Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Hirotaka Miyashita, Suzanna Lee, Mary K. Nesline, Sarabjot Pabla, Jeffrey M. Conroy, Paul DePietro, Heidi Ko, Jason K. Sicklick, Razelle Kurzrock
{"title":"4-1BB transcriptomic expression patterns across malignancies: Implications for clinical trials of 4-1BB agonists","authors":"Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Hirotaka Miyashita, Suzanna Lee, Mary K. Nesline, Sarabjot Pabla, Jeffrey M. Conroy, Paul DePietro, Heidi Ko, Jason K. Sicklick, Razelle Kurzrock","doi":"10.1002/cac2.12592","DOIUrl":null,"url":null,"abstract":"<p>4-1BB, a member of the tumor necrosis factor receptor superfamily, is an important co-stimulatory molecule regulating the activity of immune cells across a range of physiological and pathological processes, which culminates in a potent immune response (Figure 1A and B) [<span>1, 2</span>]. Numerous clinical trials have been conducted utilizing 4–1BB agonists (Supplemental Table S1); however, previous and ongoing 4-1BB agonist trials are being conducted without biomarker selection, which potentially explains their modest efficacy. Interestingly, several studies suggest the potential value of utilizing transcriptomics in addition to genomics to identify the unique immunologic signature of individual tumors [<span>3-7</span>].</p><p>Herein, we explore the landscape of 4–1BB transcriptomic profiles in 514 patients, including 489 with advanced/metastatic cancers and clinical annotation, and we discuss the potential therapeutic implications of the observed patterns and heterogeneity. The study methods are provided in the Supplementary File.</p><p>There were 514 tumors reflecting 31 different cancer types evaluated (Supplemental Table S2). Their median age was 61 (range, 24-93) years; 310 (60.3%) were women. The most frequent tumor types assessed were colorectal cancer (<i>n</i> = 140 samples). Of the 514 patients, 489 had confirmed metastatic or locally advanced disease, but the dates of metastatic disease for 25 patients were not documented. Overall, 489 patients with advanced/metastatic disease had fully evaluable clinical correlative data (Figure 1C). In total, 217 patients received ICIs; 199 received anti-programmed cell death 1 (PD-1)/ programmed death-ligand 1 (PD-L1) monotherapy, 2 received anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) monotherapy, and 16 received a combination of anti-PD-1/PD-L1 and anti-CTLA-4. The remaining 272 patients never received immunotherapy.</p><p>Figure 1D demonstrates the variations in 4-1BB RNA expression across different cancer types: 4-1BB ribonucleic acid (RNA) expression was classified as “high” (75-100th percentile), “moderate” (25-74th percentile), and “low” (0-24th percentile). Among all cancers (<i>n</i> = 514), 77 (15.0%) had high, 268 (52.1%) had moderate, and 169 (32.9%) had low 4-1BB expression. Small intestine and ovarian cancers most frequently had high 4-1BB RNA expression (25.0% and 20.9% of tumors, respectively).</p><p>To identify the patient population who might theoretically benefit the most from 4-1BB agonism, the proportion of patients having high 4-1BB expression along with low/moderate 4-1BB ligand (4-1BBL) expression was assessed in malignancies that had more than 20 representative samples (from a biologic point of view, high receptor with low/moderate ligand might be most amenable to treatment with 4-1BB agonists in the clinic). Malignancies with the highest proportion of patients having both high 4-1BB expression and low/moderate 4-1BBL expression were ovarian and pancreatic, with 18.6% (8/43) and 14.5% (8/55), respectively, representing the only two malignancies with >15% of patients having this expression profile (Figure 1E). Otherwise, the proportions of patients having high 4-1BB expression along with low/moderate 4-1BBL expression were 12.5% (3/24) in sarcoma, 12.5% (3/24) in uterine, 10.0% (2/20) in lung, 8.0% (2/25) in stomach, 7.9% (11/140) in colorectal, and 0% (0/49) in breast. There was variability of expression patterns both within and between tumor types. It is, therefore, conceivable that patient selection for 4-1BB agonist trials based in part on transcript levels may merit investigation.</p><p>We examined 12 genes that produce immunomodulatory molecules related to the TNF receptor superfamily or interacting co-stimulatory molecules, as well as markers related to ICIs in the clinic (Supplemental Table S3). The results of the univariable and the subsequent multivariable logistic regression are shown in Figure 1F. High RNA expression of 4-1BB was not associated with any specific tumor types. Among immune markers, high 4-1BB RNA expression was significantly associated with that of PD-L2 (odds ratio [OR] 3.1, 95% confidence interval [CI] 1.56–6.47, <i>P</i> = 0.018), ICOS (OR 4.5, 95% CI 2.03-10.36, <i>P</i> = 0.003), and CD27 (OR 2.2, 95% CI 1.12-4.81, <i>P</i> = 0.046) (all multivariable). When analyzing the pan-cancer whole genome cohort from the ICGC and TCGA (<i>n</i> = 2,658), ICOS RNA expression was the most significantly correlated with 4-1BB expression among 33,855 genes (spearman correlation coefficient (r): 0.77, <i>P</i> < 0.001; Figure 1G). Although high RNA expression of 4-1BB was not associated with high PD-1/PD-L1 expression in our cohort (Figure 1F), 4-1BB RNA expression was significantly correlated with PD-1 expression when examined as a linear variable (spearman correlation coefficient: 0.70, <i>P</i> < 0.001; Supplementary Figure S1). Additionally, PD-L2 and CD27 expression were also significantly correlated with 4-1BB expression (spearman correlation coefficient: 0.69, <i>P</i> < 0.001; and 0.53, <i>P</i> < 0.001, respectively, Figure 1G). Therefore, patients with cancer that co-expresses high PD-L2 may benefit from concomitant blocking of the immune inhibitory activity of PD-L2 if a 4-1BB agonist is given; this could be achieved by co-administering an anti-PD-1 agent since PD-L2 serves as a ligand for PD-1.</p><p>Survival outcomes were evaluable among 489 patients; among them, 272 patients never received immunotherapy, and 217 patients were treated with an immunotherapy-based regimen (Figure 1C). Among the 489 patients, the median overall survival (OS) was 51.7 months (95% CI, 43.3-61.3) for the high-4-1BB group and 35.7 months (95% CI, 30.3-44.0) for the low/moderate 4-1BB group, respectively, from the time of metastatic/advanced disease (hazard ratio [HR] = 0.74, 95%CI: 0.52-1.06, <i>P</i> = 0.103; Figure 1H). Regarding patients who never received immunotherapy, the median OS from advanced/metastatic disease was 51.7 months (95% CI, 24.4–not available [NA]) for the high-4-1BB group and 42.2 months (95% CI, 30.9-46.3) for the low/moderate 4-1BB group, respectively, from time of advanced/metastatic disease (HR = 0.83, 95%CI: 0.49-1.41, <i>P</i> = 0.497; Figure 1I).</p><p>In patients treated with immunotherapy (<i>n</i> = 217), the high 4-1BB group (<i>n</i> = 39) showed a trend towards longer progression-free survival (PFS) (HR = 0.70, 95%CI: 0.47-1.04, <i>P</i> = 0.074; Figure 1J) and significantly longer OS (HR = 0.55, 95%CI: 0.33-0.89, <i>P</i> = 0.016; Figure 1K) compared to the low/moderate 4-1BB group (<i>n</i> = 178) (calculated from start of immunotherapy). However, the significance of 4-1BB did not hold as an independent factor for survival in multivariable analysis (HR 0.83, 95% CI 0.47–1.46, <i>P</i> = 0.515; Supplemental Table S4). In contrast, in patients treated with immunotherapy, high 4-1BBL expression was not associated with longer PFS or OS (Supplementary Figure S2).</p><p>There are several limitations in this study due to its retrospective nature and limited sample size. First, although multiple types of cancer were represented, the number of patients for each type was relatively small. Secondly, our bulk analysis was not able to identify the cell types expressing 4-1BB and its ligand. In our bulk analysis, both high 4-1BB expression and high CD4/CD8 expression were observed in 10.7% of samples (Supplementary Table S5), suggesting that 4-1BB was expressed not only in T cells but also in tumor cells within the tumor microenvironment.</p><p>In summary, a myriad of reasons likely account for the suboptimal outcomes observed in current trials that focus on 4-1BB targeting. This study illuminates additional factors worth investigating in subsequent clinical trials. Based on our findings, 4-1BB and its ligand show variability of expression both between and within tumor types, indicating that cancers need to be sampled and analyzed in order to establish their individual immunomic portfolios. The concomitant high expression of 4-1BB and PD-L2 suggests that a combination approach that includes anti-PD-1 agents for malignancies with high PD-L2 expression warrants exploration.</p><p><i>Conception and design</i>: Yuji Uehara, Shumei Kato, Razelle Kurzrock. <i>Development of methodology</i>: Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. <i>Analysis and interpretation of data</i> (e.g., statistical analysis, biostatistics, computational analysis): Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. <i>Writing, review, and/or revision of the manuscript</i>: Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Hirotaka Miyashita, Suzanna Lee, Mary K. Nesline, Sarabjot Pabla, Jeffrey M. Conroy, Paul DePietro, Heidi Ko, Jason K. Sicklick, Razelle Kurzrock. <i>Administrative, technical, or material support</i> (i.e., reporting or organizing data, constructing databases): Suzanna Lee, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. <i>Study supervision</i>: Shumei Kato, Razelle Kurzrock.</p><p>Dr. Kato serves as a consultant for Medpace, Foundation Medicine, NeoGenomics, and CureMatch. He receives speaker's fees from Roche and Bayer, and the advisory board for Pfizer. He has research funding from ACT Genomics, Sysmex, Konica Minolta, OmniSeq, and Personalis.</p><p>Dr. Sicklick receives research funding from Novartis Pharmaceuticals, Amgen Pharmaceuticals, and Foundation Medicine; consultant fees from Grand Rounds, Loxo, and Deciphera; and speaker's fees from Roche and Deciphera. He also owns stocks in Personalis.</p><p>Dr. Kurzrock has received research funding from Boehringer Ingelheim, Debiopharm, Foundation Medicine, Genentech, Grifols, Guardant, Incyte, Konica Minolta, Medimmune, Merck Serono, Omniseq, Pfizer, Sequenom, Takeda, and TopAlliance and from the NCI; as well as consultant and/or speaker fees and/or advisory board/consultant for Actuate Therapeutics, AstraZeneca, Bicara Therapeutics, Inc., Biological Dynamics, Caris, Datar Cancer Genetics, Daiichi, EISAI, EOM Pharmaceuticals, Iylon, LabCorp, Merck, NeoGenomics, Neomed, Pfizer, Prosperdtx, Regeneron, Roche, TD2/Volastra, Turning Point Therapeutics, X-Biotech; has an equity interest in CureMatch Inc. and IDbyDNA; serves on the Board of CureMatch and CureMetrix, and is a co-founder of CureMatch. No potential conflicts of interest were disclosed by the other authors.</p><p>Dr. Kurzrock is funded in part by the National Institutes of Health (grant numbers: 5U01CA180888-08 and 5UG1CA233198-05.)</p><p>All investigations were conducted in accordance with the guidelines set by the Institutional Review Board of the University of California San Diego for data collection (Study of Personalized Cancer Therapy to Determine A Response and Toxicity, UCSD_PREDICT, NCT02478931) and all relevant investigational interventions for which the patients had provided consent.</p>","PeriodicalId":9495,"journal":{"name":"Cancer Communications","volume":"44 10","pages":"1168-1172"},"PeriodicalIF":24.9000,"publicationDate":"2024-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cac2.12592","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Communications","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cac2.12592","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
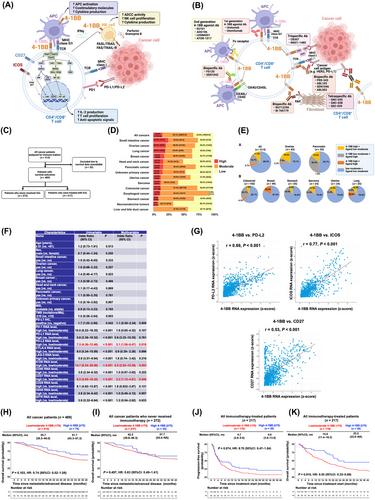
4-1BB, a member of the tumor necrosis factor receptor superfamily, is an important co-stimulatory molecule regulating the activity of immune cells across a range of physiological and pathological processes, which culminates in a potent immune response (Figure 1A and B) [1, 2]. Numerous clinical trials have been conducted utilizing 4–1BB agonists (Supplemental Table S1); however, previous and ongoing 4-1BB agonist trials are being conducted without biomarker selection, which potentially explains their modest efficacy. Interestingly, several studies suggest the potential value of utilizing transcriptomics in addition to genomics to identify the unique immunologic signature of individual tumors [3-7].
Herein, we explore the landscape of 4–1BB transcriptomic profiles in 514 patients, including 489 with advanced/metastatic cancers and clinical annotation, and we discuss the potential therapeutic implications of the observed patterns and heterogeneity. The study methods are provided in the Supplementary File.
There were 514 tumors reflecting 31 different cancer types evaluated (Supplemental Table S2). Their median age was 61 (range, 24-93) years; 310 (60.3%) were women. The most frequent tumor types assessed were colorectal cancer (n = 140 samples). Of the 514 patients, 489 had confirmed metastatic or locally advanced disease, but the dates of metastatic disease for 25 patients were not documented. Overall, 489 patients with advanced/metastatic disease had fully evaluable clinical correlative data (Figure 1C). In total, 217 patients received ICIs; 199 received anti-programmed cell death 1 (PD-1)/ programmed death-ligand 1 (PD-L1) monotherapy, 2 received anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) monotherapy, and 16 received a combination of anti-PD-1/PD-L1 and anti-CTLA-4. The remaining 272 patients never received immunotherapy.
Figure 1D demonstrates the variations in 4-1BB RNA expression across different cancer types: 4-1BB ribonucleic acid (RNA) expression was classified as “high” (75-100th percentile), “moderate” (25-74th percentile), and “low” (0-24th percentile). Among all cancers (n = 514), 77 (15.0%) had high, 268 (52.1%) had moderate, and 169 (32.9%) had low 4-1BB expression. Small intestine and ovarian cancers most frequently had high 4-1BB RNA expression (25.0% and 20.9% of tumors, respectively).
To identify the patient population who might theoretically benefit the most from 4-1BB agonism, the proportion of patients having high 4-1BB expression along with low/moderate 4-1BB ligand (4-1BBL) expression was assessed in malignancies that had more than 20 representative samples (from a biologic point of view, high receptor with low/moderate ligand might be most amenable to treatment with 4-1BB agonists in the clinic). Malignancies with the highest proportion of patients having both high 4-1BB expression and low/moderate 4-1BBL expression were ovarian and pancreatic, with 18.6% (8/43) and 14.5% (8/55), respectively, representing the only two malignancies with >15% of patients having this expression profile (Figure 1E). Otherwise, the proportions of patients having high 4-1BB expression along with low/moderate 4-1BBL expression were 12.5% (3/24) in sarcoma, 12.5% (3/24) in uterine, 10.0% (2/20) in lung, 8.0% (2/25) in stomach, 7.9% (11/140) in colorectal, and 0% (0/49) in breast. There was variability of expression patterns both within and between tumor types. It is, therefore, conceivable that patient selection for 4-1BB agonist trials based in part on transcript levels may merit investigation.
We examined 12 genes that produce immunomodulatory molecules related to the TNF receptor superfamily or interacting co-stimulatory molecules, as well as markers related to ICIs in the clinic (Supplemental Table S3). The results of the univariable and the subsequent multivariable logistic regression are shown in Figure 1F. High RNA expression of 4-1BB was not associated with any specific tumor types. Among immune markers, high 4-1BB RNA expression was significantly associated with that of PD-L2 (odds ratio [OR] 3.1, 95% confidence interval [CI] 1.56–6.47, P = 0.018), ICOS (OR 4.5, 95% CI 2.03-10.36, P = 0.003), and CD27 (OR 2.2, 95% CI 1.12-4.81, P = 0.046) (all multivariable). When analyzing the pan-cancer whole genome cohort from the ICGC and TCGA (n = 2,658), ICOS RNA expression was the most significantly correlated with 4-1BB expression among 33,855 genes (spearman correlation coefficient (r): 0.77, P < 0.001; Figure 1G). Although high RNA expression of 4-1BB was not associated with high PD-1/PD-L1 expression in our cohort (Figure 1F), 4-1BB RNA expression was significantly correlated with PD-1 expression when examined as a linear variable (spearman correlation coefficient: 0.70, P < 0.001; Supplementary Figure S1). Additionally, PD-L2 and CD27 expression were also significantly correlated with 4-1BB expression (spearman correlation coefficient: 0.69, P < 0.001; and 0.53, P < 0.001, respectively, Figure 1G). Therefore, patients with cancer that co-expresses high PD-L2 may benefit from concomitant blocking of the immune inhibitory activity of PD-L2 if a 4-1BB agonist is given; this could be achieved by co-administering an anti-PD-1 agent since PD-L2 serves as a ligand for PD-1.
Survival outcomes were evaluable among 489 patients; among them, 272 patients never received immunotherapy, and 217 patients were treated with an immunotherapy-based regimen (Figure 1C). Among the 489 patients, the median overall survival (OS) was 51.7 months (95% CI, 43.3-61.3) for the high-4-1BB group and 35.7 months (95% CI, 30.3-44.0) for the low/moderate 4-1BB group, respectively, from the time of metastatic/advanced disease (hazard ratio [HR] = 0.74, 95%CI: 0.52-1.06, P = 0.103; Figure 1H). Regarding patients who never received immunotherapy, the median OS from advanced/metastatic disease was 51.7 months (95% CI, 24.4–not available [NA]) for the high-4-1BB group and 42.2 months (95% CI, 30.9-46.3) for the low/moderate 4-1BB group, respectively, from time of advanced/metastatic disease (HR = 0.83, 95%CI: 0.49-1.41, P = 0.497; Figure 1I).
In patients treated with immunotherapy (n = 217), the high 4-1BB group (n = 39) showed a trend towards longer progression-free survival (PFS) (HR = 0.70, 95%CI: 0.47-1.04, P = 0.074; Figure 1J) and significantly longer OS (HR = 0.55, 95%CI: 0.33-0.89, P = 0.016; Figure 1K) compared to the low/moderate 4-1BB group (n = 178) (calculated from start of immunotherapy). However, the significance of 4-1BB did not hold as an independent factor for survival in multivariable analysis (HR 0.83, 95% CI 0.47–1.46, P = 0.515; Supplemental Table S4). In contrast, in patients treated with immunotherapy, high 4-1BBL expression was not associated with longer PFS or OS (Supplementary Figure S2).
There are several limitations in this study due to its retrospective nature and limited sample size. First, although multiple types of cancer were represented, the number of patients for each type was relatively small. Secondly, our bulk analysis was not able to identify the cell types expressing 4-1BB and its ligand. In our bulk analysis, both high 4-1BB expression and high CD4/CD8 expression were observed in 10.7% of samples (Supplementary Table S5), suggesting that 4-1BB was expressed not only in T cells but also in tumor cells within the tumor microenvironment.
In summary, a myriad of reasons likely account for the suboptimal outcomes observed in current trials that focus on 4-1BB targeting. This study illuminates additional factors worth investigating in subsequent clinical trials. Based on our findings, 4-1BB and its ligand show variability of expression both between and within tumor types, indicating that cancers need to be sampled and analyzed in order to establish their individual immunomic portfolios. The concomitant high expression of 4-1BB and PD-L2 suggests that a combination approach that includes anti-PD-1 agents for malignancies with high PD-L2 expression warrants exploration.
Conception and design: Yuji Uehara, Shumei Kato, Razelle Kurzrock. Development of methodology: Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational analysis): Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. Writing, review, and/or revision of the manuscript: Yuji Uehara, Shumei Kato, Daisuke Nishizaki, Hirotaka Miyashita, Suzanna Lee, Mary K. Nesline, Sarabjot Pabla, Jeffrey M. Conroy, Paul DePietro, Heidi Ko, Jason K. Sicklick, Razelle Kurzrock. Administrative, technical, or material support (i.e., reporting or organizing data, constructing databases): Suzanna Lee, Shumei Kato, Daisuke Nishizaki, Razelle Kurzrock. Study supervision: Shumei Kato, Razelle Kurzrock.
Dr. Kato serves as a consultant for Medpace, Foundation Medicine, NeoGenomics, and CureMatch. He receives speaker's fees from Roche and Bayer, and the advisory board for Pfizer. He has research funding from ACT Genomics, Sysmex, Konica Minolta, OmniSeq, and Personalis.
Dr. Sicklick receives research funding from Novartis Pharmaceuticals, Amgen Pharmaceuticals, and Foundation Medicine; consultant fees from Grand Rounds, Loxo, and Deciphera; and speaker's fees from Roche and Deciphera. He also owns stocks in Personalis.
Dr. Kurzrock has received research funding from Boehringer Ingelheim, Debiopharm, Foundation Medicine, Genentech, Grifols, Guardant, Incyte, Konica Minolta, Medimmune, Merck Serono, Omniseq, Pfizer, Sequenom, Takeda, and TopAlliance and from the NCI; as well as consultant and/or speaker fees and/or advisory board/consultant for Actuate Therapeutics, AstraZeneca, Bicara Therapeutics, Inc., Biological Dynamics, Caris, Datar Cancer Genetics, Daiichi, EISAI, EOM Pharmaceuticals, Iylon, LabCorp, Merck, NeoGenomics, Neomed, Pfizer, Prosperdtx, Regeneron, Roche, TD2/Volastra, Turning Point Therapeutics, X-Biotech; has an equity interest in CureMatch Inc. and IDbyDNA; serves on the Board of CureMatch and CureMetrix, and is a co-founder of CureMatch. No potential conflicts of interest were disclosed by the other authors.
Dr. Kurzrock is funded in part by the National Institutes of Health (grant numbers: 5U01CA180888-08 and 5UG1CA233198-05.)
All investigations were conducted in accordance with the guidelines set by the Institutional Review Board of the University of California San Diego for data collection (Study of Personalized Cancer Therapy to Determine A Response and Toxicity, UCSD_PREDICT, NCT02478931) and all relevant investigational interventions for which the patients had provided consent.
期刊介绍:
Cancer Communications is an open access, peer-reviewed online journal that encompasses basic, clinical, and translational cancer research. The journal welcomes submissions concerning clinical trials, epidemiology, molecular and cellular biology, and genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


