Outcomes of definite vs probable/presumed cardiac sarcoidosis: a systematic review and meta-analysis
IF 3
3区 医学
Q2 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
Abstract
Background
Diagnosing cardiac sarcoidosis (CS), which can be associated with arrhythmias and heart failure, remains challenging despite multiple advances over time. The 2014 Heart Rhythm Society (HRS) consensus statement recommends an endomyocardial biopsy (EMB) to establish a definite diagnosis of CS. In the absence of a positive EMB, a diagnosis of probable or presumed CS is made on the basis of clinical and imaging criteria.
Objective
To investigate whether there is any difference in outcomes between definite vs probable/presumed CS.
Methods
PubMed/MEDLINE, Embase, and the Cochrane Library databases were searched for relevant studies published after 2014. Risk ratios (RR) with 95% confidence intervals (CI) were calculated using the random effects model and presented in forest plots.
Results
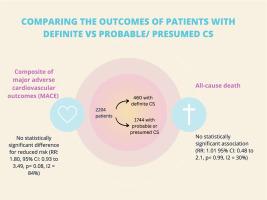
6 studies involving 2,204 patients were identified. The cohort had a mean age of 56.8 years (SD: ±13.6 years). The median duration of follow-up was 40.5 months. No statistically significant difference was observed between definite and probable/presumed CS for reduced risk of the composite endpoint (RR: 1.80, 95% CI: 0.93 to 3.49), and all-cause death (RR: 1.01, 95% CI: 0.48 to 2.10).
Conclusion
This meta-analysis demonstrated the equivalence of clinical course and prognosis between definite and probable/presumed CS. This highlights the importance of a multi-disciplinary approach to CS care and emphasizes that histological confirmation should not be a prerequisite to diagnose or manage this condition.
确诊与可能/推测的心脏肉样瘤病的结果:系统回顾和荟萃分析。
背景:心脏肉样瘤病(CS)可伴有心律失常和心力衰竭,尽管随着时间的推移取得了多项进展,但诊断CS仍具有挑战性。2014 年心律学会(HRS)共识声明建议通过心内膜活检(EMB)明确诊断 CS。如果心内膜活检未呈阳性,则根据临床和影像学标准诊断为可能或推测的 CS:调查确诊 CS 与可能/推测 CS 的结果是否存在差异:方法:检索 PubMed/MEDLINE、Embase 和 Cochrane Library 数据库中 2014 年之后发表的相关研究。采用随机效应模型计算风险比(RR)及95%置信区间(CI),并以森林图的形式展示:结果:共发现 6 项研究,涉及 2,103 名患者。研究队列的平均年龄为 56.8 岁(标准差:±13.6 岁)。随访时间的中位数为 40.5 个月。在降低复合终点风险(RR:1.06,95% CI:0.66 至 1.72)、全因死亡风险(RR:1.03,95% CI:0.73 至 1.46)、心脏性猝死(RR:1.59,95% CI:0.99 至 2.56)、心律失常(RR:0.80,95% CI:0.60 至 1.07)和 HF 相关住院(RR:0.91,95% CI:0.59 至 1.38):这项荟萃分析表明,确诊 CS 和可能/推测 CS 的临床病程和预后相当。这凸显了多学科方法对 CS 护理的重要性,并强调组织学确诊不应成为诊断或处理这种疾病的先决条件。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Current Problems in Cardiology
医学-心血管系统
CiteScore
4.80
自引率
2.40%
发文量
392
审稿时长
6 days
期刊介绍:
Under the editorial leadership of noted cardiologist Dr. Hector O. Ventura, Current Problems in Cardiology provides focused, comprehensive coverage of important clinical topics in cardiology. Each monthly issues, addresses a selected clinical problem or condition, including pathophysiology, invasive and noninvasive diagnosis, drug therapy, surgical management, and rehabilitation; or explores the clinical applications of a diagnostic modality or a particular category of drugs. Critical commentary from the distinguished editorial board accompanies each monograph, providing readers with additional insights. An extensive bibliography in each issue saves hours of library research.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


