Safety, efficacy, and optical coherence tomography insights into intravascular lithotripsy for the modification of non-eruptive calcified nodules: A prospective observational study
Abstract
Background
Non-eruptive calcium nodules (CNs) are commonly seen in heavily calcified coronary artery disease. They are the most difficult subset for modification, and may result in stent damage, malapposition and under-expansion. There are only limited options available for non-eruptive CN modification. Intravascular lithotripsy (IVL) is being explored as a potentially safe and effective modality in these lesions.
Aims
This study aimed to investigate the safety and efficacy of the use of IVL for the modification of non-eruptive CNs. The study also explored the OCT features of calcium nodule modification by IVL.
Methods
This is a single-center, prospective, observational study in which patients with angiographic heavy calcification and non-eruptive CN on OCT and undergoing PCI were enrolled. The primary safety endpoint was freedom from perforation, no-reflow/slow flow, flow-limiting dissection after IVL therapy, and major adverse cardiac events (MACE) during hospitalization and at 30 days. MACE was defined as a composite of cardiac death, myocardial infarction (MI), and ischemia-driven target lesion revascularization (TLR). The primary efficacy endpoint was procedural success, defined as residual diameter stenosis of <30% on angiography and stent expansion of more than 80% as assessed by OCT.
Results
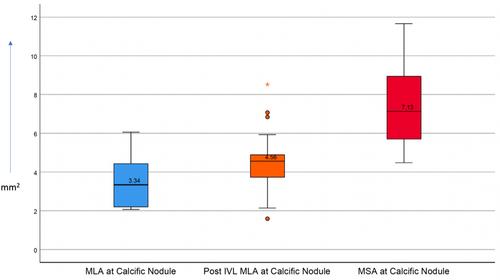
A total of 21 patients with 54 non-eruptive CNs undergoing PCI were prospectively enrolled in the study. Before IVL, OCT revealed a mean calcium score of 3.7 ± 0.5 and a mean MLA at CN of 3.9 ± 2.1 mm2. Following IVL, OCT revealed calcium fractures in 40 out of 54 (74.1%) CNs with an average of 1.05 ± 0.72 fractures per CN. Fractures were predominantly observed at the base of the CN (80%). Post IVL, the mean MLA at CN increased to 4.9 ± 2.3 mm2. After PCI, the mean MSA at the CN was 7.9 ± 2.5 mm2. Optimal stent expansion (stent expansion >80%) at the CN was achieved in 85.71% of patients. All patients remained free from MACE during hospitalization and at the 30-day follow-up. At 1-year follow-up, all-cause death had occurred in 3 (14.3%) patients.
Conclusions
This single-arm study demonstrated the safety, efficacy, and utility of the IVL in a subset of patients with non-eruptive calcified nodules. In this study, minimal procedural complications, excellent lesion modifications, and favorable 30-day and 1-year outcomes were observed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


