Céline Smekens, Quinten Beirinckx, Frederik Bosmans, Floris Vanhevel, Annemiek Snoeckx, Jan Sijbers, Ben Jeurissen, Thomas Janssens, Pieter Van Dyck
{"title":"Deep Learning-Enhanced Accelerated 2D TSE and 3D Superresolution Dixon TSE for Rapid Comprehensive Knee Joint Assessment.","authors":"Céline Smekens, Quinten Beirinckx, Frederik Bosmans, Floris Vanhevel, Annemiek Snoeckx, Jan Sijbers, Ben Jeurissen, Thomas Janssens, Pieter Van Dyck","doi":"10.1097/RLI.0000000000001118","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to evaluate the use of a multicontrast deep learning (DL)-reconstructed 4-fold accelerated 2-dimensional (2D) turbo spin echo (TSE) protocol and the feasibility of 3-dimensional (3D) superresolution reconstruction (SRR) of DL-enhanced 6-fold accelerated 2D Dixon TSE magnetic resonance imaging (MRI) for comprehensive knee joint assessment, by comparing image quality and diagnostic performance with a conventional 2-fold accelerated 2D TSE knee MRI protocol.</p><p><strong>Materials and methods: </strong>This prospective, ethics-approved study included 19 symptomatic adult subjects who underwent knee MRI on a clinical 3 T scanner. Every subject was scanned with 3 DL-enhanced acquisition protocols in a single session: a clinical standard 2-fold in-plane parallel imaging (PI) accelerated 2D TSE-based protocol (5 sequences, 11 minutes 23 seconds) that served as a reference, a DL-reconstructed 4-fold accelerated 2D TSE protocol combining 2-fold PI and 2-fold simultaneous multislice acceleration (5 sequences, 6 minutes 24 seconds), and a 3D SRR protocol based on DL-enhanced 6-fold accelerated (ie, 3-fold PI and 2-fold simultaneous multislice) 2D Dixon TSE MRI (6 anisotropic 2D Dixon TSE acquisitions rotated around the phase-encoding axis, 6 minutes 24 seconds). This resulted in a total of 228 knee MRI scans comprising 21,204 images. Three readers evaluated all pseudonymized and randomized images in terms of image quality using a 5-point Likert scale. Two of the readers (musculoskeletal radiologists) additionally evaluated anatomical visibility and diagnostic confidence to assess normal and pathological knee structures with a 5-point Likert scale. They recorded the presence and location of internal knee derangements, including cartilage defects, meniscal tears, tears of ligaments, tendons and muscles, and bone injuries. The statistical analysis included nonparametric Friedman tests, and interreader and intrareader agreement assessment using the weighted Fleiss-Cohen kappa (κ) statistic. P values of less than 0.05 were considered statistically significant.</p><p><strong>Results: </strong>The evaluated DL-enhanced 4-fold accelerated 2D TSE protocol provided very similar image quality and anatomical visibility to the standard 2D TSE protocol, whereas the 3D SRR Dixon TSE protocol scored less in terms of overall image quality due to reduced edge sharpness and the presence of artifacts ( P < 0.001). Subjective signal-to-noise ratio, contrast resolution, fluid brightness, and fat suppression were good to excellent for all protocols. For 1 reader, the Dixon method of the 3D SRR protocol provided significantly better fat suppression than the spectral fat saturation applied in the standard 2D TSE protocol ( P < 0.05). The visualization of knee structures with 3D SRR Dixon TSE was very similar to the standard protocol, except for cartilage, tendons, and bone, which were affected by the presence of reconstruction and aliasing artifacts ( P < 0.001). The diagnostic confidence of both readers was high for all protocols and all knee structures, except for cartilage and tendons. The standard 2D TSE protocol showed a significantly higher diagnostic confidence for assessing tendons than 3D SRR Dixon TSE MRI ( P < 0.01). The interreader and intrareader agreement for the assessment of internal knee derangements using any of the 3 protocols was substantial to almost perfect (κ = 0.67-1.00). For cartilage, the interreader agreement was substantial for DL-enhanced accelerated 2D TSE (κ = 0.79) and almost perfect for standard 2D TSE (κ = 0.98) and 3D SRR Dixon TSE (κ = 0.87). For menisci, the interreader agreement was substantial for 3D SRR Dixon TSE (κ = 0.70-0.80) and substantial to almost perfect for standard 2D TSE (κ = 0.80-0.99) and DL-enhanced 2D TSE (κ = 0.87-1.00). Moreover, the total acquisition time was reduced by 44% when using the DL-enhanced accelerated 2D TSE or 3D SRR Dixon TSE protocol instead of the conventional 2D TSE protocol.</p><p><strong>Conclusions: </strong>The presented DL-enhanced 4-fold accelerated 2D TSE protocol provides image quality and diagnostic performance similar to the standard 2D protocol. Moreover, the 3D SRR of DL-enhanced 6-fold accelerated 2D Dixon TSE MRI is feasible for multicontrast 3D knee MRI as its diagnostic performance is comparable to standard 2-fold accelerated 2D knee MRI. However, reconstruction and aliasing artifacts need to be further addressed to guarantee a more reliable visualization and assessment of cartilage, tendons, and bone. Both the 2D and 3D SRR DL-enhanced protocols enable a 44% faster examination compared with conventional 2-fold accelerated routine 2D TSE knee MRI and thus open new paths for more efficient clinical 2D and 3D knee MRI.</p>","PeriodicalId":14486,"journal":{"name":"Investigative Radiology","volume":" ","pages":"220-233"},"PeriodicalIF":8.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11801463/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Investigative Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/RLI.0000000000001118","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/28 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The aim of this study was to evaluate the use of a multicontrast deep learning (DL)-reconstructed 4-fold accelerated 2-dimensional (2D) turbo spin echo (TSE) protocol and the feasibility of 3-dimensional (3D) superresolution reconstruction (SRR) of DL-enhanced 6-fold accelerated 2D Dixon TSE magnetic resonance imaging (MRI) for comprehensive knee joint assessment, by comparing image quality and diagnostic performance with a conventional 2-fold accelerated 2D TSE knee MRI protocol.
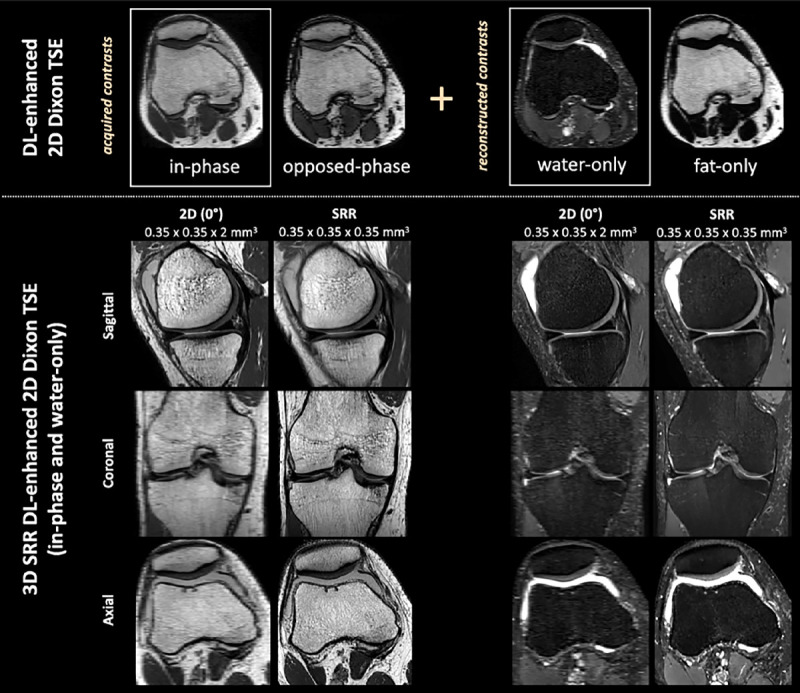
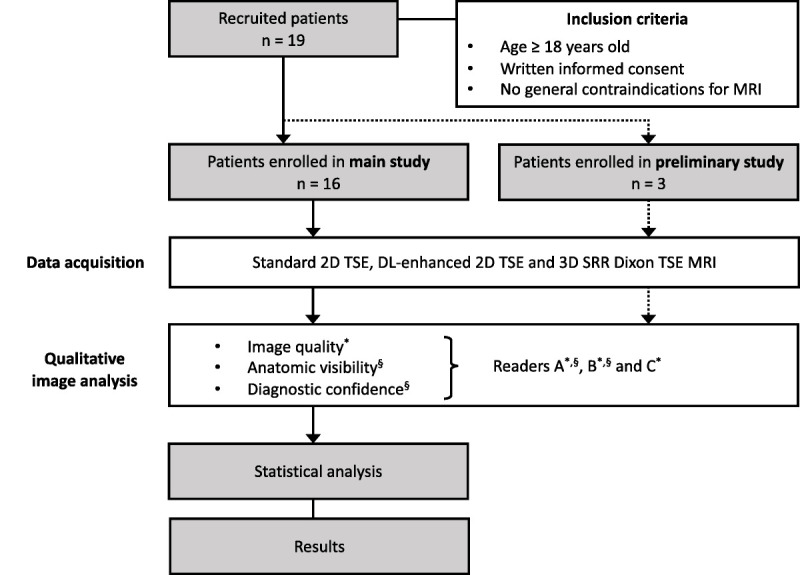
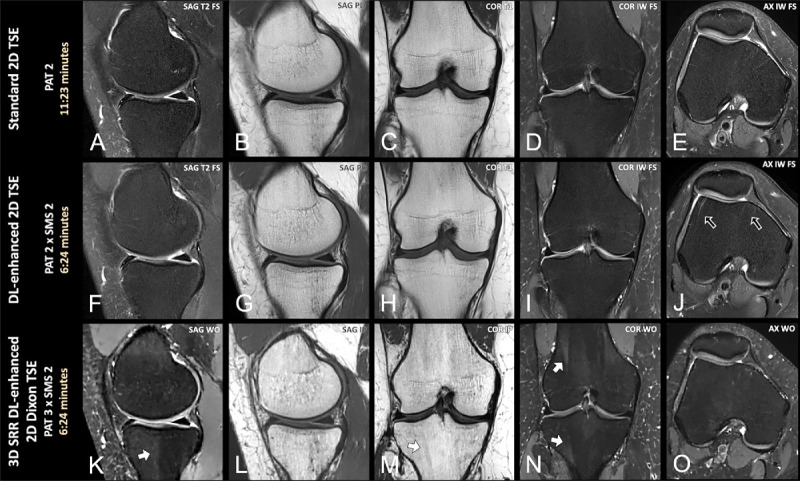
Materials and methods: This prospective, ethics-approved study included 19 symptomatic adult subjects who underwent knee MRI on a clinical 3 T scanner. Every subject was scanned with 3 DL-enhanced acquisition protocols in a single session: a clinical standard 2-fold in-plane parallel imaging (PI) accelerated 2D TSE-based protocol (5 sequences, 11 minutes 23 seconds) that served as a reference, a DL-reconstructed 4-fold accelerated 2D TSE protocol combining 2-fold PI and 2-fold simultaneous multislice acceleration (5 sequences, 6 minutes 24 seconds), and a 3D SRR protocol based on DL-enhanced 6-fold accelerated (ie, 3-fold PI and 2-fold simultaneous multislice) 2D Dixon TSE MRI (6 anisotropic 2D Dixon TSE acquisitions rotated around the phase-encoding axis, 6 minutes 24 seconds). This resulted in a total of 228 knee MRI scans comprising 21,204 images. Three readers evaluated all pseudonymized and randomized images in terms of image quality using a 5-point Likert scale. Two of the readers (musculoskeletal radiologists) additionally evaluated anatomical visibility and diagnostic confidence to assess normal and pathological knee structures with a 5-point Likert scale. They recorded the presence and location of internal knee derangements, including cartilage defects, meniscal tears, tears of ligaments, tendons and muscles, and bone injuries. The statistical analysis included nonparametric Friedman tests, and interreader and intrareader agreement assessment using the weighted Fleiss-Cohen kappa (κ) statistic. P values of less than 0.05 were considered statistically significant.
Results: The evaluated DL-enhanced 4-fold accelerated 2D TSE protocol provided very similar image quality and anatomical visibility to the standard 2D TSE protocol, whereas the 3D SRR Dixon TSE protocol scored less in terms of overall image quality due to reduced edge sharpness and the presence of artifacts ( P < 0.001). Subjective signal-to-noise ratio, contrast resolution, fluid brightness, and fat suppression were good to excellent for all protocols. For 1 reader, the Dixon method of the 3D SRR protocol provided significantly better fat suppression than the spectral fat saturation applied in the standard 2D TSE protocol ( P < 0.05). The visualization of knee structures with 3D SRR Dixon TSE was very similar to the standard protocol, except for cartilage, tendons, and bone, which were affected by the presence of reconstruction and aliasing artifacts ( P < 0.001). The diagnostic confidence of both readers was high for all protocols and all knee structures, except for cartilage and tendons. The standard 2D TSE protocol showed a significantly higher diagnostic confidence for assessing tendons than 3D SRR Dixon TSE MRI ( P < 0.01). The interreader and intrareader agreement for the assessment of internal knee derangements using any of the 3 protocols was substantial to almost perfect (κ = 0.67-1.00). For cartilage, the interreader agreement was substantial for DL-enhanced accelerated 2D TSE (κ = 0.79) and almost perfect for standard 2D TSE (κ = 0.98) and 3D SRR Dixon TSE (κ = 0.87). For menisci, the interreader agreement was substantial for 3D SRR Dixon TSE (κ = 0.70-0.80) and substantial to almost perfect for standard 2D TSE (κ = 0.80-0.99) and DL-enhanced 2D TSE (κ = 0.87-1.00). Moreover, the total acquisition time was reduced by 44% when using the DL-enhanced accelerated 2D TSE or 3D SRR Dixon TSE protocol instead of the conventional 2D TSE protocol.
Conclusions: The presented DL-enhanced 4-fold accelerated 2D TSE protocol provides image quality and diagnostic performance similar to the standard 2D protocol. Moreover, the 3D SRR of DL-enhanced 6-fold accelerated 2D Dixon TSE MRI is feasible for multicontrast 3D knee MRI as its diagnostic performance is comparable to standard 2-fold accelerated 2D knee MRI. However, reconstruction and aliasing artifacts need to be further addressed to guarantee a more reliable visualization and assessment of cartilage, tendons, and bone. Both the 2D and 3D SRR DL-enhanced protocols enable a 44% faster examination compared with conventional 2-fold accelerated routine 2D TSE knee MRI and thus open new paths for more efficient clinical 2D and 3D knee MRI.
期刊介绍:
Investigative Radiology publishes original, peer-reviewed reports on clinical and laboratory investigations in diagnostic imaging, the diagnostic use of radioactive isotopes, computed tomography, positron emission tomography, magnetic resonance imaging, ultrasound, digital subtraction angiography, and related modalities. Emphasis is on early and timely publication. Primarily research-oriented, the journal also includes a wide variety of features of interest to clinical radiologists.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


