Highly Curative Treatment of High-Risk Acute Promyelocytic Leukemia: Induction and Consolidation with ATRA+ATO+anthracyclines and Maintenance with ATRA+RIF.
Dan Liu, Juan Tong, Erling Chen, Li Wang, Lei Xue, Xuhan Zhang, Na Zhao, Xing Hu, Changcheng Zheng
{"title":"Highly Curative Treatment of High-Risk Acute Promyelocytic Leukemia: Induction and Consolidation with ATRA+ATO+anthracyclines and Maintenance with ATRA+RIF.","authors":"Dan Liu, Juan Tong, Erling Chen, Li Wang, Lei Xue, Xuhan Zhang, Na Zhao, Xing Hu, Changcheng Zheng","doi":"10.2147/BLCTT.S473984","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aim of the study was to evaluate the efficacy and safety of induction and consolidation with all-trans retinoic acid (ATRA) +arsenic trioxide (ATO) +anthracyclines and maintenance with ATRA +Realgar-<i>Indigo naturalis</i> formula (RIF) for high-risk APL.</p><p><strong>Methods: </strong>Twenty-one patients with high-risk APL treated with ATRA+ATO+ anthracyclines for induction and consolidation and ATRA+RIF for maintenance from 2012 to 2021 were analyzed. Endpoints include morphological complete remission (CR) and complete molecular remission (CMR), early death (ED) and relapse, survival and adverse events (AEs).</p><p><strong>Results: </strong>After induction treatment, all 21 patients (100%) achieved morphological CR and 14 people (66.7%) achieved CMR. Five of the 21 patients did not undergo immunological minimal residual disease (MRD) examination after induction; however, 14 of the remaining 16 patients were MRD negative (87.5%). The median time to achieve CR and CMR was 26 days (range: 16-44) and 40 days (range: 22-75), respectively. The cumulative probability of achieving CR and CMR in 45 days was 100% and 76.2% (95% CI: 56.9-91.3%), respectively. All patients achieved CMR and MRD negativity after the three courses of consolidation treatment. The median follow-up was 66 months (25-142), with no central nervous system relapse and bone marrow morphological or molecular relapse until now, and all patients survived with 100% overall survival and 100% event-free survival. Grade 4 adverse events (AEs) were observed in 3 patients (14.3%) during the induction period including arrhythmia (n = 1), pulmonary infection (n = 1) and respiratory failure (n = 1); and the most frequent grade 3 AEs were pulmonary infection, accounting for 62.0% and 28.6%, respectively, during induction and consolidation treatment, followed by neutropenia, accounting for 42.9% and 38.1%, respectively.</p><p><strong>Conclusion: </strong>For newly diagnosed high-risk APL patients, induction and consolidation with ATRA+ATO+anthracyclines and maintenance with ATRA+RIF is a highly curative treatment approach.</p>","PeriodicalId":42368,"journal":{"name":"Blood and Lymphatic Cancer-Targets and Therapy","volume":"14 ","pages":"63-69"},"PeriodicalIF":4.9000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11296505/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood and Lymphatic Cancer-Targets and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/BLCTT.S473984","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The aim of the study was to evaluate the efficacy and safety of induction and consolidation with all-trans retinoic acid (ATRA) +arsenic trioxide (ATO) +anthracyclines and maintenance with ATRA +Realgar-Indigo naturalis formula (RIF) for high-risk APL.
Methods: Twenty-one patients with high-risk APL treated with ATRA+ATO+ anthracyclines for induction and consolidation and ATRA+RIF for maintenance from 2012 to 2021 were analyzed. Endpoints include morphological complete remission (CR) and complete molecular remission (CMR), early death (ED) and relapse, survival and adverse events (AEs).
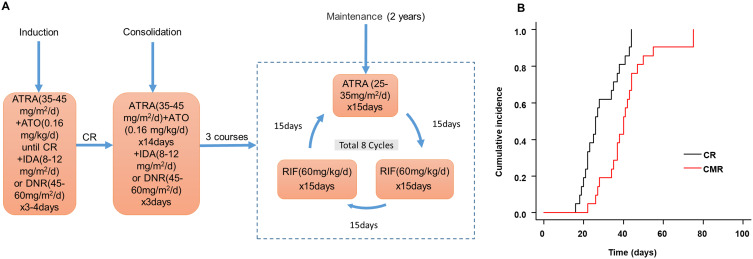
Results: After induction treatment, all 21 patients (100%) achieved morphological CR and 14 people (66.7%) achieved CMR. Five of the 21 patients did not undergo immunological minimal residual disease (MRD) examination after induction; however, 14 of the remaining 16 patients were MRD negative (87.5%). The median time to achieve CR and CMR was 26 days (range: 16-44) and 40 days (range: 22-75), respectively. The cumulative probability of achieving CR and CMR in 45 days was 100% and 76.2% (95% CI: 56.9-91.3%), respectively. All patients achieved CMR and MRD negativity after the three courses of consolidation treatment. The median follow-up was 66 months (25-142), with no central nervous system relapse and bone marrow morphological or molecular relapse until now, and all patients survived with 100% overall survival and 100% event-free survival. Grade 4 adverse events (AEs) were observed in 3 patients (14.3%) during the induction period including arrhythmia (n = 1), pulmonary infection (n = 1) and respiratory failure (n = 1); and the most frequent grade 3 AEs were pulmonary infection, accounting for 62.0% and 28.6%, respectively, during induction and consolidation treatment, followed by neutropenia, accounting for 42.9% and 38.1%, respectively.
Conclusion: For newly diagnosed high-risk APL patients, induction and consolidation with ATRA+ATO+anthracyclines and maintenance with ATRA+RIF is a highly curative treatment approach.
期刊介绍:
Blood and Lymphatic Cancer: Targets and Therapy is an international, peer reviewed, open access journal focusing on blood and lymphatic cancer research, identification of therapeutic targets, and the optimal use of preventative and integrated treatment interventions to achieve improved outcomes, enhanced survival, and quality of life for the cancer patient. Specific topics covered in the journal include: Epidemiology, detection and screening Cellular research and biomarkers Identification of biotargets and agents with novel mechanisms of action Optimal clinical use of existing anticancer agents, including combination therapies Radiation, surgery, bone marrow transplantation Palliative care Patient adherence, quality of life, satisfaction Health economic evaluations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


