{"title":"Robot-assisted, laparoscopic and open radical cystectomy for bladder cancer: A systematic review and network meta-analysis.","authors":"Zhanpo Yang, Xinmeng Dou, Wenhui Zhou, Qian Liu","doi":"10.1590/S1677-5538.IBJU.2024.0191","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the safety and effectiveness of robot-assisted radical cystectomy (RARC), laparoscopic radical cystectomy (LRC), and open radical cystectomy (ORC) in bladder cancer.</p><p><strong>Methods: </strong>A literature search for network meta-analysis was conducted using international databases up to February 29, 2024. Outcomes of interest included baseline characteristics, perioperative outcomes and oncological outcomes.</p><p><strong>Results: </strong>Forty articles were finally selected for inclusion in the network meta-analysis. Both LRC and RARC were associated with longer operative time, smaller amount of estimated blood loss, lower transfusion rate, shorter time to regular diet, fewer incidences of complications, and fewer positive surgical margin compared to ORC. LRC had a shorter time to flatus than ORC, while no difference between RARC and ORC was observed. Considering lymph node yield, there were no differences among LRC, RARC and ORC. In addition, there were statistically significant lower transfusion rates (OR=-0.15, 95% CI=-0.47 to 0.17), fewer overall complication rates (OR=-0.39, 95% CI=-0.79 to 0.00), fewer minor complication rates (OR=-0.23, 95% CI=-0.48 to 0.02), fewer major complication rates (OR=-0.23, 95% CI=-0.68 to 0.21), fewer positive surgical margin rates (OR=0.22, 95% CI=-0.27 to 0.68) in RARC group compared with LRC group.</p><p><strong>Conclusion: </strong>LRC and RARC could be considered as a feasible and safe alternative to ORC for bladder cancer. Notably, compared with LRC, RARC may benefit from significantly lower transfusion rates, fewer complications and lower positive surgical margin rates. These data thus showed that RARC might improve the management of patients with muscle invasive or high-risk non-muscle invasive bladder cancer.</p>","PeriodicalId":49283,"journal":{"name":"International Braz J Urol","volume":"50 ","pages":"683-702"},"PeriodicalIF":4.5000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11554271/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Braz J Urol","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1590/S1677-5538.IBJU.2024.0191","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the safety and effectiveness of robot-assisted radical cystectomy (RARC), laparoscopic radical cystectomy (LRC), and open radical cystectomy (ORC) in bladder cancer.
Methods: A literature search for network meta-analysis was conducted using international databases up to February 29, 2024. Outcomes of interest included baseline characteristics, perioperative outcomes and oncological outcomes.
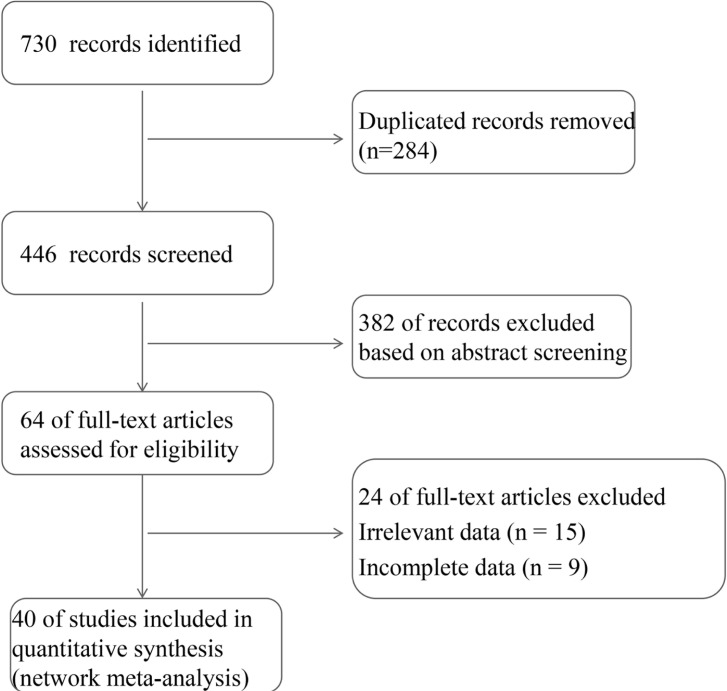
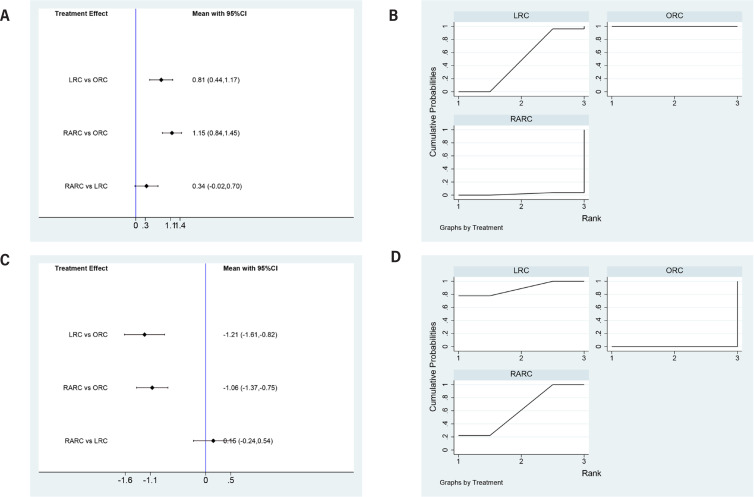
Results: Forty articles were finally selected for inclusion in the network meta-analysis. Both LRC and RARC were associated with longer operative time, smaller amount of estimated blood loss, lower transfusion rate, shorter time to regular diet, fewer incidences of complications, and fewer positive surgical margin compared to ORC. LRC had a shorter time to flatus than ORC, while no difference between RARC and ORC was observed. Considering lymph node yield, there were no differences among LRC, RARC and ORC. In addition, there were statistically significant lower transfusion rates (OR=-0.15, 95% CI=-0.47 to 0.17), fewer overall complication rates (OR=-0.39, 95% CI=-0.79 to 0.00), fewer minor complication rates (OR=-0.23, 95% CI=-0.48 to 0.02), fewer major complication rates (OR=-0.23, 95% CI=-0.68 to 0.21), fewer positive surgical margin rates (OR=0.22, 95% CI=-0.27 to 0.68) in RARC group compared with LRC group.
Conclusion: LRC and RARC could be considered as a feasible and safe alternative to ORC for bladder cancer. Notably, compared with LRC, RARC may benefit from significantly lower transfusion rates, fewer complications and lower positive surgical margin rates. These data thus showed that RARC might improve the management of patients with muscle invasive or high-risk non-muscle invasive bladder cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


