Impact of longitudinal tumor location on postoperative outcomes in gallbladder cancer: Fundus and body vs. neck and cystic duct, a retrospective multicenter study.
Kil Hwan Kim, Ju Ik Moon, Jae Woo Park, Yunghun You, Hae Il Jung, Hanlim Choi, Si Eun Hwang, Sungho Jo
{"title":"Impact of longitudinal tumor location on postoperative outcomes in gallbladder cancer: Fundus and body vs. neck and cystic duct, a retrospective multicenter study.","authors":"Kil Hwan Kim, Ju Ik Moon, Jae Woo Park, Yunghun You, Hae Il Jung, Hanlim Choi, Si Eun Hwang, Sungho Jo","doi":"10.14701/ahbps.24-117","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds/aims: </strong>Systematic investigations into the prognostic impact of the longitudinal tumor location in gallbladder cancer (GBC) remain insufficient. To address the limitations of our pilot study, we conducted a multicenter investigation to clarify the impact of the longitudinal tumor location on the oncological outcomes of GBC.</p><p><strong>Methods: </strong>A retrospective multicenter study was conducted on 372 patients undergoing radical resections for GBC from January 2010 to December 2019 across seven hospitals that belong to the Daejeon-Chungcheong branch of the Korean Association of Hepato-Biliary-Pancreatic Surgery. Patients were divided into GBC in the fundus/body (FB-GBC) and GBC in the neck/cystic duct (NC-GBC) groups, based on the longitudinal tumor location.</p><p><strong>Results: </strong>Of 372 patients, 282 had FB-GBC, while 90 had NC-GBC. NC-GBC was associated with more frequent elevation of preoperative carbohydrate antigen (CA) 19-9 levels, requirement for more extensive surgery, more advanced histologic grade and tumor stages, more frequent lymphovascular and perineural invasion, lower R0 resection rates, higher recurrence rates, and worse 5-year overall and disease-free survival rates. Propensity score matching analysis confirmed these findings, showing lower R0 resection rates, higher recurrence rates, and worse survival rates in the NC-GBC group. Multivariate analysis identified elevated preoperative CA 19-9 levels, lymph node metastasis, and non-R0 resection as independent prognostic factors, but not longitudinal tumor location.</p><p><strong>Conclusions: </strong>NC-GBC exhibits more frequent elevation of preoperative CA 19-9 levels, more advanced histologic grade and tumor stages, lower R0 resection rates, and poorer overall and disease-free survival rates, compared to FB-GBC. However, the longitudinal tumor location was not analyzed as an independent prognostic factor.</p>","PeriodicalId":72220,"journal":{"name":"Annals of hepato-biliary-pancreatic surgery","volume":" ","pages":"474-482"},"PeriodicalIF":1.7000,"publicationDate":"2024-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11599822/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of hepato-biliary-pancreatic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14701/ahbps.24-117","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/20 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Backgrounds/aims: Systematic investigations into the prognostic impact of the longitudinal tumor location in gallbladder cancer (GBC) remain insufficient. To address the limitations of our pilot study, we conducted a multicenter investigation to clarify the impact of the longitudinal tumor location on the oncological outcomes of GBC.
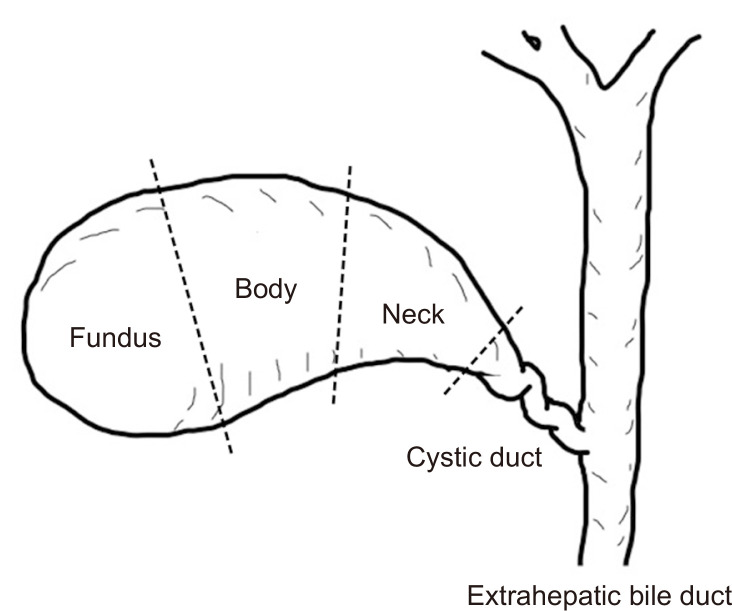
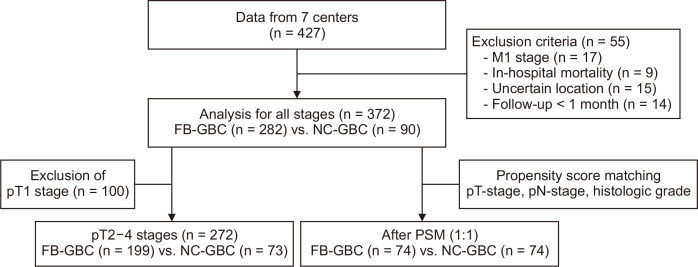
Methods: A retrospective multicenter study was conducted on 372 patients undergoing radical resections for GBC from January 2010 to December 2019 across seven hospitals that belong to the Daejeon-Chungcheong branch of the Korean Association of Hepato-Biliary-Pancreatic Surgery. Patients were divided into GBC in the fundus/body (FB-GBC) and GBC in the neck/cystic duct (NC-GBC) groups, based on the longitudinal tumor location.
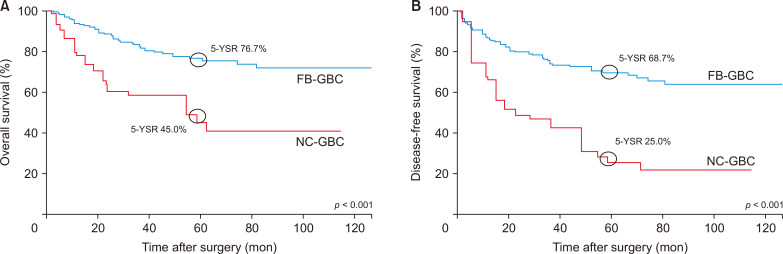
Results: Of 372 patients, 282 had FB-GBC, while 90 had NC-GBC. NC-GBC was associated with more frequent elevation of preoperative carbohydrate antigen (CA) 19-9 levels, requirement for more extensive surgery, more advanced histologic grade and tumor stages, more frequent lymphovascular and perineural invasion, lower R0 resection rates, higher recurrence rates, and worse 5-year overall and disease-free survival rates. Propensity score matching analysis confirmed these findings, showing lower R0 resection rates, higher recurrence rates, and worse survival rates in the NC-GBC group. Multivariate analysis identified elevated preoperative CA 19-9 levels, lymph node metastasis, and non-R0 resection as independent prognostic factors, but not longitudinal tumor location.
Conclusions: NC-GBC exhibits more frequent elevation of preoperative CA 19-9 levels, more advanced histologic grade and tumor stages, lower R0 resection rates, and poorer overall and disease-free survival rates, compared to FB-GBC. However, the longitudinal tumor location was not analyzed as an independent prognostic factor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


