Michael J Mello, Janette Baird, Anthony Spirito, Kelli Scott, Mark R Zonfrillo, Lois K Lee, Andrew Kiragu, Emily Christison-Lagay, Julie Bromberg, Stephanie Ruest, Charles Pruitt, Karla A Lawson, Isam W Nasr, Jeremy T Aidlen, Robert Todd Maxson, Sara Becker
{"title":"Adolescents' Perceptions of Screening, Brief Intervention, and Referral to Treatment Service at Pediatric Trauma Centers.","authors":"Michael J Mello, Janette Baird, Anthony Spirito, Kelli Scott, Mark R Zonfrillo, Lois K Lee, Andrew Kiragu, Emily Christison-Lagay, Julie Bromberg, Stephanie Ruest, Charles Pruitt, Karla A Lawson, Isam W Nasr, Jeremy T Aidlen, Robert Todd Maxson, Sara Becker","doi":"10.1177/29768357241272356","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Screening, brief intervention, and referral to treatment (SBIRT) for adolescent alcohol and drug (AOD) use is recommended to occur with adolescents admitted to pediatric trauma centers. Most metrics on SBIRT service delivery only reference medical record documentation. In this analysis we examined changes in adolescents' perception of SBIRT services and concordance of adolescent-report and medical record data, among a sample of adolescents admitted before and after institutional SBIRT implementation.</p><p><strong>Methods: </strong>We implemented SBIRT for adolescent AOD use using the Science to Service Laboratory implementation strategy and enrolled adolescents at 9 pediatric trauma centers. The recommended clinical workflow was for nursing to screen, social work to provide adolescents screening positive with brief intervention and referral to their PCP for continued AOD discussions with those. Adolescents screening as high-risk also referred to specialty services. Adolescents were enrolled and contacted 30 days after discharge and asked about their perception of any SBIRT services received. Data were also extracted from enrolled patient's medical record.</p><p><strong>Results: </strong>There were 430 adolescents enrolled, with 424 that were matched to their EHR data and 329 completed the 30-day survey. In this sample, EHR documented screening increased from pre-implementation to post-implementation (16.3%-65.7%) and brief interventions increased (27.1%-40.7%). Adolescents self-reported higher rates of being asked about alcohol or drug use than in EHR data both pre- and post-implementation (80.7%-81%). Both EHR data and adolescent self-reported data demonstrated low referral back to PCP for continued AOD discussions.</p><p><strong>Conclusions: </strong>Implementation of SBIRT at pediatric trauma centers was not associated with change in adolescent perceptions of SBIRT, despite improved documentation of delivery of AOD screening and interventions. Adolescents perceived being asked about AOD use more often than was documented. Referral to PCP or specialty care for continued AOD discussion remains an area of needed attention.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov NCT03297060.</p>","PeriodicalId":517405,"journal":{"name":"Substance use : research and treatment","volume":"18 ","pages":"29768357241272356"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11339738/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance use : research and treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/29768357241272356","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Screening, brief intervention, and referral to treatment (SBIRT) for adolescent alcohol and drug (AOD) use is recommended to occur with adolescents admitted to pediatric trauma centers. Most metrics on SBIRT service delivery only reference medical record documentation. In this analysis we examined changes in adolescents' perception of SBIRT services and concordance of adolescent-report and medical record data, among a sample of adolescents admitted before and after institutional SBIRT implementation.
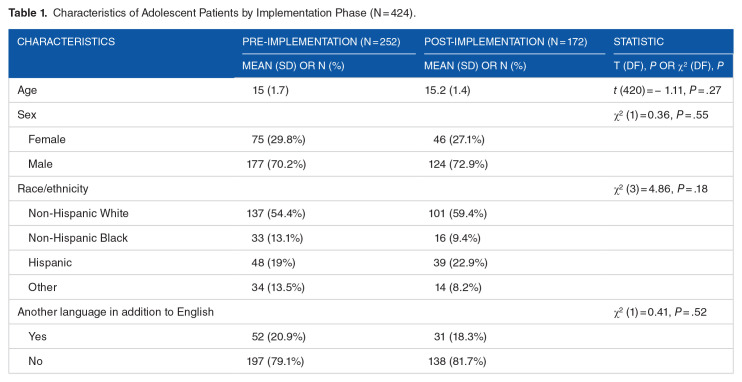
Methods: We implemented SBIRT for adolescent AOD use using the Science to Service Laboratory implementation strategy and enrolled adolescents at 9 pediatric trauma centers. The recommended clinical workflow was for nursing to screen, social work to provide adolescents screening positive with brief intervention and referral to their PCP for continued AOD discussions with those. Adolescents screening as high-risk also referred to specialty services. Adolescents were enrolled and contacted 30 days after discharge and asked about their perception of any SBIRT services received. Data were also extracted from enrolled patient's medical record.
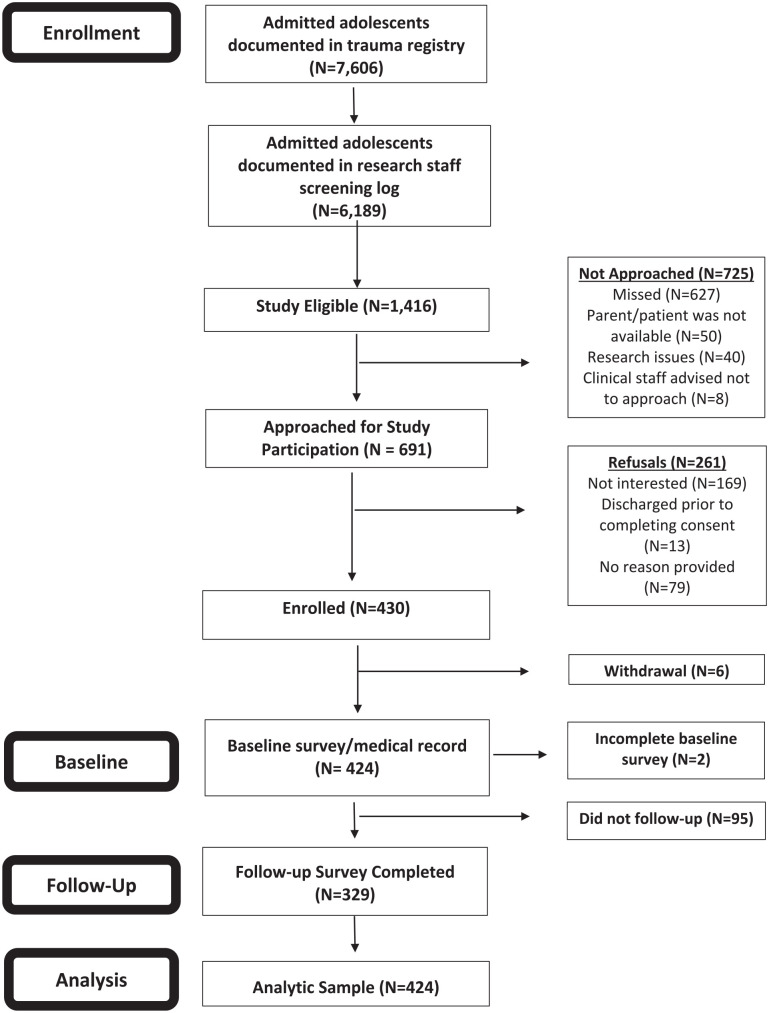
Results: There were 430 adolescents enrolled, with 424 that were matched to their EHR data and 329 completed the 30-day survey. In this sample, EHR documented screening increased from pre-implementation to post-implementation (16.3%-65.7%) and brief interventions increased (27.1%-40.7%). Adolescents self-reported higher rates of being asked about alcohol or drug use than in EHR data both pre- and post-implementation (80.7%-81%). Both EHR data and adolescent self-reported data demonstrated low referral back to PCP for continued AOD discussions.
Conclusions: Implementation of SBIRT at pediatric trauma centers was not associated with change in adolescent perceptions of SBIRT, despite improved documentation of delivery of AOD screening and interventions. Adolescents perceived being asked about AOD use more often than was documented. Referral to PCP or specialty care for continued AOD discussion remains an area of needed attention.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


