Andrew Deak, Syed M Zaidi, Chethan Gangireddy, Edmond Cronin, Eman Hamad, Carly Fabrizio, Sanjana Bhatia-Patel, Val Rakita, Isaac R Whitman
{"title":"Mid-term clinical outcomes and cardiac function in patients receiving cardiac contractility modulation.","authors":"Andrew Deak, Syed M Zaidi, Chethan Gangireddy, Edmond Cronin, Eman Hamad, Carly Fabrizio, Sanjana Bhatia-Patel, Val Rakita, Isaac R Whitman","doi":"10.1007/s10840-024-01900-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To describe the mid-term clinical and functional cardiac contractility modulation therapy (CCM) recipients in an urban population with heart failure.</p><p><strong>Background: </strong>CCM is a non-excitatory electrical therapy for patients with systolic heart failure with NYHA class III symptoms and ejection fraction (EF) 25-45%. How CCM affects a broad range of clinical measures, including diastolic dysfunction (DD) and weight change, is unexplored.</p><p><strong>Methods: </strong>We reviewed 31 consecutive patients at our center who underwent CCM implant. NYHA class, hospitalizations, ejection fraction (EF), diastolic function, and weight were compared pre- and post-CCM implant.</p><p><strong>Results: </strong>Mean age and follow-up time was 63 ± 10 years and 1.4 ± 0.8 years, respectively. Mean NYHA class improved by 0.97 functional classes (p < 0.001), and improvement occurred in 68% of patients. Mean annualized hospitalizations improved (0.8 ± 0.8 vs. 0.4 ± 1.0 hospitalizations/year, p = 0.048), and after exclusion of a single outlier, change in annualized days hospitalized also improved (total cohort 3.8 ± 4.7 vs. 3.7 ± 14.8 days/year; p = 0.96; after exclusion, 3.8 ± 4.7 vs. 1.1 ± 1.9 days/year, p < 0.001). Mean EF improved by 8% (p = 0.002), and among those with DD pre-CCM, mean DD improvement was 0.8 \"grades\" (p < 0.001). Mean weight change was 8.5 pounds lost, amounting to 4% of body weight (p = 0.002, p = 0.002, respectively), with 77% of patients having lost weight after CCM. Five patients (16%) experienced procedural complications; incidence skewed toward early implants.</p><p><strong>Conclusion: </strong>In an observational cohort, CCM therapy resulted in improvement in NYHA class, hospitalizations, systolic and diastolic function, and weight.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"579-588"},"PeriodicalIF":2.6000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167296/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-024-01900-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To describe the mid-term clinical and functional cardiac contractility modulation therapy (CCM) recipients in an urban population with heart failure.
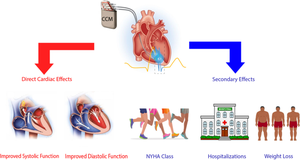
Background: CCM is a non-excitatory electrical therapy for patients with systolic heart failure with NYHA class III symptoms and ejection fraction (EF) 25-45%. How CCM affects a broad range of clinical measures, including diastolic dysfunction (DD) and weight change, is unexplored.
Methods: We reviewed 31 consecutive patients at our center who underwent CCM implant. NYHA class, hospitalizations, ejection fraction (EF), diastolic function, and weight were compared pre- and post-CCM implant.
Results: Mean age and follow-up time was 63 ± 10 years and 1.4 ± 0.8 years, respectively. Mean NYHA class improved by 0.97 functional classes (p < 0.001), and improvement occurred in 68% of patients. Mean annualized hospitalizations improved (0.8 ± 0.8 vs. 0.4 ± 1.0 hospitalizations/year, p = 0.048), and after exclusion of a single outlier, change in annualized days hospitalized also improved (total cohort 3.8 ± 4.7 vs. 3.7 ± 14.8 days/year; p = 0.96; after exclusion, 3.8 ± 4.7 vs. 1.1 ± 1.9 days/year, p < 0.001). Mean EF improved by 8% (p = 0.002), and among those with DD pre-CCM, mean DD improvement was 0.8 "grades" (p < 0.001). Mean weight change was 8.5 pounds lost, amounting to 4% of body weight (p = 0.002, p = 0.002, respectively), with 77% of patients having lost weight after CCM. Five patients (16%) experienced procedural complications; incidence skewed toward early implants.
Conclusion: In an observational cohort, CCM therapy resulted in improvement in NYHA class, hospitalizations, systolic and diastolic function, and weight.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


