{"title":"Retroactive blood-borne pathogens detection of archival clotting factor concentrates throughout the 1970s and 1980s highlights virus contaminations","authors":"Morgan Brisse, Hinh Ly","doi":"10.1002/jmv.29907","DOIUrl":null,"url":null,"abstract":"<p>Blood coagulation relies on a cascade of protein-protein interactions that comprise two primary downstream pathways (intrinsic and extrinsic<span><sup>1</sup></span>). Individuals deficient in certain coagulation pathway proteins, also known as clotting factors, may present with primary or secondary bleeding disorders (coagulopathies). For example, hemophilia results from genetic alterations to factors VIII, IX or XI,<span><sup>2</sup></span> while secondary bleeding disorders may result from dysregulation of clotting factors caused by underlying conditions,<span><sup>3-5</sup></span> medication use,<span><sup>6</sup></span> or infection.<span><sup>7-9</sup></span> Concentrated coagulation factors derived from human blood donations have been made available for treating bleeding disorders since the 1970s.<span><sup>10, 11</sup></span> However, therapeutic coagulation-factor use was found in the 1980s to be associated with a significantly increased risk of developing disease from the then newly discovered blood-borne pathogens (BBPs), such as human immunodeficiency virus-1 (HIV-1, discovered in 1983) and hepatitis C virus (HCV, discovered in 1990).<span><sup>12-15</sup></span> Measures were subsequently put into place throughout the mid-to-late 1980s and early 1990s to limit BBP spread to patients, who were using clotting factor products. Those practices included viral detection, viral exclusion and inactivation, and blood donor screening.</p><p>The degree of viral burden carried by clotting factor products before viral exclusion practices remained unknown with regard to contamination with HCV, HIV-1 and/or other BBPs that had since been found in patients with hemophilia (PWHs).<span><sup>16-19</sup></span> The authors of a newly published article in the Journal of Medical Virology<span><sup>20</sup></span> retrospectively identified BBPs present in 24 lyophilized clotting factor samples (14 commercially produced clothing factors and 10 from non-remunerated blood donors) taken from three time periods: 1974–1977, 1981–1985 and 1989–1992. Blood factor products (either single coagulation factor or a combination of the factors) came from commercial and nationalized (British and French blood bank) sources and were sorted by their listed expiration dates (Figure 1), as production date for each of them was not recorded. Using established or in-house developed qPCR assays, the authors intended to test those products for HIV-1, HIV-2, hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), and hepatitis E virus (HEV), human pegiviruses 1 and 2 (HPgV1, HPgV2), and the parvoviruses B19V and PARV4. It is important to note that while the authors stated in the abstract that HIV-2 would be part of a panel of BBPs to be tested, they did not report the result of this test in the subsequent sections of the manuscript. It is, therefore, unclear whether this had been done for this study. Regardless, samples identified as positive for HCV or HIV-1 were subjected to Illumina or Sanger sequencing for virus strain detection and for comparison to historic and currently circulating strains of those BBPs.</p><p>For products with an expiry date as early as 1976, all tested viruses were found, except for HEV. The authors theorized, however, that samples from 1974 to 1975 might all have been tested negative for viral burden due to smaller pools of plasma used for product purification during that period. HIV-1, HAV and HBV were also only identified in 3/24, 1/24 and 1/24 samples, respectively. By 1983-1984, HCV levels peaked several logs higher than 1976 levels and were identifiable in all samples from 1981 to 1985 and were present at relatively low levels in only one sample post 1989. HIV-1 was identified in two samples at relatively low levels (1983 and 1985) and one sample at relatively high levels (1983), which was consistent with the sporadic presence of HIV-1<span><sup>21</sup></span> in clotting factor products tested in the 1980s and was also corresponding with the period of time when the highest numbers of seroconverted PWHs were identified in the UK.<span><sup>22</sup></span> HAV and HBV were only detected in a single sample each and none were positive for HEV. These findings suggest that while PWHs were known to have high incidence rates of HBV,<span><sup>23, 24</sup></span> they had a relatively low level of additional exposure to HAV<span><sup>25, 26</sup></span> and HEV.<span><sup>27, 28</sup></span> Transmission of HBV was found to occur even in HBV antigen-negative plasma,<span><sup>23, 29</sup></span> suggesting that HBV infection might have required a very small number of infectious virus particles to be present in clotting factors.<span><sup>30, 31</sup></span> Illumina sequencing of positive samples identified five HCV genotypes that were all identified in UK PWHs at the time,<span><sup>32-34</sup></span> which corresponded with previous studies showing a close correlation between the virus genotypes identified in affected PWHs and the virus genotypes circulating in local populations.<span><sup>35</sup></span> Only one out of three of the HIV-positive samples successfully underwent Sanger sequencing, which contained a closely matched virus sequence of a serum sample taken in California in 1978.<span><sup>36</sup></span></p><p>The other three tested BBPs (HPgV-1 and the parvoviruses B19V and PARV4) were readily identifiable in the tested coagulant factor samples, with HPgV-1 and B19V being consistently present from 1975 to 1985 and 1991, respectively, which notably for B19V continued well past the initiation of virus inactivation procedures and was likely influenced by the natural feature of parvoviruses that are resistant to heat and detergent inactivation.<span><sup>37</sup></span> PARV4 was more sporadically detected from 1976 to 1984, and the lack of positivity of either parvovirus from the tested coagulation products by 1992 suggests that other mitigation methods (such as screening blood donors for risk factors associated with BBP acquisition) may have eventually helped control parvovirus burden before the introduction of more comprehensive and sensitive viral nucleic-acid detection methods. These three tested BBPs (HPgV-1 and the parvoviruses B19V and PARV4) are also most associated with disease development in immunocompromised individuals, making their detections additionally difficult.</p><p>In summary, this manuscript provides evidence of BBP contaminations of the commercial purified coagulation product supplies throughout the 1970s and 1980s and prior to the introduction of viral exclusion and screening procedures. Specifically, the authors of the study found that HCV, B19V and HPgV-1 were the most frequently detected viruses in all 24 tested samples and primarily in commercial clotting factors at extremely high viral loads in the late 1970s–1985 (Figure 1) and with a diverse range of virus genotypes. However, the detection frequencies of those blood-borne viruses sharply declined following the introduction of virus inactivation methods. On the other hand, HIV-1, HAV and HBV were less frequently detected, that is, only in 3/24, 1/24, and 1/24 tested samples, respectively, and no HEV was present in those samples. In contrast, B19V and PARV4 were detected throughout the study period, even after introduction of dry heat treatment, which was consistent with documented B19V and PARV4 transmissions to PWHs during that period (and into the early 1990s). In spite of this being a retrospective study, it highlights the need for continued vigilance to conduct BBP screening of human (and animal) blood products as well as to further the development of synthetically or recombinantly manufactured clotting products,<span><sup>38</sup></span> especially for therapeutic products that are intended to be given repeatedly to patients over significant periods of time, which can raise the risk for BBP exposure with each subsequent infusion. It is important to note that viral genomic detection does not necessarily equate infectious virus or the potential of onward risk of transmission. Finally, this work adds to a growing body of retrospective literature identifying different viruses and viral genotypes in historic samples that would provide a unique opportunity for a more comprehensive analysis of viral evolution in humans over an extended period.</p>","PeriodicalId":16354,"journal":{"name":"Journal of Medical Virology","volume":null,"pages":null},"PeriodicalIF":6.8000,"publicationDate":"2024-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jmv.29907","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Virology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jmv.29907","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"VIROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Blood coagulation relies on a cascade of protein-protein interactions that comprise two primary downstream pathways (intrinsic and extrinsic1). Individuals deficient in certain coagulation pathway proteins, also known as clotting factors, may present with primary or secondary bleeding disorders (coagulopathies). For example, hemophilia results from genetic alterations to factors VIII, IX or XI,2 while secondary bleeding disorders may result from dysregulation of clotting factors caused by underlying conditions,3-5 medication use,6 or infection.7-9 Concentrated coagulation factors derived from human blood donations have been made available for treating bleeding disorders since the 1970s.10, 11 However, therapeutic coagulation-factor use was found in the 1980s to be associated with a significantly increased risk of developing disease from the then newly discovered blood-borne pathogens (BBPs), such as human immunodeficiency virus-1 (HIV-1, discovered in 1983) and hepatitis C virus (HCV, discovered in 1990).12-15 Measures were subsequently put into place throughout the mid-to-late 1980s and early 1990s to limit BBP spread to patients, who were using clotting factor products. Those practices included viral detection, viral exclusion and inactivation, and blood donor screening.
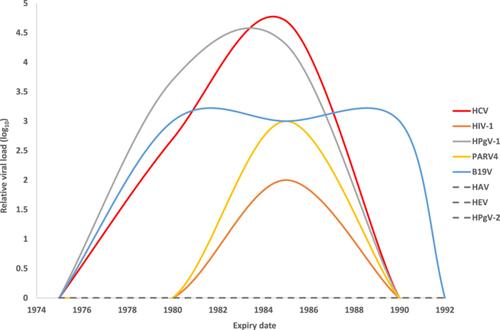
The degree of viral burden carried by clotting factor products before viral exclusion practices remained unknown with regard to contamination with HCV, HIV-1 and/or other BBPs that had since been found in patients with hemophilia (PWHs).16-19 The authors of a newly published article in the Journal of Medical Virology20 retrospectively identified BBPs present in 24 lyophilized clotting factor samples (14 commercially produced clothing factors and 10 from non-remunerated blood donors) taken from three time periods: 1974–1977, 1981–1985 and 1989–1992. Blood factor products (either single coagulation factor or a combination of the factors) came from commercial and nationalized (British and French blood bank) sources and were sorted by their listed expiration dates (Figure 1), as production date for each of them was not recorded. Using established or in-house developed qPCR assays, the authors intended to test those products for HIV-1, HIV-2, hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), and hepatitis E virus (HEV), human pegiviruses 1 and 2 (HPgV1, HPgV2), and the parvoviruses B19V and PARV4. It is important to note that while the authors stated in the abstract that HIV-2 would be part of a panel of BBPs to be tested, they did not report the result of this test in the subsequent sections of the manuscript. It is, therefore, unclear whether this had been done for this study. Regardless, samples identified as positive for HCV or HIV-1 were subjected to Illumina or Sanger sequencing for virus strain detection and for comparison to historic and currently circulating strains of those BBPs.
For products with an expiry date as early as 1976, all tested viruses were found, except for HEV. The authors theorized, however, that samples from 1974 to 1975 might all have been tested negative for viral burden due to smaller pools of plasma used for product purification during that period. HIV-1, HAV and HBV were also only identified in 3/24, 1/24 and 1/24 samples, respectively. By 1983-1984, HCV levels peaked several logs higher than 1976 levels and were identifiable in all samples from 1981 to 1985 and were present at relatively low levels in only one sample post 1989. HIV-1 was identified in two samples at relatively low levels (1983 and 1985) and one sample at relatively high levels (1983), which was consistent with the sporadic presence of HIV-121 in clotting factor products tested in the 1980s and was also corresponding with the period of time when the highest numbers of seroconverted PWHs were identified in the UK.22 HAV and HBV were only detected in a single sample each and none were positive for HEV. These findings suggest that while PWHs were known to have high incidence rates of HBV,23, 24 they had a relatively low level of additional exposure to HAV25, 26 and HEV.27, 28 Transmission of HBV was found to occur even in HBV antigen-negative plasma,23, 29 suggesting that HBV infection might have required a very small number of infectious virus particles to be present in clotting factors.30, 31 Illumina sequencing of positive samples identified five HCV genotypes that were all identified in UK PWHs at the time,32-34 which corresponded with previous studies showing a close correlation between the virus genotypes identified in affected PWHs and the virus genotypes circulating in local populations.35 Only one out of three of the HIV-positive samples successfully underwent Sanger sequencing, which contained a closely matched virus sequence of a serum sample taken in California in 1978.36
The other three tested BBPs (HPgV-1 and the parvoviruses B19V and PARV4) were readily identifiable in the tested coagulant factor samples, with HPgV-1 and B19V being consistently present from 1975 to 1985 and 1991, respectively, which notably for B19V continued well past the initiation of virus inactivation procedures and was likely influenced by the natural feature of parvoviruses that are resistant to heat and detergent inactivation.37 PARV4 was more sporadically detected from 1976 to 1984, and the lack of positivity of either parvovirus from the tested coagulation products by 1992 suggests that other mitigation methods (such as screening blood donors for risk factors associated with BBP acquisition) may have eventually helped control parvovirus burden before the introduction of more comprehensive and sensitive viral nucleic-acid detection methods. These three tested BBPs (HPgV-1 and the parvoviruses B19V and PARV4) are also most associated with disease development in immunocompromised individuals, making their detections additionally difficult.
In summary, this manuscript provides evidence of BBP contaminations of the commercial purified coagulation product supplies throughout the 1970s and 1980s and prior to the introduction of viral exclusion and screening procedures. Specifically, the authors of the study found that HCV, B19V and HPgV-1 were the most frequently detected viruses in all 24 tested samples and primarily in commercial clotting factors at extremely high viral loads in the late 1970s–1985 (Figure 1) and with a diverse range of virus genotypes. However, the detection frequencies of those blood-borne viruses sharply declined following the introduction of virus inactivation methods. On the other hand, HIV-1, HAV and HBV were less frequently detected, that is, only in 3/24, 1/24, and 1/24 tested samples, respectively, and no HEV was present in those samples. In contrast, B19V and PARV4 were detected throughout the study period, even after introduction of dry heat treatment, which was consistent with documented B19V and PARV4 transmissions to PWHs during that period (and into the early 1990s). In spite of this being a retrospective study, it highlights the need for continued vigilance to conduct BBP screening of human (and animal) blood products as well as to further the development of synthetically or recombinantly manufactured clotting products,38 especially for therapeutic products that are intended to be given repeatedly to patients over significant periods of time, which can raise the risk for BBP exposure with each subsequent infusion. It is important to note that viral genomic detection does not necessarily equate infectious virus or the potential of onward risk of transmission. Finally, this work adds to a growing body of retrospective literature identifying different viruses and viral genotypes in historic samples that would provide a unique opportunity for a more comprehensive analysis of viral evolution in humans over an extended period.
期刊介绍:
The Journal of Medical Virology focuses on publishing original scientific papers on both basic and applied research related to viruses that affect humans. The journal publishes reports covering a wide range of topics, including the characterization, diagnosis, epidemiology, immunology, and pathogenesis of human virus infections. It also includes studies on virus morphology, genetics, replication, and interactions with host cells.
The intended readership of the journal includes virologists, microbiologists, immunologists, infectious disease specialists, diagnostic laboratory technologists, epidemiologists, hematologists, and cell biologists.
The Journal of Medical Virology is indexed and abstracted in various databases, including Abstracts in Anthropology (Sage), CABI, AgBiotech News & Information, National Agricultural Library, Biological Abstracts, Embase, Global Health, Web of Science, Veterinary Bulletin, and others.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


