Yanling Jin, Jia Li, Yong Mun, Anthony Masaquel, Sylvia Hu, Juliana M. L. Biondo
{"title":"Association of race/ethnicity and insurance with survival in patients with diffuse large B-cell lymphoma in a large real-world cohort","authors":"Yanling Jin, Jia Li, Yong Mun, Anthony Masaquel, Sylvia Hu, Juliana M. L. Biondo","doi":"10.1002/cam4.70032","DOIUrl":null,"url":null,"abstract":"<p>Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), accounting for approximately 30% of all NHL diagnoses.<span><sup>1</sup></span> DLBCL is a highly heterogenous, aggressive hematological malignancy typically presenting with rapidly enlarging lymphadenopathy and constitutional symptoms, requiring urgent treatment.<span><sup>2</sup></span> More than 18,000 patients are diagnosed with DLBCL each year in the United States (predominantly males), with a 5-year relative survival rate of approximately 64%.<span><sup>3, 4</sup></span></p><p>Although first-line treatment comprising cyclophosphamide, doxorubicin, vincristine and prednisone and the anti-CD20 monoclonal antibody rituximab (R-CHOP) can achieve complete remission for many patients, over one-third of patients with DLBCL do not respond to, or relapse after, R-CHOP.<span><sup>5-7</sup></span> For these patients with refractory or relapsed disease, alternative treatment options including salvage chemotherapy, autologous stem cell transplant or alternative immunotherapeutic approaches are used, but outcomes are often poor.<span><sup>8, 9</sup></span></p><p>Disease stage and treatment are widely acknowledged as key factors affecting health outcomes for cancer patients.<span><sup>10</sup></span> However, in addition to disease stage and treatment, disparities in health outcomes due to race, ethnicity, and socioeconomic status are also documented in the literature, with certain groups at increased risk of developing or succumbing to particular cancers.<span><sup>11</sup></span> An example of this is the documented higher mortality rate for Black patients compared with all other racial/ethnic groups for many, although not all, cancer types.<span><sup>12</sup></span> Furthermore, individuals who live in USA counties that experience persistent poverty are more likely to die from cancer than those who live in more wealthy counties.<span><sup>13</sup></span> Male gender has also been associated with worse survival among patients with DLBCL treated with R-CHOP.<span><sup>14</sup></span></p><p>A small number of studies have specifically addressed socioeconomic disparities, using insurance as a proxy, or racial/ethnic disparities in treatment patterns and health outcomes for patients with DLBCL.<span><sup>15-19</sup></span> Though some of the above studies used large datasets such as the Surveillance, Epidemiology, and End Results (SEER)<span><sup>16, 17</sup></span> and the National Cancer Database (NCDB),<span><sup>15</sup></span> the Flatiron Health database provides an opportunity to study the effect of race and insurance status on cancer survival in a large population of patients with DLBCL in the USA. Flatiron Health includes clinical and outcome data unique among real-world datasets, allowing detailed investigation including sequential time-to-event endpoints.<span><sup>20</sup></span> To our knowledge, no studies have addressed in detail disparities in both health insurance access and race/ethnicity and the relationship with health outcomes for patients with DLBCL based on recent data. Here, we leverage the Flatiron Health database to evaluate the association of race, ethnicity, and health insurance status with treatment outcomes in patients with DLBCL. Based on published findings, we hypothesize that insurance status and race will be significantly linked to poorer survival outcomes in patients with DLBCL.</p><p>In this analysis of data from the Flatiron Health database, which included over 5300 patients with DLBCL treated in the real world, OS was similar among patients of White, Black, Hispanic or Latino, and Asian race after adjusting for baseline characteristics. However, we found that among patients aged <65 years, using Medicaid without access to Commercial insurance was associated with worse OS and a shorter TTNTD when compared with Commercially insured patients.</p><p>In the current study, after adjusting for baseline characteristics, race was not a significant factor associated with survival outcomes in patients with DLBCL. This contradicts the findings of some early studies in the literature, which reported worse survival outcomes in Black patients with DLBCL compared with White patients.<span><sup>17, 22</sup></span> However, recent data from large single-center studies have shown similar survival outcomes in Black patients compared with White patients,<span><sup>19</sup></span> and even improved survival in Hispanic or Latino patients compared with non-Hispanic White patients with DLBCL.<span><sup>18</sup></span> A retrospective analysis by Flowers et al, 2013<span><sup>23</sup></span> suggested that the discrepancy in racial disparity observed between early studies and more recent studies could have arisen from the change in treatment regimen since January 2011, from predominantly using CHOP to R-CHOP. Racial disparity was no longer shown in patients with DLBCL treated with R-CHOP. The Flatiron database only included patients from 2011 onwards and ~ 90% of patients with DLBCL were treated with R-CHOP.</p><p>Our finding that insurance status (Medicaid-insured) was strongly associated with shorter survival outcomes in patients aged <65 years treated for DLBCL is consistent with previously published findings. In a report based on data from the NCDB, patients with DLBCL aged 18–64 years using Medicaid had inferior survival (HR for death, 1.48 [95% CI, 1.23–1.78]) compared with privately insured patients.<span><sup>15</sup></span> Similarly, adjusted data from the SEER database showed that survival estimates for Medicaid-insured patients with DLBCL were statistically significantly lower compared with non-Medicaid-insured patients; 3-year cause-specific survival estimates were 75% for patients with Medicaid and 89% for patients with other insurance.<span><sup>16</sup></span> Patients aged <65 years with Medicaid insurance were diagnosed with more advanced disease (stage III–IV) when compared with patients with commercial insurance (without Medicaid) (65.8% vs. 47.7%; <i>p</i> = 0.005). This difference was not observed in patients aged ≥65 years (<i>p</i> = 0.400). Broadening access to affordable health insurance at an early point in the diagnostic process could reduce the survival disadvantage for patients without adequate coverage.</p><p>In addition to survival, our analysis reported TTNTD (which was lacking in prior work) and found that Medicaid-insured patients aged <65 years had shorter TTNTD when compared with Commercially insured patients (20.0 months vs. 91.8 months, respectively). Both disease-specific (i.e., later stage at diagnosis) and DLBCL-unrelated factors (i.e., unfavorable socioeconomic status and related access barriers) likely contributed to the differences observed according to insurance status.</p><p>Similar to other studies in the literature, our data also show that Black patients with DLBCL, when compared with White patients, were diagnosed at a younger age<span><sup>24</sup></span> and male gender was associated with statistically significantly worse OS and TTNTD.<span><sup>15</sup></span></p><p>Using real-world data has its own uniqueness and strengths. The Flatiron Health database includes comprehensive patient information with long follow up. However, limitations also exist, including missingness of some variables; only around 25% of the insurance data in the Flatiron Health database included both insurance start and end dates (though a missing end date may mean the insurance is valid, without yet reaching its termination date).Another potential limitation was the lack of database information on confounders of survival such as patient comorbidity score and supportive care, preventing their inclusion as covariates in multivariable analyses. Finally, although our cohort was quite large, the number of Medicaid patients was relatively small compared with Commercial patients, suggesting that there is scope for further large-scale studies to be conducted in these populations. While race was not independently associated with long-term DLBCL outcomes, Black patients were much more likely to have Medicaid insurance.</p><p>In conclusion, real-world data from the USA nationwide Flatiron Health database suggest that race is not independently associated with survival outcomes in patients with DLBCL. Instead, insurance status (Medicaid-insured) was significantly associated with shorter survival outcomes among patients aged <65 years but not in those aged ≥65 years. The median OS and TTNTD observed in these real-world data were broadly aligned with previous clinical trials in patients with DLBCL.<span><sup>7</sup></span> Future studies are needed to further evaluate the relationship between race/ethnicity and insurance status and the impact on survival outcomes in patients with DLBCL, and should consider social, environmental, biologic, and patient-related factors that contribute to potential disparities in DLBCL survival.</p><p><b>Yanling Jin:</b> Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). <b>Jia Li:</b> Investigation (equal); writing – review and editing (equal). <b>Yong Mun:</b> Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). <b>Anthony Masaquel:</b> Investigation (equal); writing – review and editing (equal). <b>Sylvia Hu:</b> Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). <b>Juliana M. L. Biondo:</b> Investigation (equal); writing – review and editing (equal).</p><p>This study was sponsored by Genentech, Inc.</p><p>YJ, JL, YM, AM, and JB: current employment, and current equity holder in a publicly traded company (Genentech Inc./F. Hoffmann-La Roche Ltd). SH: previous employment, and previous equity holder in a publicly traded company (F. Hoffmann-La Roche Ltd).</p>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"13 16","pages":""},"PeriodicalIF":3.1000,"publicationDate":"2024-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cam4.70032","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70032","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), accounting for approximately 30% of all NHL diagnoses.1 DLBCL is a highly heterogenous, aggressive hematological malignancy typically presenting with rapidly enlarging lymphadenopathy and constitutional symptoms, requiring urgent treatment.2 More than 18,000 patients are diagnosed with DLBCL each year in the United States (predominantly males), with a 5-year relative survival rate of approximately 64%.3, 4
Although first-line treatment comprising cyclophosphamide, doxorubicin, vincristine and prednisone and the anti-CD20 monoclonal antibody rituximab (R-CHOP) can achieve complete remission for many patients, over one-third of patients with DLBCL do not respond to, or relapse after, R-CHOP.5-7 For these patients with refractory or relapsed disease, alternative treatment options including salvage chemotherapy, autologous stem cell transplant or alternative immunotherapeutic approaches are used, but outcomes are often poor.8, 9
Disease stage and treatment are widely acknowledged as key factors affecting health outcomes for cancer patients.10 However, in addition to disease stage and treatment, disparities in health outcomes due to race, ethnicity, and socioeconomic status are also documented in the literature, with certain groups at increased risk of developing or succumbing to particular cancers.11 An example of this is the documented higher mortality rate for Black patients compared with all other racial/ethnic groups for many, although not all, cancer types.12 Furthermore, individuals who live in USA counties that experience persistent poverty are more likely to die from cancer than those who live in more wealthy counties.13 Male gender has also been associated with worse survival among patients with DLBCL treated with R-CHOP.14
A small number of studies have specifically addressed socioeconomic disparities, using insurance as a proxy, or racial/ethnic disparities in treatment patterns and health outcomes for patients with DLBCL.15-19 Though some of the above studies used large datasets such as the Surveillance, Epidemiology, and End Results (SEER)16, 17 and the National Cancer Database (NCDB),15 the Flatiron Health database provides an opportunity to study the effect of race and insurance status on cancer survival in a large population of patients with DLBCL in the USA. Flatiron Health includes clinical and outcome data unique among real-world datasets, allowing detailed investigation including sequential time-to-event endpoints.20 To our knowledge, no studies have addressed in detail disparities in both health insurance access and race/ethnicity and the relationship with health outcomes for patients with DLBCL based on recent data. Here, we leverage the Flatiron Health database to evaluate the association of race, ethnicity, and health insurance status with treatment outcomes in patients with DLBCL. Based on published findings, we hypothesize that insurance status and race will be significantly linked to poorer survival outcomes in patients with DLBCL.
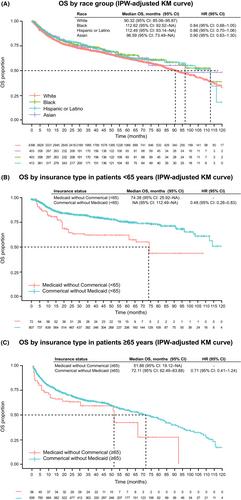
In this analysis of data from the Flatiron Health database, which included over 5300 patients with DLBCL treated in the real world, OS was similar among patients of White, Black, Hispanic or Latino, and Asian race after adjusting for baseline characteristics. However, we found that among patients aged <65 years, using Medicaid without access to Commercial insurance was associated with worse OS and a shorter TTNTD when compared with Commercially insured patients.
In the current study, after adjusting for baseline characteristics, race was not a significant factor associated with survival outcomes in patients with DLBCL. This contradicts the findings of some early studies in the literature, which reported worse survival outcomes in Black patients with DLBCL compared with White patients.17, 22 However, recent data from large single-center studies have shown similar survival outcomes in Black patients compared with White patients,19 and even improved survival in Hispanic or Latino patients compared with non-Hispanic White patients with DLBCL.18 A retrospective analysis by Flowers et al, 201323 suggested that the discrepancy in racial disparity observed between early studies and more recent studies could have arisen from the change in treatment regimen since January 2011, from predominantly using CHOP to R-CHOP. Racial disparity was no longer shown in patients with DLBCL treated with R-CHOP. The Flatiron database only included patients from 2011 onwards and ~ 90% of patients with DLBCL were treated with R-CHOP.
Our finding that insurance status (Medicaid-insured) was strongly associated with shorter survival outcomes in patients aged <65 years treated for DLBCL is consistent with previously published findings. In a report based on data from the NCDB, patients with DLBCL aged 18–64 years using Medicaid had inferior survival (HR for death, 1.48 [95% CI, 1.23–1.78]) compared with privately insured patients.15 Similarly, adjusted data from the SEER database showed that survival estimates for Medicaid-insured patients with DLBCL were statistically significantly lower compared with non-Medicaid-insured patients; 3-year cause-specific survival estimates were 75% for patients with Medicaid and 89% for patients with other insurance.16 Patients aged <65 years with Medicaid insurance were diagnosed with more advanced disease (stage III–IV) when compared with patients with commercial insurance (without Medicaid) (65.8% vs. 47.7%; p = 0.005). This difference was not observed in patients aged ≥65 years (p = 0.400). Broadening access to affordable health insurance at an early point in the diagnostic process could reduce the survival disadvantage for patients without adequate coverage.
In addition to survival, our analysis reported TTNTD (which was lacking in prior work) and found that Medicaid-insured patients aged <65 years had shorter TTNTD when compared with Commercially insured patients (20.0 months vs. 91.8 months, respectively). Both disease-specific (i.e., later stage at diagnosis) and DLBCL-unrelated factors (i.e., unfavorable socioeconomic status and related access barriers) likely contributed to the differences observed according to insurance status.
Similar to other studies in the literature, our data also show that Black patients with DLBCL, when compared with White patients, were diagnosed at a younger age24 and male gender was associated with statistically significantly worse OS and TTNTD.15
Using real-world data has its own uniqueness and strengths. The Flatiron Health database includes comprehensive patient information with long follow up. However, limitations also exist, including missingness of some variables; only around 25% of the insurance data in the Flatiron Health database included both insurance start and end dates (though a missing end date may mean the insurance is valid, without yet reaching its termination date).Another potential limitation was the lack of database information on confounders of survival such as patient comorbidity score and supportive care, preventing their inclusion as covariates in multivariable analyses. Finally, although our cohort was quite large, the number of Medicaid patients was relatively small compared with Commercial patients, suggesting that there is scope for further large-scale studies to be conducted in these populations. While race was not independently associated with long-term DLBCL outcomes, Black patients were much more likely to have Medicaid insurance.
In conclusion, real-world data from the USA nationwide Flatiron Health database suggest that race is not independently associated with survival outcomes in patients with DLBCL. Instead, insurance status (Medicaid-insured) was significantly associated with shorter survival outcomes among patients aged <65 years but not in those aged ≥65 years. The median OS and TTNTD observed in these real-world data were broadly aligned with previous clinical trials in patients with DLBCL.7 Future studies are needed to further evaluate the relationship between race/ethnicity and insurance status and the impact on survival outcomes in patients with DLBCL, and should consider social, environmental, biologic, and patient-related factors that contribute to potential disparities in DLBCL survival.
Yanling Jin: Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). Jia Li: Investigation (equal); writing – review and editing (equal). Yong Mun: Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). Anthony Masaquel: Investigation (equal); writing – review and editing (equal). Sylvia Hu: Conceptualization (equal); data curation (equal); formal analysis (equal); investigation (equal); writing – review and editing (equal). Juliana M. L. Biondo: Investigation (equal); writing – review and editing (equal).
This study was sponsored by Genentech, Inc.
YJ, JL, YM, AM, and JB: current employment, and current equity holder in a publicly traded company (Genentech Inc./F. Hoffmann-La Roche Ltd). SH: previous employment, and previous equity holder in a publicly traded company (F. Hoffmann-La Roche Ltd).
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


