Felicity Norris, Amrit Dhesi, Shifa Shaikh, Andrew T. Clark, Gary Stiefel
{"title":"BSACI Nut Allergy Guideline Audit by National Survey: A Summary of Findings","authors":"Felicity Norris, Amrit Dhesi, Shifa Shaikh, Andrew T. Clark, Gary Stiefel","doi":"10.1111/cea.14549","DOIUrl":null,"url":null,"abstract":"<p>Since the publication of the BSACI guideline on the management of nut allergy (NA) in 2017 [<span>1</span>], little is known regarding current practice across the United Kingdom (UK). Between 07 December 2022 and 03 February 2023, an online survey was disseminated through the BSACI and local allergy networks to BSACI members and non-members. Respondents completed a survey (available via link below) covering resources and case vignettes to assess approaches to diagnosis and management of NA. Aims of the survey included to audit compliance with the published diagnostic pathways, and to establish current dietary and medical management. Finally, we assessed regional differences in service provision and management of NA.</p><p>A total of 249 healthcare professionals (HCPs) responded to the survey. Of respondents, 190 (76%) were BSACI members and 59 (24%) were non-members. The response rate amongst BSACI members was 19% (190/979). 219/249 (88%) of respondents exclusively managed paediatric patients; 105/190 (55%) of the BSACI members were paediatric allergists/paediatricians with allergy interest.</p><p>Amongst respondents from the different UK regions, at least 92% had access to skin prick testing (SPT), 95% to specific IgE (sIgE) testing and 93% to written allergy plans. Overall, ≥99% respondents had access to a dietitian via a referral process except in the North (<i>referring to Health Education England's</i> North East and North West regions). There was a large observed disparity in access to a dietitian in clinic; 74% in London compared to 35% in the North. Only respondents from 3 NHS trusts (Ireland, Wales and London) reported psychologist access in clinic.</p><p>Diagnostic accuracy to three case vignettes was determined by correct interpretation and application of the published diagnostic algorithm [<span>1</span>]. Only BSACI member responses were audited (<i>n</i> = 190). Responses resulting in diagnostic accuracy for primary peanut allergy (PA) were 140/149 (94%) and 142/148 (96%) for pollen food syndrome (PFS). Despite typical histories of PA and PFS, 43/149 (29%) and 105/148 (71%), respectively, suggested component resolved diagnostics (CRD), which are not recommended. Only 89/146 (61%) suggested CRD for a case of PFS/primary hazelnut allergy (diagnostic uncertainty), although the algorithm supports its use.</p><p>Medical and dietary management was evaluated in BSACI members (<i>n</i> = 190). Prescribing AAIs for cases of anaphylaxis to peanut (147/149 (99%)) and PFS with no asthma (17/153 (11%)) were consistent across respondents. In example cases 1, 3 & 4 (Figure 1) there was large variation with 98/154 (64%), 82/154 (53%) and 94/154 (61%), respectively, recommending AAIs. Over 90% of respondents in all regions except the Midlands & East (62%) would advise patients to carry two AAIs at all times in a case of anaphylaxis to peanut.</p><p>Dietary advice for avoidance of the index nut was consistent using a case of PA and tree NA at 97%. 118–120/155 (76%–77%) recommended additional tree nut avoidance if sensitised unless tolerated and consumed regularly, 47–49/155 (30%–32%) advised to consume foods with nut precautionary allergen labelling (PAL), while 50–52/155 (32%–34%) suggested the contrary.</p><p>The provision of SPT or sIgE testing, written allergy plans and medication are generally standardised across the UK. However, this survey provides further evidence that there is significant regional variation in provision of allied HCPs (dietitians and psychology support) particularly with regards to being present in clinic as part of a multidisciplinary team [<span>2</span>]. This may result in delays for families in receiving appropriate advice and, additional appointments, which have financial implications particularly for low-income families [<span>3</span>].</p><p>Diagnosis of NA relies on an allergy-focused history and SPT/sIgE, which is consistent with the BSACI NA guideline although there appears to be increasing use of CRDs, which should be reserved for cases of diagnostic uncertainty. This practice is unlikely to have been influenced by the BSACI PFS guideline published in 2022 as CRDs are only recommended in cases of uncertainty on primary tree nut/legume allergy or cases of possible primary tree nut/legume allergy and PFS [<span>4</span>]. However, the ‘EAACI Molecular Allergology User Guide 2.0’ in the case of diagnosis to peanut allergy suggests peanut specific IgE and Ara h 2 component as first-line investigations with a clear history [<span>5</span>]. It would be useful to determine further consensus on when CRD should be used as it has the potential of further increasing healthcare costs.</p><p>AAI prescribing practices are consistent in cases of clear anaphylaxis to peanut or PFS with no asthma. However, there is more variation in practice in other cases such as primary NA without anaphylaxis or PFS and asthma as well as regional variations (Repository information is available at https://osf.io/dvm3z/?view_only=ed289c3a6c3d4aa9ab3a5190c8f282d2). Both the BSACI and EAACI (European Academy of Allergy and Clinical Immunology) provide guidance but allow for lots of variation in practice in these grey areas [<span>6, 7</span>]. Continued education and dissemination of the guideline would enable greater consistency. Furthermore, research in identifying high-risk phenotypes in the grey cases would enable greater consensus amongst HCPs on AAI prescribing.</p><p>Variation also exists relating to dietary advice regarding avoidance of other nuts apart from the index nut and, on PAL. This does not seem to be influenced by dietetic service provision. Further consensus amongst HCPs in addition to the ongoing work by industry and the Food Standards Agency may result in a more consistent approach for patients.</p><p>We recognise that there was a low survey response rate; however, this is consistent with previous BSACI surveys. It illustrates an important snapshot of the current state of NA diagnosis and management and better dissemination of guidance may improve adherence. However, further work is required if the allergy community wish to provide a consistent message to patients in relation to dietetic and AAI provision.</p><p>G.S., A.D., A.T.C. and S.S. were involved in initial creation of audit questionnaire and execution of the project. F.N. collated and evaluated the data and all authors contributed to the writing and revision of the article.</p><p>Dr. Gary Stiefel is principal investigator on the NATASHA study looking at Peanut and milk desensitisation and is a trustee for Allergy UK. Dr. Andrew Clark is Chief Medical Officer and stockholder in Camallergy Ltd.</p>","PeriodicalId":10207,"journal":{"name":"Clinical and Experimental Allergy","volume":"54 11","pages":"936-938"},"PeriodicalIF":6.3000,"publicationDate":"2024-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/cea.14549","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Allergy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cea.14549","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Since the publication of the BSACI guideline on the management of nut allergy (NA) in 2017 [1], little is known regarding current practice across the United Kingdom (UK). Between 07 December 2022 and 03 February 2023, an online survey was disseminated through the BSACI and local allergy networks to BSACI members and non-members. Respondents completed a survey (available via link below) covering resources and case vignettes to assess approaches to diagnosis and management of NA. Aims of the survey included to audit compliance with the published diagnostic pathways, and to establish current dietary and medical management. Finally, we assessed regional differences in service provision and management of NA.
A total of 249 healthcare professionals (HCPs) responded to the survey. Of respondents, 190 (76%) were BSACI members and 59 (24%) were non-members. The response rate amongst BSACI members was 19% (190/979). 219/249 (88%) of respondents exclusively managed paediatric patients; 105/190 (55%) of the BSACI members were paediatric allergists/paediatricians with allergy interest.
Amongst respondents from the different UK regions, at least 92% had access to skin prick testing (SPT), 95% to specific IgE (sIgE) testing and 93% to written allergy plans. Overall, ≥99% respondents had access to a dietitian via a referral process except in the North (referring to Health Education England's North East and North West regions). There was a large observed disparity in access to a dietitian in clinic; 74% in London compared to 35% in the North. Only respondents from 3 NHS trusts (Ireland, Wales and London) reported psychologist access in clinic.
Diagnostic accuracy to three case vignettes was determined by correct interpretation and application of the published diagnostic algorithm [1]. Only BSACI member responses were audited (n = 190). Responses resulting in diagnostic accuracy for primary peanut allergy (PA) were 140/149 (94%) and 142/148 (96%) for pollen food syndrome (PFS). Despite typical histories of PA and PFS, 43/149 (29%) and 105/148 (71%), respectively, suggested component resolved diagnostics (CRD), which are not recommended. Only 89/146 (61%) suggested CRD for a case of PFS/primary hazelnut allergy (diagnostic uncertainty), although the algorithm supports its use.
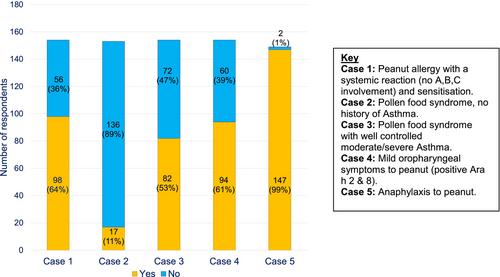
Medical and dietary management was evaluated in BSACI members (n = 190). Prescribing AAIs for cases of anaphylaxis to peanut (147/149 (99%)) and PFS with no asthma (17/153 (11%)) were consistent across respondents. In example cases 1, 3 & 4 (Figure 1) there was large variation with 98/154 (64%), 82/154 (53%) and 94/154 (61%), respectively, recommending AAIs. Over 90% of respondents in all regions except the Midlands & East (62%) would advise patients to carry two AAIs at all times in a case of anaphylaxis to peanut.
Dietary advice for avoidance of the index nut was consistent using a case of PA and tree NA at 97%. 118–120/155 (76%–77%) recommended additional tree nut avoidance if sensitised unless tolerated and consumed regularly, 47–49/155 (30%–32%) advised to consume foods with nut precautionary allergen labelling (PAL), while 50–52/155 (32%–34%) suggested the contrary.
The provision of SPT or sIgE testing, written allergy plans and medication are generally standardised across the UK. However, this survey provides further evidence that there is significant regional variation in provision of allied HCPs (dietitians and psychology support) particularly with regards to being present in clinic as part of a multidisciplinary team [2]. This may result in delays for families in receiving appropriate advice and, additional appointments, which have financial implications particularly for low-income families [3].
Diagnosis of NA relies on an allergy-focused history and SPT/sIgE, which is consistent with the BSACI NA guideline although there appears to be increasing use of CRDs, which should be reserved for cases of diagnostic uncertainty. This practice is unlikely to have been influenced by the BSACI PFS guideline published in 2022 as CRDs are only recommended in cases of uncertainty on primary tree nut/legume allergy or cases of possible primary tree nut/legume allergy and PFS [4]. However, the ‘EAACI Molecular Allergology User Guide 2.0’ in the case of diagnosis to peanut allergy suggests peanut specific IgE and Ara h 2 component as first-line investigations with a clear history [5]. It would be useful to determine further consensus on when CRD should be used as it has the potential of further increasing healthcare costs.
AAI prescribing practices are consistent in cases of clear anaphylaxis to peanut or PFS with no asthma. However, there is more variation in practice in other cases such as primary NA without anaphylaxis or PFS and asthma as well as regional variations (Repository information is available at https://osf.io/dvm3z/?view_only=ed289c3a6c3d4aa9ab3a5190c8f282d2). Both the BSACI and EAACI (European Academy of Allergy and Clinical Immunology) provide guidance but allow for lots of variation in practice in these grey areas [6, 7]. Continued education and dissemination of the guideline would enable greater consistency. Furthermore, research in identifying high-risk phenotypes in the grey cases would enable greater consensus amongst HCPs on AAI prescribing.
Variation also exists relating to dietary advice regarding avoidance of other nuts apart from the index nut and, on PAL. This does not seem to be influenced by dietetic service provision. Further consensus amongst HCPs in addition to the ongoing work by industry and the Food Standards Agency may result in a more consistent approach for patients.
We recognise that there was a low survey response rate; however, this is consistent with previous BSACI surveys. It illustrates an important snapshot of the current state of NA diagnosis and management and better dissemination of guidance may improve adherence. However, further work is required if the allergy community wish to provide a consistent message to patients in relation to dietetic and AAI provision.
G.S., A.D., A.T.C. and S.S. were involved in initial creation of audit questionnaire and execution of the project. F.N. collated and evaluated the data and all authors contributed to the writing and revision of the article.
Dr. Gary Stiefel is principal investigator on the NATASHA study looking at Peanut and milk desensitisation and is a trustee for Allergy UK. Dr. Andrew Clark is Chief Medical Officer and stockholder in Camallergy Ltd.
期刊介绍:
Clinical & Experimental Allergy strikes an excellent balance between clinical and scientific articles and carries regular reviews and editorials written by leading authorities in their field.
In response to the increasing number of quality submissions, since 1996 the journals size has increased by over 30%. Clinical & Experimental Allergy is essential reading for allergy practitioners and research scientists with an interest in allergic diseases and mechanisms. Truly international in appeal, Clinical & Experimental Allergy publishes clinical and experimental observations in disease in all fields of medicine in which allergic hypersensitivity plays a part.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


