{"title":"Duodenitis associated with ulcerative colitis and pouchitis after total colectomy successfully treated with upadacitinib: A case report","authors":"Kentaro Kojima*, Jun Takada, Kiichi Otani, Naoya Masuda, Yukari Tezuka, Sachiyo Onishi, Masaya Kubota, Takashi Ibuka, Masahito Shimizu","doi":"10.1002/deo2.415","DOIUrl":null,"url":null,"abstract":"<p>A 27-year-old man had ulcerative colitis (UC) 1 year prior and underwent a colectomy and two-stage ileal pouch-anal anastomosis for medically refractory UC 6 months ago. He visited our department with epigastric pain and discomfort, increased stool frequency, and bloody diarrhea. Esophagogastroduodenoscopy revealed continuous diffuse friable mucosa, erosions, and edema in the duodenum, and pouchoscopy revealed multiple ulcers and purulent mucus adhesions. Based on endoscopic and pathological findings, the patient was diagnosed with duodenitis associated with UC and pouchitis, for which he received oral prednisolone (40 mg/day) and ciprofloxacin. The frequency of stools and occurrence of bloody diarrhea reduced, and epigastric pain and discomfort improved after 2 weeks. However, when prednisolone was discontinued, the symptoms worsened, albumin level decreased, and C-reactive protein level increased. Following this, we administered a 20 mg prednisolone sodium phosphate enema once daily, and the patient's symptoms improved. However, the symptoms relapsed when the enema was discontinued. Assuming that the patient had steroid-dependent duodenitis associated with UC and pouchitis, we initiated upadacitinib. His symptoms improved within a few days, and biomarkers returned to normal after 1 month. Nine months after initiating the upadacitinib treatment, endoscopic remission was achieved in the mucosa of the duodenum and pouch. The patient has been in clinical remission for 1 year without any adverse events.</p>","PeriodicalId":93973,"journal":{"name":"DEN open","volume":"5 1","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2024-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11300533/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"DEN open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/deo2.415","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
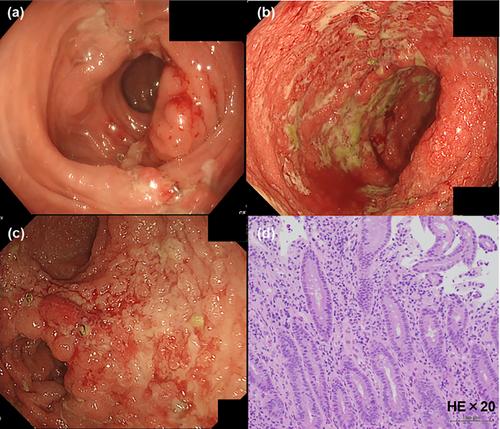
A 27-year-old man had ulcerative colitis (UC) 1 year prior and underwent a colectomy and two-stage ileal pouch-anal anastomosis for medically refractory UC 6 months ago. He visited our department with epigastric pain and discomfort, increased stool frequency, and bloody diarrhea. Esophagogastroduodenoscopy revealed continuous diffuse friable mucosa, erosions, and edema in the duodenum, and pouchoscopy revealed multiple ulcers and purulent mucus adhesions. Based on endoscopic and pathological findings, the patient was diagnosed with duodenitis associated with UC and pouchitis, for which he received oral prednisolone (40 mg/day) and ciprofloxacin. The frequency of stools and occurrence of bloody diarrhea reduced, and epigastric pain and discomfort improved after 2 weeks. However, when prednisolone was discontinued, the symptoms worsened, albumin level decreased, and C-reactive protein level increased. Following this, we administered a 20 mg prednisolone sodium phosphate enema once daily, and the patient's symptoms improved. However, the symptoms relapsed when the enema was discontinued. Assuming that the patient had steroid-dependent duodenitis associated with UC and pouchitis, we initiated upadacitinib. His symptoms improved within a few days, and biomarkers returned to normal after 1 month. Nine months after initiating the upadacitinib treatment, endoscopic remission was achieved in the mucosa of the duodenum and pouch. The patient has been in clinical remission for 1 year without any adverse events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


