{"title":"Quantitative Anatomical Study of the Supratentorial and Infratentorial “Endoscopic Keyhole” Approach to the Peripineal Region","authors":"Hao Wu, Aierpati Maimaiti, Qiang Xie, Yirizhati Aili, Mamutijiang Muertizha, Guohua Zhu, Maimaitili Mijiti, Yandong Li, Yongxin Wang","doi":"10.1155/2024/6851468","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Background</i>. The pineal region represents significant challenges in terms of neurosurgery. Currently, anatomical research that simulates surgery for the endoscopic keyhole approach to the pineal region is lacking. This study aims to summarize the exposure range and operational characteristics of total endoscopic surgery under the four supratentorial and infratentorial keyhole approaches, through rigorous quantitative anatomical research. We also aim to understand the surgical exposure characteristics and surgical feasibility under each approach. <i>Method</i>. Six wet cadaveric head specimens (a total of 12 sides) were subjected to simulated surgery with a keyhole bone window size of approximately 3 × 4 cm. The median endoscopic supracerebellar infratentorial approach (M-ESCITA), the paramedian endoscopic supracerebellar infratentorial approach (PM-ESCITA), the endoscopic occipital transtentorial approach (EOTA), and the endoscopic interhemispheric high occipital transtentorial approach (EHOTA) were used to measure the surgical path depth, maximum distance between the tentorial margins, maximum operable area, operable angle, and relative degree of freedom of each approach. <i>Results</i>. There was no difference in the exposure range of the surgical area. The surgical path of PM-ESCITA was the longest (<i>p</i> < 0.001), and its horizontal operating angle was the largest (<i>p</i> < 0.001), whereas the anteroposterior operating angle of EHOTA was the largest (<i>p</i> < 0.001). The maximum operational area of M-ESCITA was the largest in the pineal region (<i>p</i> < 0.01), whereas that of EHOTA was the largest in the tetrapod region (<i>p</i> < 0.001). M-ESCITA had the highest relative degree of freedom during surgery at the pineal gland level (<i>p</i> < 0.001), PM-ESCITA at the splenium of the corpus callosum (<i>p</i> < 0.01), and EHOTA at the corpora quadrigemina (<i>p</i> < 0.001). <i>Conclusions</i>. Each of the four endoscopic keyhole approaches has its own advantages. Through anatomical research, doctors can train themselves and master the differences in surgical procedures through different approaches. The choice of approach and surgical challenge are dependent on the microsurgical techniques employed by the surgeon. A balance between minimally invasive and safe endoscopic surgery should be pursued.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.2000,"publicationDate":"2024-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/6851468","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/6851468","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
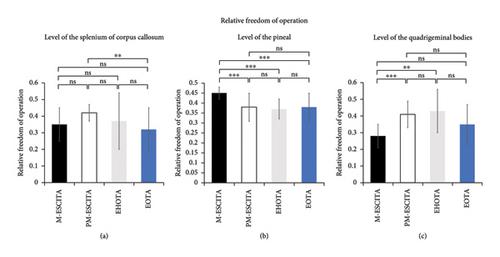
Background. The pineal region represents significant challenges in terms of neurosurgery. Currently, anatomical research that simulates surgery for the endoscopic keyhole approach to the pineal region is lacking. This study aims to summarize the exposure range and operational characteristics of total endoscopic surgery under the four supratentorial and infratentorial keyhole approaches, through rigorous quantitative anatomical research. We also aim to understand the surgical exposure characteristics and surgical feasibility under each approach. Method. Six wet cadaveric head specimens (a total of 12 sides) were subjected to simulated surgery with a keyhole bone window size of approximately 3 × 4 cm. The median endoscopic supracerebellar infratentorial approach (M-ESCITA), the paramedian endoscopic supracerebellar infratentorial approach (PM-ESCITA), the endoscopic occipital transtentorial approach (EOTA), and the endoscopic interhemispheric high occipital transtentorial approach (EHOTA) were used to measure the surgical path depth, maximum distance between the tentorial margins, maximum operable area, operable angle, and relative degree of freedom of each approach. Results. There was no difference in the exposure range of the surgical area. The surgical path of PM-ESCITA was the longest (p < 0.001), and its horizontal operating angle was the largest (p < 0.001), whereas the anteroposterior operating angle of EHOTA was the largest (p < 0.001). The maximum operational area of M-ESCITA was the largest in the pineal region (p < 0.01), whereas that of EHOTA was the largest in the tetrapod region (p < 0.001). M-ESCITA had the highest relative degree of freedom during surgery at the pineal gland level (p < 0.001), PM-ESCITA at the splenium of the corpus callosum (p < 0.01), and EHOTA at the corpora quadrigemina (p < 0.001). Conclusions. Each of the four endoscopic keyhole approaches has its own advantages. Through anatomical research, doctors can train themselves and master the differences in surgical procedures through different approaches. The choice of approach and surgical challenge are dependent on the microsurgical techniques employed by the surgeon. A balance between minimally invasive and safe endoscopic surgery should be pursued.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


