{"title":"Impacto en la morbilidad neonatal del retraso de crecimiento intrauterino precoz moderado-grave definido por criterios doppler: estudio multicéntrico","authors":"Jesús Alberto Fuentes Carballal , Marcelino Pumarada Prieto , Pilar Adelaida Crespo Suárez , José Luaces González , Isabel López Conde , Rosaura Picans Leis , Alicia Sardina Ríos , Cristina Durán Fernández-Feijoo , Alejandro Avila-Alvarez","doi":"10.1016/j.anpedi.2024.05.010","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>In recent years, there has been a change in the conceptualization of fetal growth restriction (FGR), which has gone from being defined solely based on weight criteria to being defined and staged based on Doppler criteria. The aim of our study was to evaluate neonatal risk in a cohort of neonates with moderate to severe early-onset FGR defined by Doppler criteria.</p></div><div><h3>Population and methods</h3><p>We conducted a multicentre prospective cohort study in a cohort of neonates with early-onset fetal growth restriction and abnormal Doppler findings, and a control cohort without Doppler abnormalities matched for sex and gestational age.</p></div><div><h3>Results</h3><p>A total of 105 patients (50 cases, 55 controls) were included. We found a higher frequency of respiratory morbidity in the FGR group, with an increased need of surfactant (30 vs. 27.3%; OR 5.3 [95% CI 1.1-26.7]), an increased need for supplemental oxygen (66 vs. 49.1%; OR 5.6 [95% CI 1.5-20.5]), and a decreased survival without bronchopulmonary dysplasia (70 vs. 87.3%; OR 0.16 [95% CI 0.03-0.99]). Patients with FGR required a longer length of stay and more days of parenteral nutrition and had a higher incidence of haematological abnormalities such as neutropenia and thrombopenia. The lactate level at birth was higher in the severe FGR subgroup (6.12 vs. 2.4<!--> <!-->mg/dL; <em>P</em> <!-->=<!--> <!-->.02).</p></div><div><h3>Conclusions</h3><p>The diagnosis of early-onset moderate to severe FGR defined by Doppler criteria carries a greater risk of respiratory, nutritional and haematological morbidity, independently of weight and gestational age. These patients, therefore, should be considered at increased risk compared to constitutionally small for gestational age preterm infants or preterm infants without FGR.</p></div>","PeriodicalId":7783,"journal":{"name":"Anales de pediatria","volume":"101 2","pages":"Pages 104-114"},"PeriodicalIF":1.5000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S1695403324001097/pdfft?md5=4ed9b2b65e52234f6aa2833a0c354ad0&pid=1-s2.0-S1695403324001097-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anales de pediatria","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1695403324001097","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
In recent years, there has been a change in the conceptualization of fetal growth restriction (FGR), which has gone from being defined solely based on weight criteria to being defined and staged based on Doppler criteria. The aim of our study was to evaluate neonatal risk in a cohort of neonates with moderate to severe early-onset FGR defined by Doppler criteria.
Population and methods
We conducted a multicentre prospective cohort study in a cohort of neonates with early-onset fetal growth restriction and abnormal Doppler findings, and a control cohort without Doppler abnormalities matched for sex and gestational age.
Results
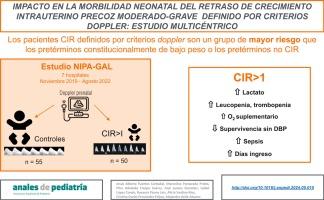
A total of 105 patients (50 cases, 55 controls) were included. We found a higher frequency of respiratory morbidity in the FGR group, with an increased need of surfactant (30 vs. 27.3%; OR 5.3 [95% CI 1.1-26.7]), an increased need for supplemental oxygen (66 vs. 49.1%; OR 5.6 [95% CI 1.5-20.5]), and a decreased survival without bronchopulmonary dysplasia (70 vs. 87.3%; OR 0.16 [95% CI 0.03-0.99]). Patients with FGR required a longer length of stay and more days of parenteral nutrition and had a higher incidence of haematological abnormalities such as neutropenia and thrombopenia. The lactate level at birth was higher in the severe FGR subgroup (6.12 vs. 2.4 mg/dL; P = .02).
Conclusions
The diagnosis of early-onset moderate to severe FGR defined by Doppler criteria carries a greater risk of respiratory, nutritional and haematological morbidity, independently of weight and gestational age. These patients, therefore, should be considered at increased risk compared to constitutionally small for gestational age preterm infants or preterm infants without FGR.
导言近年来,胎儿生长受限(FGR)的概念发生了变化,从单纯根据体重标准定义到根据多普勒标准定义和分期。我们的研究旨在评估根据多普勒标准定义的中度至重度早发型胎儿生长受限新生儿队列中的新生儿风险。研究对象和方法 我们对早发型胎儿生长受限且多普勒结果异常的新生儿队列以及性别和胎龄匹配的无多普勒异常的对照队列进行了一项多中心前瞻性队列研究。我们发现 FGR 组呼吸系统发病率较高,需要使用表面活性物质的比例增加(30 vs. 27.3%;OR 5.3 [95% CI 1.1-26.7]),需要补充氧气的比例增加(66 vs. 49.1%;OR 5.6 [95% CI 1.5-20.5]),无支气管肺发育不良的存活率降低(70 vs. 87.3%;OR 0.16 [95% CI 0.03-0.99])。FGR患者需要更长的住院时间和更多的肠外营养天数,中性粒细胞减少症和血栓性血小板减少症等血液学异常的发生率也更高。结论:根据多普勒标准诊断出的早发中度至重度FGR,其呼吸、营养和血液病发病风险更高,与体重和胎龄无关。因此,与胎龄小的早产儿或无FGR的早产儿相比,这些患者的风险应被视为更高。
期刊介绍:
La Asociación Española de Pediatría tiene como uno de sus objetivos principales la difusión de información científica rigurosa y actualizada sobre las distintas áreas de la pediatría. Anales de Pediatría es el Órgano de Expresión Científica de la Asociación y constituye el vehículo a través del cual se comunican los asociados. Publica trabajos originales sobre investigación clínica en pediatría procedentes de España y países latinoamericanos, así como artículos de revisión elaborados por los mejores profesionales de cada especialidad, las comunicaciones del congreso anual y los libros de actas de la Asociación, y guías de actuación elaboradas por las diferentes Sociedades/Secciones Especializadas integradas en la Asociación Española de Pediatría.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


