Niharika Gummaraj Srinivas, Ye Chen, Angie Mae Rodday, Dami Ko
{"title":"Disparities in Liver Transplant Outcomes: Race/Ethnicity and Individual- and Neighborhood-Level Socioeconomic Status.","authors":"Niharika Gummaraj Srinivas, Ye Chen, Angie Mae Rodday, Dami Ko","doi":"10.1177/10547738241273128","DOIUrl":null,"url":null,"abstract":"<p><p>Race/ethnicity and individual-level socioeconomic status (SES) may contribute to health disparities in liver transplant (LT) outcomes. The socioeconomic conditions of a neighborhood may either mitigate or exacerbate these health disparities. This retrospective study investigated the relationship between race/ethnicity, individual- and neighborhood-level SES, and LT outcomes, and whether neighborhood-level SES modified the relationship between individual factors and LT outcomes. Adult individuals who underwent LT between 2010 and 2019 (<i>n</i> = 55,688) were identified from the United Network for Organ Sharing database. Primary exposures were race/ethnicity, education, primary insurance type, and the Social Deprivation Index (SDI) scores. Education and primary insurance type were used as proxies for individual-level SES, while SDI scores were used as a proxy for neighborhood-level SES. The primary outcome was time to occurrence of graft failure or mortality. Cox proportional hazard models were used to examine the associations between the exposures and outcomes. LT recipients who were Black (hazard ratio [HR]: 1.27, <i>p</i> < .0001), completed high school or less (HR: 1.06, <i>p</i> = .002), and had public insurance (HR: 1.14, <i>p</i> < .0001) had a higher rate of graft failure or mortality than those who were White, completed more than high school, and had private insurance, respectively. The SDI scores were not significantly associated with LT outcomes when adjusting for individual factors (HR: 1.02, <i>p</i> = .45) and did not modify the associations between individual factors and LT outcomes. Findings of this study suggest that disparities based on individual factors were not modified by neighborhood-level SES. Tailored interventions targeting the unique needs associated with race/ethnicity and individual-level SES are needed to optimize LT outcomes.</p>","PeriodicalId":50677,"journal":{"name":"Clinical Nursing Research","volume":" ","pages":"509-518"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11421193/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nursing Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10547738241273128","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
Abstract
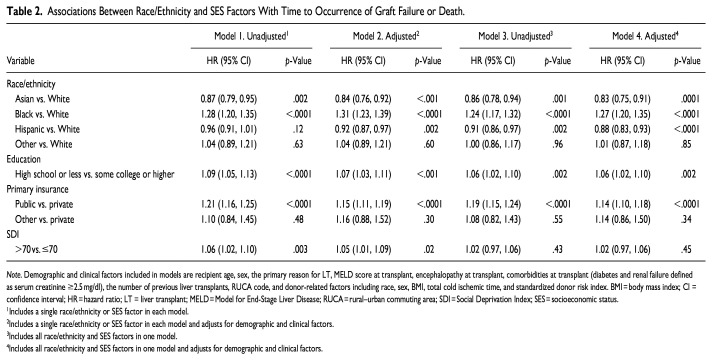
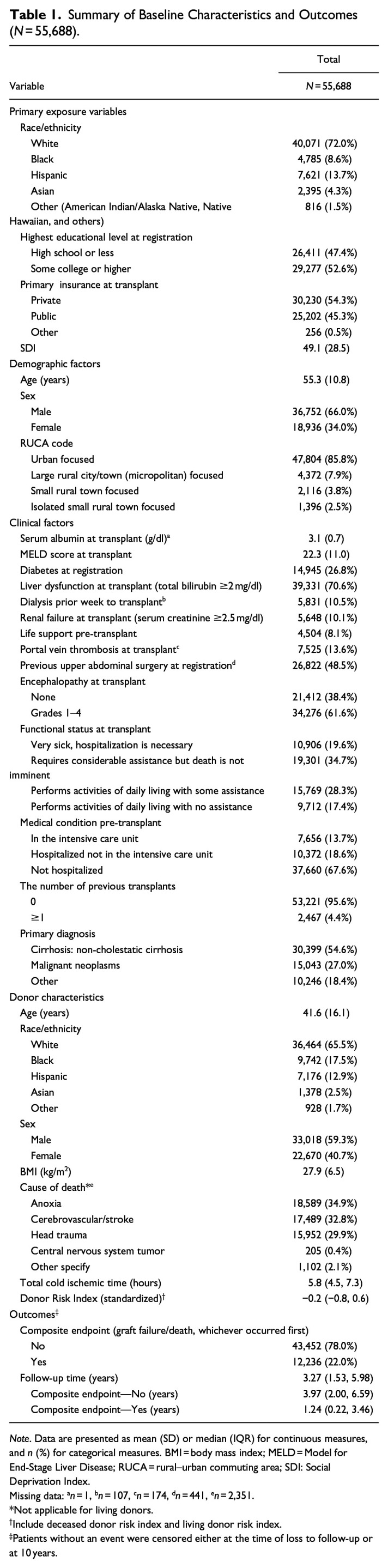
Race/ethnicity and individual-level socioeconomic status (SES) may contribute to health disparities in liver transplant (LT) outcomes. The socioeconomic conditions of a neighborhood may either mitigate or exacerbate these health disparities. This retrospective study investigated the relationship between race/ethnicity, individual- and neighborhood-level SES, and LT outcomes, and whether neighborhood-level SES modified the relationship between individual factors and LT outcomes. Adult individuals who underwent LT between 2010 and 2019 (n = 55,688) were identified from the United Network for Organ Sharing database. Primary exposures were race/ethnicity, education, primary insurance type, and the Social Deprivation Index (SDI) scores. Education and primary insurance type were used as proxies for individual-level SES, while SDI scores were used as a proxy for neighborhood-level SES. The primary outcome was time to occurrence of graft failure or mortality. Cox proportional hazard models were used to examine the associations between the exposures and outcomes. LT recipients who were Black (hazard ratio [HR]: 1.27, p < .0001), completed high school or less (HR: 1.06, p = .002), and had public insurance (HR: 1.14, p < .0001) had a higher rate of graft failure or mortality than those who were White, completed more than high school, and had private insurance, respectively. The SDI scores were not significantly associated with LT outcomes when adjusting for individual factors (HR: 1.02, p = .45) and did not modify the associations between individual factors and LT outcomes. Findings of this study suggest that disparities based on individual factors were not modified by neighborhood-level SES. Tailored interventions targeting the unique needs associated with race/ethnicity and individual-level SES are needed to optimize LT outcomes.
期刊介绍:
Clinical Nursing Research (CNR) is a peer-reviewed quarterly journal that addresses issues of clinical research that are meaningful to practicing nurses, providing an international forum to encourage discussion among clinical practitioners, enhance clinical practice by pinpointing potential clinical applications of the latest scholarly research, and disseminate research findings of particular interest to practicing nurses. This journal is a member of the Committee on Publication Ethics (COPE).


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


