Joon Sung Kim, Byung-Wook Kim, Jin Il Kim, Woo Chul Chung, Sung Woo Jung, Chang Seok Bang, Gwang Ha Kim, Seon Woo Jeon, Moon Kyoung Joo, Si Hyung Lee, Yun Jeong Lim, Jae Kyu Sung, Seung Young Seo, Sun Young Park, Wan Sik Lee, Hang Lak Lee, Ki Bae Kim, Heung Up Kim
{"title":"Empirical Therapy Versus Tailored Therapy of Helicobacter pylori in Korea: Results of the K-CREATE Study","authors":"Joon Sung Kim, Byung-Wook Kim, Jin Il Kim, Woo Chul Chung, Sung Woo Jung, Chang Seok Bang, Gwang Ha Kim, Seon Woo Jeon, Moon Kyoung Joo, Si Hyung Lee, Yun Jeong Lim, Jae Kyu Sung, Seung Young Seo, Sun Young Park, Wan Sik Lee, Hang Lak Lee, Ki Bae Kim, Heung Up Kim","doi":"10.1111/hel.13126","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The optimal duration of regimens for tailored therapy based on genotypic resistance for clarithromycin has yet to be established.</p>\n </section>\n \n <section>\n \n <h3> Aim</h3>\n \n <p>This study was a nationwide, multicenter, randomized trial comparing empirical therapy with tailored therapy based on genotypic resistance for first-line eradication of <i>Helicobacter pylori</i>. We also compared the eradication rates of 7- and 14-day regimens for each group.</p>\n </section>\n \n <section>\n \n <h3> Patients and Methods</h3>\n \n <p>Patients with <i>H. pylori</i> infection were first randomized to receive empirical or tailored therapy. Patients in each group were further randomized into 7- or 14-day regimens. Empirical therapy consisted of a triple therapy (TT) regimen (twice-daily doses of pantoprazole 40 mg, amoxicillin 1 g, and clarithromycin 500 mg) for 7 or 14 days. Tailored therapy consisted of TT of 7 or 14 days in patients without genotypic resistance. Patients with genotypic resistance were treated with bismuth quadruple therapy (BQT) regimens (twice-daily doses of pantoprazole 40 mg, three daily doses of metronidazole 500 mg, and four times daily doses of bismuth 300 mg and tetracycline 500 mg) for 7 or 14 days. A <sup>13</sup>C-urea breath test assessed eradication rates. The primary outcome was eradication rates of each group.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>A total of 593 patients were included in the study. The eradication rates were 65.7% (201/306) in the empirical therapy group and 81.9% (235/287) in the tailored therapy group for intention-to-treat analysis (<i>p</i> < 0.001). In the per-protocol analysis, the eradication rates of the empirical therapy and tailored groups were 70.3% (201/286) and 85.5% (235/274) (<i>p</i> < 0.001), respectively. There was no difference in compliance between the two groups. The rate of adverse events was higher in the tailored group compared to the empirical group (<i>p</i> < 0.001).</p>\n </section>\n \n <section>\n \n <h3> Discussion</h3>\n \n <p>Our study confirmed that tailored therapy based on genotypic resistance was more effective than empirical therapy for <i>H. pylori</i> eradication in Korea. However, no significant difference was found between 7- and 14-day regimens for each group. Future studies are needed to determine the optimal duration of therapy for empirical and tailored therapy regimens.</p>\n </section>\n </div>","PeriodicalId":13223,"journal":{"name":"Helicobacter","volume":"29 4","pages":""},"PeriodicalIF":4.3000,"publicationDate":"2024-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/hel.13126","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Helicobacter","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/hel.13126","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background
The optimal duration of regimens for tailored therapy based on genotypic resistance for clarithromycin has yet to be established.
Aim
This study was a nationwide, multicenter, randomized trial comparing empirical therapy with tailored therapy based on genotypic resistance for first-line eradication of Helicobacter pylori. We also compared the eradication rates of 7- and 14-day regimens for each group.
Patients and Methods
Patients with H. pylori infection were first randomized to receive empirical or tailored therapy. Patients in each group were further randomized into 7- or 14-day regimens. Empirical therapy consisted of a triple therapy (TT) regimen (twice-daily doses of pantoprazole 40 mg, amoxicillin 1 g, and clarithromycin 500 mg) for 7 or 14 days. Tailored therapy consisted of TT of 7 or 14 days in patients without genotypic resistance. Patients with genotypic resistance were treated with bismuth quadruple therapy (BQT) regimens (twice-daily doses of pantoprazole 40 mg, three daily doses of metronidazole 500 mg, and four times daily doses of bismuth 300 mg and tetracycline 500 mg) for 7 or 14 days. A 13C-urea breath test assessed eradication rates. The primary outcome was eradication rates of each group.
Results
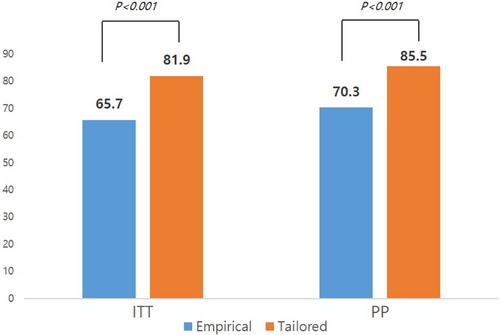
A total of 593 patients were included in the study. The eradication rates were 65.7% (201/306) in the empirical therapy group and 81.9% (235/287) in the tailored therapy group for intention-to-treat analysis (p < 0.001). In the per-protocol analysis, the eradication rates of the empirical therapy and tailored groups were 70.3% (201/286) and 85.5% (235/274) (p < 0.001), respectively. There was no difference in compliance between the two groups. The rate of adverse events was higher in the tailored group compared to the empirical group (p < 0.001).
Discussion
Our study confirmed that tailored therapy based on genotypic resistance was more effective than empirical therapy for H. pylori eradication in Korea. However, no significant difference was found between 7- and 14-day regimens for each group. Future studies are needed to determine the optimal duration of therapy for empirical and tailored therapy regimens.
期刊介绍:
Helicobacter is edited by Professor David Y Graham. The editorial and peer review process is an independent process. Whenever there is a conflict of interest, the editor and editorial board will declare their interests and affiliations. Helicobacter recognises the critical role that has been established for Helicobacter pylori in peptic ulcer, gastric adenocarcinoma, and primary gastric lymphoma. As new helicobacter species are now regularly being discovered, Helicobacter covers the entire range of helicobacter research, increasing communication among the fields of gastroenterology; microbiology; vaccine development; laboratory animal science.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


