Percutaneous coronary revascularization versus medical therapy in chronic coronary syndromes: An updated meta-analysis of randomized controlled trials
Abstract
Introduction
Coronary artery disease (CAD) is a main cause of morbidity and mortality. The effectiveness of coronary revascularization in chronic coronary syndromes (CCS) is still debated. Our recent study showed the superiority of coronary revascularization over optimal medical therapy (OMT) in reducing cardiovascular (CV) mortality and myocardial infarction (MI). The recent publication of the ORBITA-2 trial suggested superiority of percutaneous coronary revascularization (PCI) in reducing angina and improving quality of life. Therefore, we aimed to provide an updated meta-analysis evaluating the impact of PCI on both clinical outcomes and angina in CCS.
Methods
Relevant studies were screened in PubMed/Medline until 08/01/2024. Randomized controlled trials (RCTs) comparing PCI to OMT in CCS were selected. The primary outcome was CV death. Secondary outcomes were MI, all-cause mortality, stroke, major bleeding and angina severity.
Results
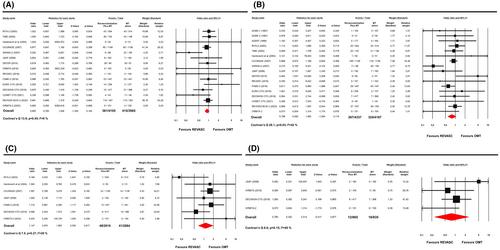
Nineteen RCTs involving 8616 patients were included. Median follow-up duration was 3.3 years. Revascularization significantly reduced CV death (4.2% vs. 5.5%; OR = .77; 95% CI .62–.96, p = .02). Subgroup analyses favoured revascularization in patients without chronic total occlusions (CTOs) (p = .052) and those aged <65 years (p = .02). Finally, a follow-up duration beyond 3 years showed increased benefit of coronary revascularization (p = .04). Secondary outcomes analyses showed no significant differences, except for a lower angina severity in the revascularization group according to the Seattle Angina Questionnaire (SAQ) (p = .04) and to the Canadian Cardiovascular Society (CCS) classification (p = .005).
Conclusions
PCI compared to OMT significantly reduces CV mortality and angina severity, improving quality of life in CCS patients. This benefit was larger without CTOs, in patients aged <65 years and with follow-up duration beyond 3 years.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


