Kaushik Ravipati, Inamullah Khan, Wesley Chen, Ravi Nunna, Aaron Voshage, Sasidhar Karuparti, Ismail Ziu, Michael Ortiz
{"title":"Factors associated with radiographic progression and neurologic decline in patients with isolated traumatic subarachnoid hemorrhage.","authors":"Kaushik Ravipati, Inamullah Khan, Wesley Chen, Ravi Nunna, Aaron Voshage, Sasidhar Karuparti, Ismail Ziu, Michael Ortiz","doi":"10.1186/s41016-024-00377-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Complicated mild traumatic brain injury (cmTBI) is a common neurosurgical disorder that consumes a significant amount of healthcare resources without a clearly established benefit. Best practices for the management of cmTBI regarding triage, hospital admission, and the necessity for repeat imaging are controversial. Our objective is to describe the rate of radiographic progression and neurologic decline for isolated traumatic subarachnoid hemorrhage (itSAH) patients admitted to the hospital. We hypothesized that only a minority of itSAH patients suffer radiographic progression and that radiographic progression is not necessarily associated with neurologic decline.</p><p><strong>Methods: </strong>Database queries and direct patient chart reviews were used to gather patient data. T-tests and Fisher's exact tests were performed.</p><p><strong>Results: </strong>A total of 340 patients with cmTBI associated with itSAH were included for analysis. The radiographic progression rate was 5.6%. There was no statistically significant association between age, gender, GCS at presentation, anticoagulation status, and risk of radiographic progression. However, subgroup analysis on anticoagulated patients did show those on warfarin had a statistically significant risk of radiographic progression (p = 0.003). No patient developed neurologic decline, irrespective of whether they developed radiographic progression.</p><p><strong>Conclusion: </strong>Secondary triaging, hospital admission, ICU stay, and repeat HCT might not be necessary for awake, GCS 13-15 patients with itSAH without any other significant injuries. In the case of anticoagulant use, but not necessarily antiplatelet use, the medication should be reversed, and admission should be considered.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":"10 1","pages":"25"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11302199/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-024-00377-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Complicated mild traumatic brain injury (cmTBI) is a common neurosurgical disorder that consumes a significant amount of healthcare resources without a clearly established benefit. Best practices for the management of cmTBI regarding triage, hospital admission, and the necessity for repeat imaging are controversial. Our objective is to describe the rate of radiographic progression and neurologic decline for isolated traumatic subarachnoid hemorrhage (itSAH) patients admitted to the hospital. We hypothesized that only a minority of itSAH patients suffer radiographic progression and that radiographic progression is not necessarily associated with neurologic decline.
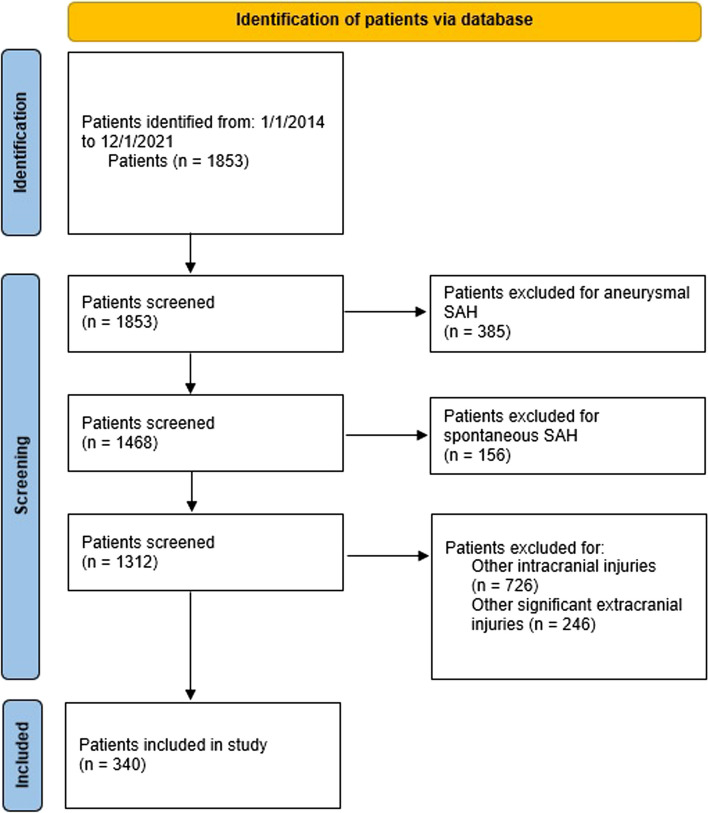
Methods: Database queries and direct patient chart reviews were used to gather patient data. T-tests and Fisher's exact tests were performed.
Results: A total of 340 patients with cmTBI associated with itSAH were included for analysis. The radiographic progression rate was 5.6%. There was no statistically significant association between age, gender, GCS at presentation, anticoagulation status, and risk of radiographic progression. However, subgroup analysis on anticoagulated patients did show those on warfarin had a statistically significant risk of radiographic progression (p = 0.003). No patient developed neurologic decline, irrespective of whether they developed radiographic progression.
Conclusion: Secondary triaging, hospital admission, ICU stay, and repeat HCT might not be necessary for awake, GCS 13-15 patients with itSAH without any other significant injuries. In the case of anticoagulant use, but not necessarily antiplatelet use, the medication should be reversed, and admission should be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


