRACP, Rohan Poulter MBBS, FRACP, Darren L. Walters MBBS, FRACP, MPhil, Russell Denman MBBS, FRACP, Isuru Ranasinghe MBChB, MMed, PhD, FRACP, Owen Christopher Raffel MB, CHB, FRACP","doi":"10.1002/ccd.31206","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Historically, differences in timely reperfusion and outcomes have been described in females who suffer ST-segment elevation myocardial infarction (STEMI). However, there have been improvements in the treatment of STEMI patients with contemporary Percutaneous Coronary Intervention (PCI) strategies.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Comparisons between sexes were performed on STEMI patients treated with primary PCI over a 4-year period (January 1, 2017–December 31, 2020) from the Queensland Cardiac Outcomes Registry. Primary outcomes were 30-day and 1-year cardiovascular mortality. Secondary outcomes were STEMI performance measures. The total and direct effects of gender on mortality outcomes were estimated using logistic and multinomial logistic regression models.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Overall, 2747 (76% male) were included. Females were on average older (65.9 vs. 61.9 years; <i>p</i> < 0.001), had longer total ischemic time (69 min vs. 52 min; <i>p</i> < 0.001) and less achievement of STEMI performance targets (<90 min) (50% vs. 58%; <i>p</i> < 0.001). There was no evidence for a total (odds ratio [OR] 1.3 (95% confidence interval [CI]: 0.8–2.2; <i>p</i> = 0.35) or direct (adjusted OR 1.2 (95% CI: 0.7–2.1; <i>p</i> = 0.58) effect of female sex on 30-day mortality. One-year mortality was higher in females (6.9% vs. 4.4%; <i>p</i> = 0.014) with total effect estimates consistent with increased risk of cardiovascular mortality (Incidence rate ratio [IRR]: 1.5; 95% CI: 1.0–2.3; <i>p</i> = 0.059) and noncardiovascular mortality (IRR: 2.1; 95% CI: 0.9–4.7; <i>p</i> = 0.077) in females. However, direct (adjusted) effect estimates of cardiovascular mortality (IRR: 1.0; 95% CI: 0.6–1.6; <i>p</i> = 0.94) indicated sex differences were explained by confounders and mediators.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Small sex differences in STEMI performance measures still exist; however, with contemporary primary PCI strategies, sex is not associated with cardiovascular mortality at 30 days or 1 year.</p>\n </section>\n </div>","PeriodicalId":9650,"journal":{"name":"Catheterization and Cardiovascular Interventions","volume":"104 5","pages":"934-944"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ccd.31206","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Catheterization and Cardiovascular Interventions","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ccd.31206","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Historically, differences in timely reperfusion and outcomes have been described in females who suffer ST-segment elevation myocardial infarction (STEMI). However, there have been improvements in the treatment of STEMI patients with contemporary Percutaneous Coronary Intervention (PCI) strategies.
Methods
Comparisons between sexes were performed on STEMI patients treated with primary PCI over a 4-year period (January 1, 2017–December 31, 2020) from the Queensland Cardiac Outcomes Registry. Primary outcomes were 30-day and 1-year cardiovascular mortality. Secondary outcomes were STEMI performance measures. The total and direct effects of gender on mortality outcomes were estimated using logistic and multinomial logistic regression models.
Results
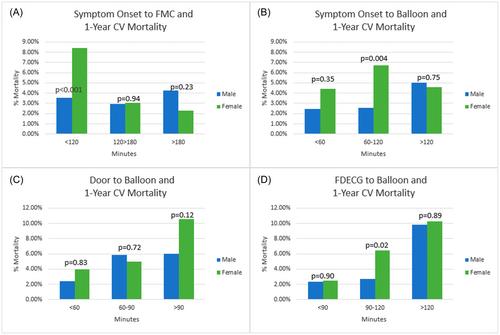
Overall, 2747 (76% male) were included. Females were on average older (65.9 vs. 61.9 years; p < 0.001), had longer total ischemic time (69 min vs. 52 min; p < 0.001) and less achievement of STEMI performance targets (<90 min) (50% vs. 58%; p < 0.001). There was no evidence for a total (odds ratio [OR] 1.3 (95% confidence interval [CI]: 0.8–2.2; p = 0.35) or direct (adjusted OR 1.2 (95% CI: 0.7–2.1; p = 0.58) effect of female sex on 30-day mortality. One-year mortality was higher in females (6.9% vs. 4.4%; p = 0.014) with total effect estimates consistent with increased risk of cardiovascular mortality (Incidence rate ratio [IRR]: 1.5; 95% CI: 1.0–2.3; p = 0.059) and noncardiovascular mortality (IRR: 2.1; 95% CI: 0.9–4.7; p = 0.077) in females. However, direct (adjusted) effect estimates of cardiovascular mortality (IRR: 1.0; 95% CI: 0.6–1.6; p = 0.94) indicated sex differences were explained by confounders and mediators.
Conclusion
Small sex differences in STEMI performance measures still exist; however, with contemporary primary PCI strategies, sex is not associated with cardiovascular mortality at 30 days or 1 year.
期刊介绍:
Catheterization and Cardiovascular Interventions is an international journal covering the broad field of cardiovascular diseases. Subject material includes basic and clinical information that is derived from or related to invasive and interventional coronary or peripheral vascular techniques. The journal focuses on material that will be of immediate practical value to physicians providing patient care in the clinical laboratory setting. To accomplish this, the journal publishes Preliminary Reports and Work In Progress articles that complement the traditional Original Studies, Case Reports, and Comprehensive Reviews. Perspective and insight concerning controversial subjects and evolving technologies are provided regularly through Editorial Commentaries furnished by members of the Editorial Board and other experts. Articles are subject to double-blind peer review and complete editorial evaluation prior to any decision regarding acceptability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


