Lars Brodowski, Maria Knoth, Leonie Zehner, Ulrich Pecks
{"title":"Assessing Severity and Need for Delivery in Early Onset Preeclampsia Before 32 Weeks of Gestation: a Delphi Consensus Procedure.","authors":"Lars Brodowski, Maria Knoth, Leonie Zehner, Ulrich Pecks","doi":"10.1055/a-2361-0563","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preeclampsia is a potentially life-threatening hypertensive pregnancy disorder that carries an acute risk of an unfavorable outcome of the pregnancy but also has consequences for the long-term health of the mother. Women who develop the early form of pre-eclampsia before the 32nd week of pregnancy have the highest risk and are also the most difficult to treat. The severity of pre-eclampsia is not characterized uniformly in Germany, so that the indication for delivery is rather individualized. The aim of this study was to reach a consensus on parameters that could serve as criteria for describing the severity of pre-eclampsia based on the urgency of delivery. To this end, a Delphi procedure was used to present a scenario in which a woman was admitted for preeclampsia before 32 gestational weeks and after completion of antenatal steroid therapy.</p><p><strong>Methods: </strong>Clinicians specialized in maternal-fetal medicine from German-speaking countries completed five rounds of a modified Delphi questionnaire. Presented parameters were selected by the section \"Hypertensive Pregnancy Diseases and Fetal Growth Restriction\" of the German Society of Gynecology and Obstetrics after reviewing the literature. These included objectifiable laboratory or clinical parameters as well as subjective symptoms of the patient. In addition, nine fetal parameters were taken into account. The clinicians were asked to rate presented parameters as an indication for delivery on a Likert scale from 0 to 4 (no indication to absolute indication without delay). For each item, the predefined cut-off for group consensus was ≥ 70% agreement.</p><p><strong>Results: </strong>A total of 126 experts were approached. Sixty-nine experts (54.8%) took part in the first round; of those 50 completed the entire Delphi procedure. A consensus was reached on 14 parameters to be considered rapid preparation for delivery without delay (4 points on the Likert scale). These were among others hepatic hematoma or liver capsule rupture, acute liver failure with fulminant coagulation disorder or disseminated intravascular coagulation, eclampsia, pathologic findings in imaging (e.g. cMRI) or electrocardiogram arranged for new onset of headache or retrosternal pain, respectively. Twenty-six parameters were rated as factors that should be considered in the decision without being absolute (1 to 3 points), and 13 parameters should have no influence on the decision to deliver (0 points). No consensus on severe hypertension as an indication for delivery could be reached for blood pressure values below 220/140 mmHg.</p><p><strong>Conclusion: </strong>A consensus was reached on whether to deliver in preeclampsia typic clinical findings and symptoms. The results can serve as guidance for current clinical practice and for the definition of clinical endpoints in intervention studies. Nevertheless, the isolated criteria are a theoretical construction since the combined deterioration or summation of several factors rather than a single factor most likely influences the decision to deliver and reflect the severity of preeclampsia. Moreover, the degree of hypertension as an indication for delivery remains controversial, unless the patient suffers additionally from complaints. Future research should be enforced to incorporate long-term risks for the mother into a decision aid.</p>","PeriodicalId":12481,"journal":{"name":"Geburtshilfe Und Frauenheilkunde","volume":"84 8","pages":"760-772"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11303012/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geburtshilfe Und Frauenheilkunde","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2361-0563","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Preeclampsia is a potentially life-threatening hypertensive pregnancy disorder that carries an acute risk of an unfavorable outcome of the pregnancy but also has consequences for the long-term health of the mother. Women who develop the early form of pre-eclampsia before the 32nd week of pregnancy have the highest risk and are also the most difficult to treat. The severity of pre-eclampsia is not characterized uniformly in Germany, so that the indication for delivery is rather individualized. The aim of this study was to reach a consensus on parameters that could serve as criteria for describing the severity of pre-eclampsia based on the urgency of delivery. To this end, a Delphi procedure was used to present a scenario in which a woman was admitted for preeclampsia before 32 gestational weeks and after completion of antenatal steroid therapy.
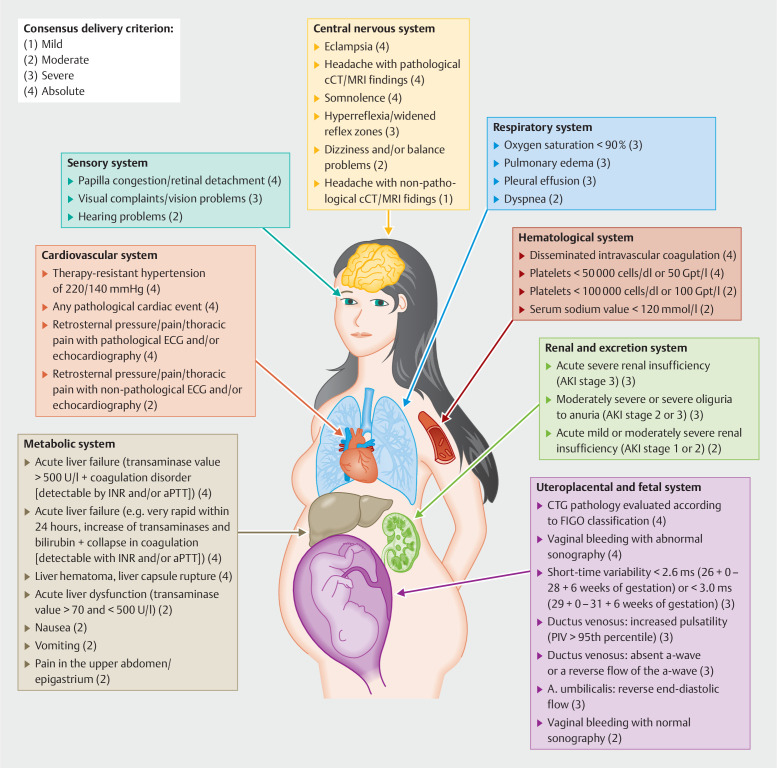
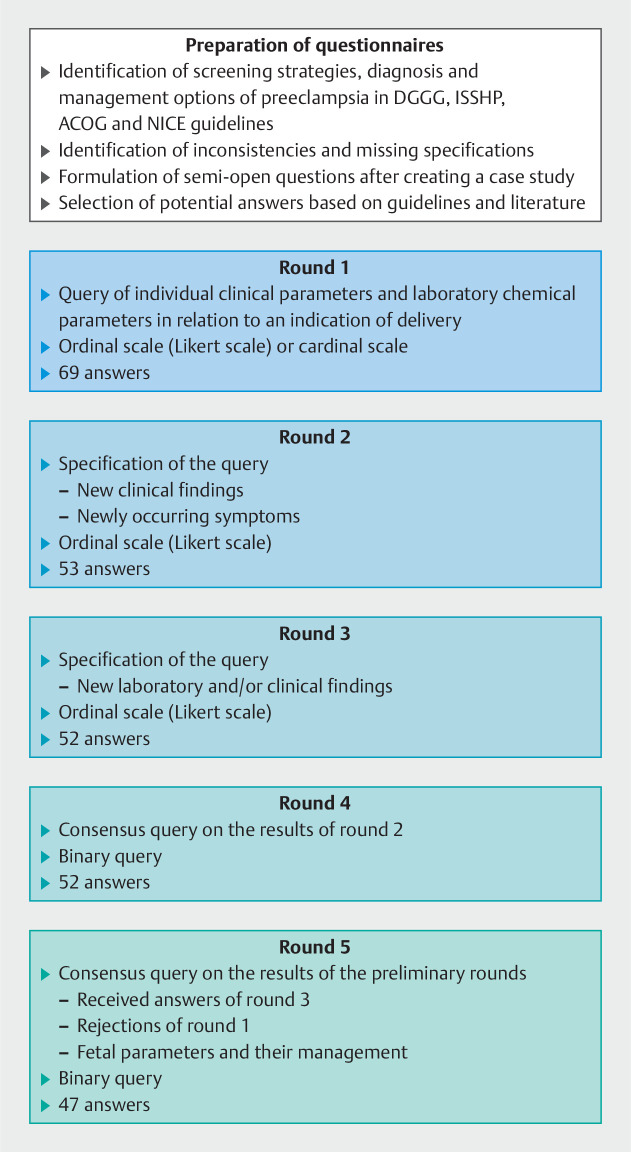
Methods: Clinicians specialized in maternal-fetal medicine from German-speaking countries completed five rounds of a modified Delphi questionnaire. Presented parameters were selected by the section "Hypertensive Pregnancy Diseases and Fetal Growth Restriction" of the German Society of Gynecology and Obstetrics after reviewing the literature. These included objectifiable laboratory or clinical parameters as well as subjective symptoms of the patient. In addition, nine fetal parameters were taken into account. The clinicians were asked to rate presented parameters as an indication for delivery on a Likert scale from 0 to 4 (no indication to absolute indication without delay). For each item, the predefined cut-off for group consensus was ≥ 70% agreement.
Results: A total of 126 experts were approached. Sixty-nine experts (54.8%) took part in the first round; of those 50 completed the entire Delphi procedure. A consensus was reached on 14 parameters to be considered rapid preparation for delivery without delay (4 points on the Likert scale). These were among others hepatic hematoma or liver capsule rupture, acute liver failure with fulminant coagulation disorder or disseminated intravascular coagulation, eclampsia, pathologic findings in imaging (e.g. cMRI) or electrocardiogram arranged for new onset of headache or retrosternal pain, respectively. Twenty-six parameters were rated as factors that should be considered in the decision without being absolute (1 to 3 points), and 13 parameters should have no influence on the decision to deliver (0 points). No consensus on severe hypertension as an indication for delivery could be reached for blood pressure values below 220/140 mmHg.
Conclusion: A consensus was reached on whether to deliver in preeclampsia typic clinical findings and symptoms. The results can serve as guidance for current clinical practice and for the definition of clinical endpoints in intervention studies. Nevertheless, the isolated criteria are a theoretical construction since the combined deterioration or summation of several factors rather than a single factor most likely influences the decision to deliver and reflect the severity of preeclampsia. Moreover, the degree of hypertension as an indication for delivery remains controversial, unless the patient suffers additionally from complaints. Future research should be enforced to incorporate long-term risks for the mother into a decision aid.
期刊介绍:
Geburtshilfe und Frauenheilkunde (GebFra) addresses the whole field of obstetrics and gynecology and is concerned with research as much as with clinical practice. In its scientific section, it publishes original articles, reviews and case reports in all fields of the discipline, namely
gynecological oncology, including oncology of the breast
obstetrics and perinatal medicine,
reproductive medicine,
and urogynecology.
GebFra invites the submission of original articles and review articles.
In addition, the journal publishes guidelines, statements and recommendations in cooperation with the DGGG, SGGG, OEGGG and the Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF, Association of Scientific Medical Societies, www.awmf.org). Apart from the scientific section, Geburtshilfe und Frauenheilkunde has a news and views section that also includes discussions, book reviews and professional information.
Letters to the editors are welcome. If a letter discusses an article that has been published in our journal, the corresponding author of the article will be informed and invited to comment on the letter. The comment will be published along with the letter.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


