Assessment of right ventricular systolic function using speckle tracking strain imaging in patients with severe tricuspid regurgitation: a validation study with cardiac magnetic resonance.
Inki Moon, Soongu Kwak, MinKwan Kim, Seung-Pyo Lee, Hyung-Kwan Kim, Yong-Jin Kim, Jun-Bean Park
{"title":"Assessment of right ventricular systolic function using speckle tracking strain imaging in patients with severe tricuspid regurgitation: a validation study with cardiac magnetic resonance.","authors":"Inki Moon, Soongu Kwak, MinKwan Kim, Seung-Pyo Lee, Hyung-Kwan Kim, Yong-Jin Kim, Jun-Bean Park","doi":"10.1186/s44348-024-00015-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Right ventricular (RV) systolic dysfunction is an established prognostic factor in patients with severe tricuspid regurgitation (TR). However, accurate assessment of RV systolic function using conventional echocardiography remains challenging. We investigated the accuracy of strain measurement using speckle tracking echocardiography (STE) for evaluating RV systolic function in patients with severe TR.</p><p><strong>Methods: </strong>We included consecutive patients with severe TR who underwent echocardiography and cardiac magnetic resonance imaging (CMR) within 30 days between 2011 and 2023. Two-dimensional STE was used to measure RV free wall longitudinal strain (RVFWLS) and global longitudinal strain (RVGLS). These values were compared with the RV ejection fraction (RVEF) from CMR. RV systolic dysfunction was defined as a CMR-derived RVEF < 35%.</p><p><strong>Results: </strong>A total of 87 patients with severe TR were identified during the study period. Among echocardiographic RV strain measurements, RVFWLS was the best correlate of CMR-derived RVEF (r = -0.37, P < 0.001), followed by RVGLS (r = -0.27, P = 0.012). Receiver operating characteristic (ROC) curve analysis revealed that RVFWLS provided better discrimination of RV systolic dysfunction, yielding an area under the ROC curve (AUC) of 0.770 (95% confidence interval [CI], 0.696-0.800) than RV fractional area change (AUC, 0.615; 95% CI, 0.500-0.859).</p><p><strong>Conclusions: </strong>In patients with severe TR, STE-derived RVFWLS showed the best correlation with RVEF on CMR and displayed superior discrimination of RV systolic dysfunction compared with the RV fractional area change. This study suggests the potential usefulness of STE in assessing RV systolic function in this population.</p>","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"32 1","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11304584/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44348-024-00015-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Right ventricular (RV) systolic dysfunction is an established prognostic factor in patients with severe tricuspid regurgitation (TR). However, accurate assessment of RV systolic function using conventional echocardiography remains challenging. We investigated the accuracy of strain measurement using speckle tracking echocardiography (STE) for evaluating RV systolic function in patients with severe TR.
Methods: We included consecutive patients with severe TR who underwent echocardiography and cardiac magnetic resonance imaging (CMR) within 30 days between 2011 and 2023. Two-dimensional STE was used to measure RV free wall longitudinal strain (RVFWLS) and global longitudinal strain (RVGLS). These values were compared with the RV ejection fraction (RVEF) from CMR. RV systolic dysfunction was defined as a CMR-derived RVEF < 35%.
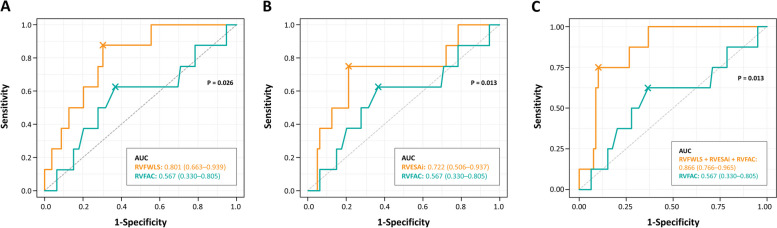
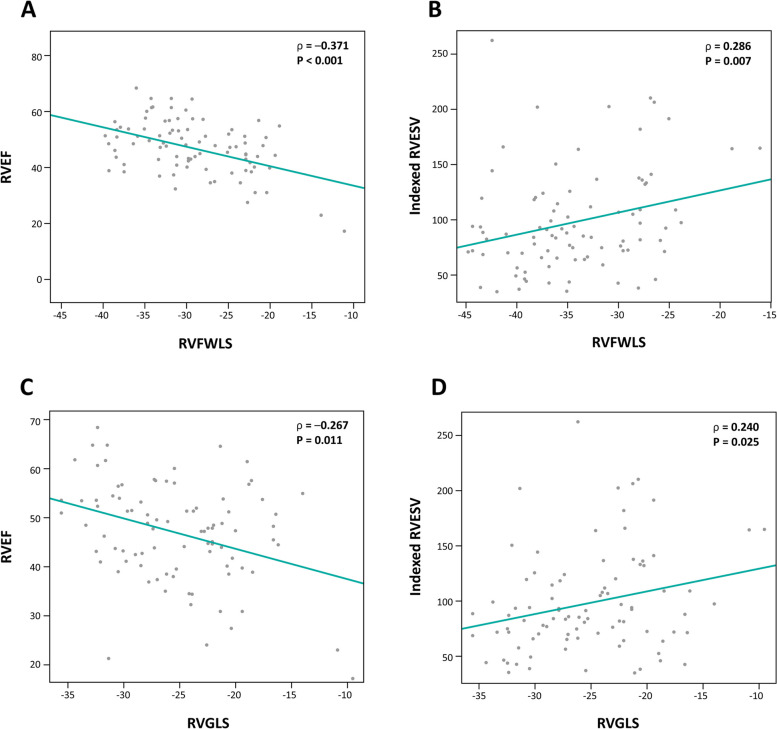
Results: A total of 87 patients with severe TR were identified during the study period. Among echocardiographic RV strain measurements, RVFWLS was the best correlate of CMR-derived RVEF (r = -0.37, P < 0.001), followed by RVGLS (r = -0.27, P = 0.012). Receiver operating characteristic (ROC) curve analysis revealed that RVFWLS provided better discrimination of RV systolic dysfunction, yielding an area under the ROC curve (AUC) of 0.770 (95% confidence interval [CI], 0.696-0.800) than RV fractional area change (AUC, 0.615; 95% CI, 0.500-0.859).
Conclusions: In patients with severe TR, STE-derived RVFWLS showed the best correlation with RVEF on CMR and displayed superior discrimination of RV systolic dysfunction compared with the RV fractional area change. This study suggests the potential usefulness of STE in assessing RV systolic function in this population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


