Richard Crawley, Sina Amirrajab, Didier Lustermans, Robert J Holtackers, Sven Plein, Mitko Veta, Marcel Breeuwer, Amedeo Chiribiri, Cian M Scannell
{"title":"Automated cardiovascular MR myocardial scar quantification with unsupervised domain adaptation.","authors":"Richard Crawley, Sina Amirrajab, Didier Lustermans, Robert J Holtackers, Sven Plein, Mitko Veta, Marcel Breeuwer, Amedeo Chiribiri, Cian M Scannell","doi":"10.1186/s41747-024-00497-3","DOIUrl":null,"url":null,"abstract":"<p><p>Quantification of myocardial scar from late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) images can be facilitated by automated artificial intelligence (AI)-based analysis. However, AI models are susceptible to domain shifts in which the model performance is degraded when applied to data with different characteristics than the original training data. In this study, CycleGAN models were trained to translate local hospital data to the appearance of a public LGE CMR dataset. After domain adaptation, an AI scar quantification pipeline including myocardium segmentation, scar segmentation, and computation of scar burden, previously developed on the public dataset, was evaluated on an external test set including 44 patients clinically assessed for ischemic scar. The mean ± standard deviation Dice similarity coefficients between the manual and AI-predicted segmentations in all patients were similar to those previously reported: 0.76 ± 0.05 for myocardium and 0.75 ± 0.32 for scar, 0.41 ± 0.12 for scar in scans with pathological findings. Bland-Altman analysis showed a mean bias in scar burden percentage of -0.62% with limits of agreement from -8.4% to 7.17%. These results show the feasibility of deploying AI models, trained with public data, for LGE CMR quantification on local clinical data using unsupervised CycleGAN-based domain adaptation. RELEVANCE STATEMENT: Our study demonstrated the possibility of using AI models trained from public databases to be applied to patient data acquired at a specific institution with different acquisition settings, without additional manual labor to obtain further training labels.</p>","PeriodicalId":36926,"journal":{"name":"European Radiology Experimental","volume":"8 1","pages":"93"},"PeriodicalIF":3.7000,"publicationDate":"2024-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11324636/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Radiology Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41747-024-00497-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
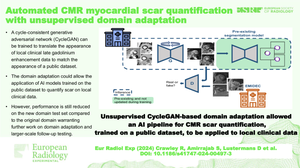
Quantification of myocardial scar from late gadolinium enhancement (LGE) cardiovascular magnetic resonance (CMR) images can be facilitated by automated artificial intelligence (AI)-based analysis. However, AI models are susceptible to domain shifts in which the model performance is degraded when applied to data with different characteristics than the original training data. In this study, CycleGAN models were trained to translate local hospital data to the appearance of a public LGE CMR dataset. After domain adaptation, an AI scar quantification pipeline including myocardium segmentation, scar segmentation, and computation of scar burden, previously developed on the public dataset, was evaluated on an external test set including 44 patients clinically assessed for ischemic scar. The mean ± standard deviation Dice similarity coefficients between the manual and AI-predicted segmentations in all patients were similar to those previously reported: 0.76 ± 0.05 for myocardium and 0.75 ± 0.32 for scar, 0.41 ± 0.12 for scar in scans with pathological findings. Bland-Altman analysis showed a mean bias in scar burden percentage of -0.62% with limits of agreement from -8.4% to 7.17%. These results show the feasibility of deploying AI models, trained with public data, for LGE CMR quantification on local clinical data using unsupervised CycleGAN-based domain adaptation. RELEVANCE STATEMENT: Our study demonstrated the possibility of using AI models trained from public databases to be applied to patient data acquired at a specific institution with different acquisition settings, without additional manual labor to obtain further training labels.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


