{"title":"Acquired Hemophilia A Diagnosed Based on Gross Hematuria: A Case Report and Literature Review.","authors":"Kenichi Hata, Junichiro Kato, Yusuke Takahashi, Shun Saito, Keigo Sakanaka, Takahiro Kimura","doi":"10.1155/2024/2760153","DOIUrl":null,"url":null,"abstract":"<p><p>Acquired hemophilia A (AHA) is an acquired bleeding disorder caused by neutralizing antibodies (inhibitors) against Coagulation Factor VIII (FVIII:C), causing sudden hemorrhagic symptoms (i.e., subcutaneous bleeding, intramuscular bleeding, and hematuria). Herein, this study is aimed at presenting a case of AHA diagnosed based on hematuria and reviewing patients who were diagnosed with AHA due to hematuria. A 67-year-old woman was referred to Atsugi City Hospital with painless gross hematuria that began 4 weeks before presentation. Contrast-enhanced computed tomography (eCT) revealed an approximately 2 cm mass in the right renal pelvis, and the patient's activated partial thromboplastin time (APTT) was elevated (61.4 s). The day after the endoscopic biopsy, the patient was in shock due to a large retroperitoneal hematoma. Although her condition stabilized after intravenous radioembolization, she underwent emergency surgeries several times because of rebleeding within the next 3 weeks. At that time, APTT was more prolonged at 106.4 s, and the FVIII:C level was 2%. Mixing tests showed an upwardly convex curve after 2-h incubation, indicating the presence of an inhibitor. Factor VIII inhibitor titer was ≥5.1 Bethesda unit (BU)/mL. A combined product of Plasma-Derived Factors VIIa and X (pd-FVIIa/FX), as second-line hemostatic therapy, as well as cyclophosphamide (CYP), were administered after Recombinant Activated Factor VIIa (rFVIIa) had been ineffective. Following this, the Factor VIII inhibitor titer was undetectable, FVIII:C levels were restored, and APTT decreased to within the normal range. Gross hematuria was significantly alleviated. However, the patient died of cytomegalovirus and fungal infections due to prolonged immunosuppressive therapy. Although AHA diagnosed based on hematuria may have a better prognosis than others, there have been occasional cases with severe outcomes. APTT, detected upon initial hematological testing in patients with hematuria, may be a potential indicator of an existing AHA.</p>","PeriodicalId":30323,"journal":{"name":"Case Reports in Urology","volume":"2024 ","pages":"2760153"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11333134/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/2760153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
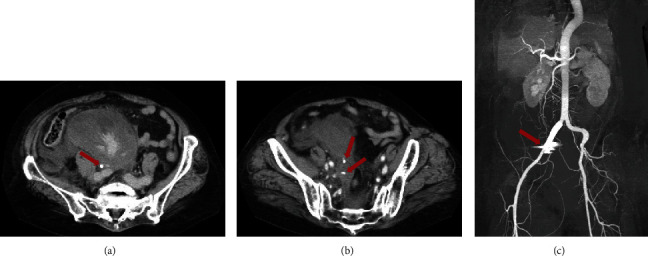
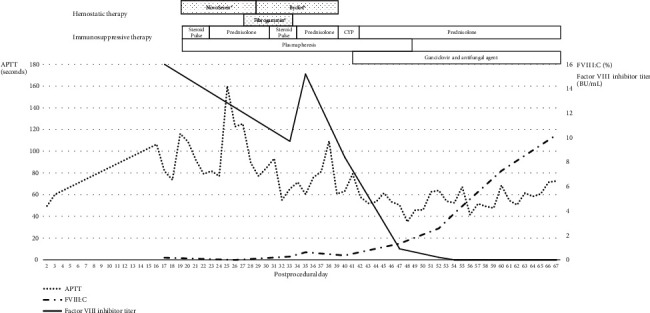
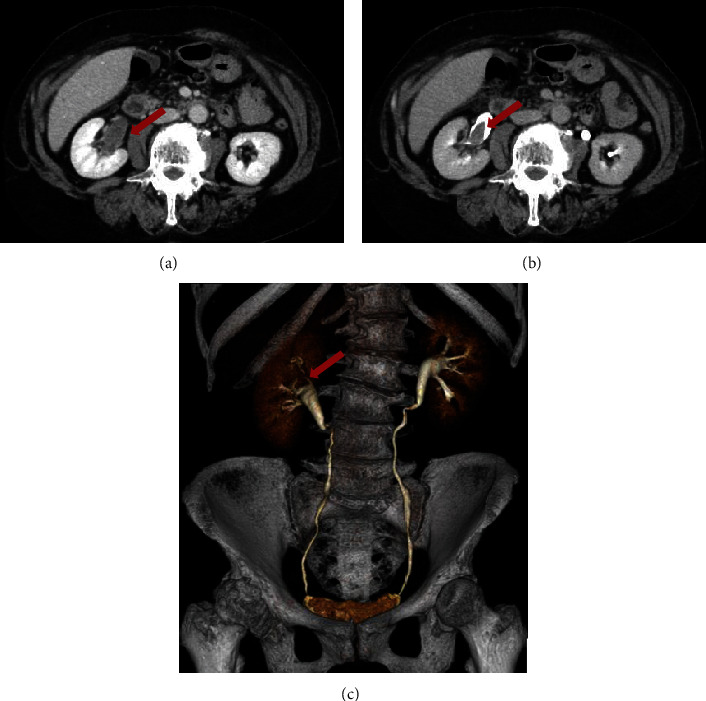
Acquired hemophilia A (AHA) is an acquired bleeding disorder caused by neutralizing antibodies (inhibitors) against Coagulation Factor VIII (FVIII:C), causing sudden hemorrhagic symptoms (i.e., subcutaneous bleeding, intramuscular bleeding, and hematuria). Herein, this study is aimed at presenting a case of AHA diagnosed based on hematuria and reviewing patients who were diagnosed with AHA due to hematuria. A 67-year-old woman was referred to Atsugi City Hospital with painless gross hematuria that began 4 weeks before presentation. Contrast-enhanced computed tomography (eCT) revealed an approximately 2 cm mass in the right renal pelvis, and the patient's activated partial thromboplastin time (APTT) was elevated (61.4 s). The day after the endoscopic biopsy, the patient was in shock due to a large retroperitoneal hematoma. Although her condition stabilized after intravenous radioembolization, she underwent emergency surgeries several times because of rebleeding within the next 3 weeks. At that time, APTT was more prolonged at 106.4 s, and the FVIII:C level was 2%. Mixing tests showed an upwardly convex curve after 2-h incubation, indicating the presence of an inhibitor. Factor VIII inhibitor titer was ≥5.1 Bethesda unit (BU)/mL. A combined product of Plasma-Derived Factors VIIa and X (pd-FVIIa/FX), as second-line hemostatic therapy, as well as cyclophosphamide (CYP), were administered after Recombinant Activated Factor VIIa (rFVIIa) had been ineffective. Following this, the Factor VIII inhibitor titer was undetectable, FVIII:C levels were restored, and APTT decreased to within the normal range. Gross hematuria was significantly alleviated. However, the patient died of cytomegalovirus and fungal infections due to prolonged immunosuppressive therapy. Although AHA diagnosed based on hematuria may have a better prognosis than others, there have been occasional cases with severe outcomes. APTT, detected upon initial hematological testing in patients with hematuria, may be a potential indicator of an existing AHA.
获得性血友病 A(AHA)是一种获得性出血性疾病,由凝血因子 VIII(FVIII:C)的中和抗体(抑制剂)引起,导致突发性出血症状(即皮下出血、肌肉出血和血尿)。本研究旨在介绍一例因血尿而被诊断为 AHA 的病例,并回顾因血尿而被诊断为 AHA 的患者。一名 67 岁的女性因无痛性毛细血尿于就诊前 4 周开始出现,被转诊至厚木市立医院。造影增强计算机断层扫描(eCT)显示右肾盂有一个约 2 厘米的肿块,患者的活化部分凝血活酶时间(APTT)升高(61.4 秒)。内镜活检后第二天,患者因腹膜后巨大血肿而休克。虽然在静脉放射栓塞术后病情趋于稳定,但在接下来的三周内,她因再次出血而多次接受急诊手术。当时,APTT 延长至 106.4 秒,FVIII:C 水平为 2%。混合试验显示,培养 2 小时后曲线向上凸起,表明存在抑制剂。因子 VIII 抑制剂滴度≥5.1 贝塞斯达单位(BU)/毫升。在重组活化因子 VIIa(rFVIIa)无效后,作为二线止血疗法的血浆衍生因子 VIIa 和 X 的联合产品(pd-FVIIa/FX)以及环磷酰胺(CYP)被使用。此后,检测不到因子 VIII 抑制剂滴度,FVIII:C 水平得到恢复,APTT 下降到正常范围内。血尿症状明显减轻。然而,由于长期接受免疫抑制治疗,患者死于巨细胞病毒和真菌感染。虽然根据血尿确诊的 AHA 患者预后可能比其他患者好,但偶尔也会出现严重后果的病例。在对血尿患者进行初步血液学检测时发现的 APTT 可能是现有 AHA 的一个潜在指标。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


