Kosmas Daskalakis, Marina Tsoli, Maria Wedin, Beata Kos-Kudla, Angelika Kogut, Raj Srirajaskanthan, Dominique S V M Clement, Georgios Giovos, Martin O Weickert, Gregory Kaltsas
{"title":"Longitudinal Changes in Ki-67 Indices in Small-Intestinal Neuroendocrine Tumours and Their Impact on Survival.","authors":"Kosmas Daskalakis, Marina Tsoli, Maria Wedin, Beata Kos-Kudla, Angelika Kogut, Raj Srirajaskanthan, Dominique S V M Clement, Georgios Giovos, Martin O Weickert, Gregory Kaltsas","doi":"10.1159/000541101","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The purpose of this study was to evaluate longitudinal changes in Ki-67 indices of SI-NETs and assess the impact of these in overall survival (OS).</p><p><strong>Methods: </strong>We screened 551 patients with SI-NETs diagnosed from 1993, through 2021, identified using the SI-NET databases from five European referral centres. Only patients with well-differentiated tumours and available baseline tumour samples and follow-up re-biopsies were included. For tumour grading, apart from 2017 WHO classification system, we applied a recently proposed SI-NET site-specific modified histopathological grading system with Ki-67 cut-offs of 5 and 10%. Uni- and multivariable regression analyses were used to determine whether there was a difference between OS in SI-NET patients stratified by increment of Ki-67 indices over time and/or progression to a higher grade.</p><p><strong>Results: </strong>We included 45 patients. Median Ki-67 index at SI-NET diagnosis was 2% (range: 0.5-15%). Thirty-three patients had Ki-67 indices <5% (70.2%), 6 had Ki-67: 5-10% (12.8%), and 8 had Ki-67 ≥10% (17%). Mean time to re-biopsy was 48.8 months (SD: ±162.5). At re-biopsy, the median change in Ki-67 index (absolute value; follow-up minus time of diagnosis) was 1% (range: -10 to +38%). An increase in Ki-67 occurred in 20 patients (42.6%); in 14 patients, the change in Ki-67 resulted in progression to higher tumour grade following the modified grading system. Patients with an increment in Ki-67 ≥1% had a median OS of 32.9 months versus 80.5 months in patients without (HR = 5.6, 95% CI: 1.42-22.02; p = 0.014). When applying the novel modified histopathological grading system for SI-NETs, patients with grade progression had a median OS of 32.9 months versus 53.7 months in those without (HR = 4.61, 95% CI: 1.22-13.54; p = 0.022). At multivariable analysis, grade progression was confirmed as an independent predictor for death (HR = 7.2, 95% CI: 1.58-32.82; p = 0.011).</p><p><strong>Conclusions: </strong>Metachronous increment in Ki-67 indices and related grade progression over time following a site-specific modified histopathological grading system with Ki-67 cut-offs of 5 and 10% is observed in approximately 1/3 of SI-NETs subjected to re-biopsy and it is associated with worse survival outcomes.</p>","PeriodicalId":19117,"journal":{"name":"Neuroendocrinology","volume":" ","pages":"402-410"},"PeriodicalIF":2.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12169796/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuroendocrinology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000541101","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The purpose of this study was to evaluate longitudinal changes in Ki-67 indices of SI-NETs and assess the impact of these in overall survival (OS).
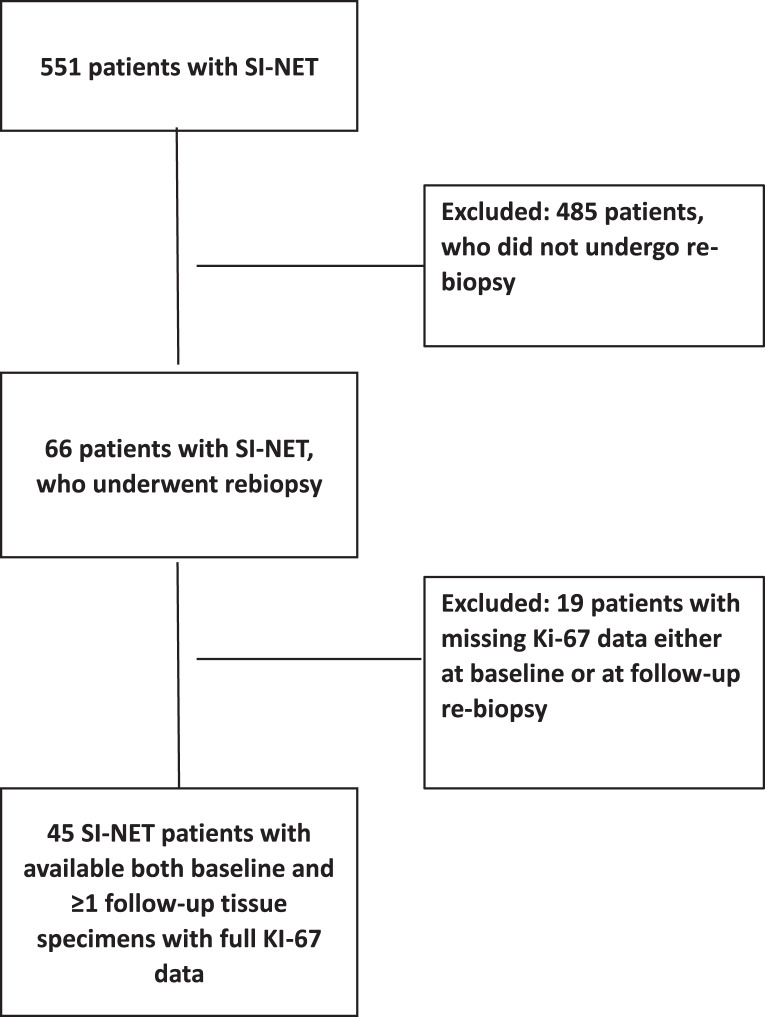
Methods: We screened 551 patients with SI-NETs diagnosed from 1993, through 2021, identified using the SI-NET databases from five European referral centres. Only patients with well-differentiated tumours and available baseline tumour samples and follow-up re-biopsies were included. For tumour grading, apart from 2017 WHO classification system, we applied a recently proposed SI-NET site-specific modified histopathological grading system with Ki-67 cut-offs of 5 and 10%. Uni- and multivariable regression analyses were used to determine whether there was a difference between OS in SI-NET patients stratified by increment of Ki-67 indices over time and/or progression to a higher grade.
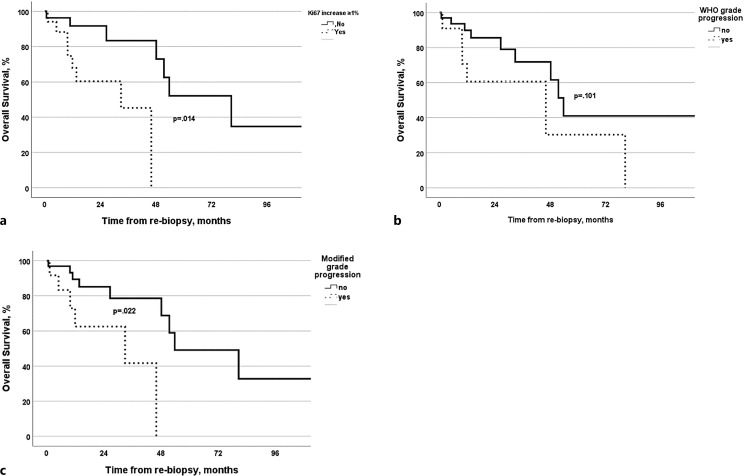
Results: We included 45 patients. Median Ki-67 index at SI-NET diagnosis was 2% (range: 0.5-15%). Thirty-three patients had Ki-67 indices <5% (70.2%), 6 had Ki-67: 5-10% (12.8%), and 8 had Ki-67 ≥10% (17%). Mean time to re-biopsy was 48.8 months (SD: ±162.5). At re-biopsy, the median change in Ki-67 index (absolute value; follow-up minus time of diagnosis) was 1% (range: -10 to +38%). An increase in Ki-67 occurred in 20 patients (42.6%); in 14 patients, the change in Ki-67 resulted in progression to higher tumour grade following the modified grading system. Patients with an increment in Ki-67 ≥1% had a median OS of 32.9 months versus 80.5 months in patients without (HR = 5.6, 95% CI: 1.42-22.02; p = 0.014). When applying the novel modified histopathological grading system for SI-NETs, patients with grade progression had a median OS of 32.9 months versus 53.7 months in those without (HR = 4.61, 95% CI: 1.22-13.54; p = 0.022). At multivariable analysis, grade progression was confirmed as an independent predictor for death (HR = 7.2, 95% CI: 1.58-32.82; p = 0.011).
Conclusions: Metachronous increment in Ki-67 indices and related grade progression over time following a site-specific modified histopathological grading system with Ki-67 cut-offs of 5 and 10% is observed in approximately 1/3 of SI-NETs subjected to re-biopsy and it is associated with worse survival outcomes.
期刊介绍:
''Neuroendocrinology'' publishes papers reporting original research in basic and clinical neuroendocrinology. The journal explores the complex interactions between neuronal networks and endocrine glands (in some instances also immunecells) in both central and peripheral nervous systems. Original contributions cover all aspects of the field, from molecular and cellular neuroendocrinology, physiology, pharmacology, and the neuroanatomy of neuroendocrine systems to neuroendocrine correlates of behaviour, clinical neuroendocrinology and neuroendocrine cancers. Readers also benefit from reviews by noted experts, which highlight especially active areas of current research, and special focus editions of topical interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


