Robert T. Means Jr, Caixia Bi, Edward C. C. Wong, Lance A. Bare, Michael J. McPhaul
{"title":"Ferritin reference intervals in a population of working-age adults without anemia","authors":"Robert T. Means Jr, Caixia Bi, Edward C. C. Wong, Lance A. Bare, Michael J. McPhaul","doi":"10.1002/ajh.27444","DOIUrl":null,"url":null,"abstract":"<p>Iron deficiency anemia is recognized as one of the most important contributors to the worldwide burden of illness. It has a particularly high incidence in children and females of childbearing years in both the developed and less-developed world. It is generally recognized that serum ferritin concentration is the single most useful laboratory test in the diagnosis of iron deficiency.<span><sup>1</sup></span> However, it has significant limitations. Ferritin is an acute phase reactant and can be increased out of proportion to iron stores when inflammation is present and even without inflammation the specific ferritin concentration that represents iron deficiency is not clearly established, particularly in females.<span><sup>1, 2</sup></span></p><p>The authors reviewed anonymized data from 28,134 Quest Diagnostics employees participating in the Quest Blueprint For Wellness (BFW) screening program to evaluate age-specific ferritin reference intervals in a population of adults aged 18–80 years without anemia or other red cell abnormalities. In addition, changes in red cell indices in relation to serum ferritin concentrations (mean corpuscular volume (MCV); mean corpuscular hemoglobin (MCH); mean corpuscular hemoglobin concentration (MCHC); and the coefficient of variation of the red blood cell distribution width (RDW)) as well as the hemoglobin concentration, red blood cell concentration (RBC), and the hematocrit were analyzed in order to identify a more physiologic ferritin cutoff at which changes suggestive of iron deficiency may begin to appear. Individuals with values outside the Quest reference intervals for hemoglobin concentration, hematocrit, RBC, MCV, MCH, MCHC, and RDW (reference values shown in Table S2); serum total iron binding capacity (TIBC) saturation <20%; or an International Classification of Diseases-10 (ICD 10) code indicating an anemia diagnosis or a self-reported history of anemia on their BFW health questionnaire were excluded. To exclude individuals whose serum ferritin concentrations might be elevated out of proportion to iron stores by inflammation, individuals with high sensitivity C-reactive protein (hsCRP) >3 mg/L were excluded. Data from the remaining 24 812 individuals (55% female) were analyzed as presented below. Specific details of the study population including racial/ethnic and geographic demographics are shown in Table S1 and Figure S1.</p><p>The statistical technique multimodal decomposition was utilized to determine the reference ranges for serum ferritin concentrations in the final study population. Results were expressed by age deciles, with the lower limit representing the 2.5% confidence interval of population distribution for the individuals studied. A detailed description of methodology is provided in Supplemental Methods.</p><p>The ferritin reference interval lower limits for females 50 years of age or younger ranged between 11 and 13 ng/mL and were substantially lower than the lower limits for males in the same age ranges (39–41 ng/mL). However, for individuals over the age of 50, the lower limits of ferritin reference intervals for females increased, approaching but not equaling or exceeding the lower limit values observed for males until age greater than 70 years (increasing from 22 to 38 ng/mL). In contrast, the lower limit for males increased for ages 18 to 30 and 30 to 40 years but then declined and by the eighth decade was lower than the lower limit for females of the same age (28 ng/mL males vs. 38 ng/mL females). To evaluate whether the TIBC saturation cutoff at 20% was appropriate for excluding potentially iron deficient patients compared to a higher TIBC saturation cutoff, the lower limits of the ferritin reference interval for age deciles in males and females were evaluated at TIBC saturations ranging from greater than or equal to 20% to greater than or equal to 25%. There were no significant increases or decreases in ferritin reference interval lower limits. Full data are shown in Table S3.</p><p>Correlations between serum ferritin concentration and red cell parameters were statistically significant. The relationship between serum ferritin concentration and hemoglobin concentration, RBC, and MCV is shown in Figure 1. The nonparametric method LOESS (LOcally Estimated Scatterplot Smoothing) was utilized to fit a smooth curve and an inflection point was estimated for each curve by finding the lowest ferritin concentration where the LOESS curve started to plateau or where the rate of change on the y-axis was minimal. (Correlation values and LOESS curves/inflection points for all parameters are shown as Figures S2, S3 and in Tables S4 and S5). Changes in parameters that would be consistent with the development of iron deficiency (decreases in hemoglobin, hematocrit, RBC, MCV, MCH, and MCHC, and an increase in RDW) began to appear at serum ferritin concentrations less than 100 ng/mL. The ferritin concentrations at the inflection points for these changes were between 44 and 65 ng/mL. Ferritin concentrations at the curve inflection points in males were higher than those observed for females for all parameters, with a median difference of 10 ng/mL (95% confidence interval 2–24 ng/mL). Male/female inflection point differences were smallest for hemoglobin concentration and hematocrit (3 and 2 ng/mL, respectively), with male/female inflection point differences for other parameters studied between 9 and 21 ng/mL. Full results are shown in Table S5.</p><p>It has been suggested that, while the upper limits of the hemoglobin, hematocrit, and RBC concentration reference intervals may be intrinsically higher in males because of testosterone production, the reference interval lower limits for these parameters in healthy females may not be determined by intrinsic male/female differences but by a higher incidence of iron deficiency in females.<span><sup>3</sup></span> We examined this possibility in two ways. Ferritin reference intervals for females were recalculated after excluding individuals whose hemoglobin, hematocrit, and RBC values were below the cutoff value for males. This excluded 68% of the females in the original study population. However, the ferritin reference interval lower limits were essentially identical to those of the original study population for females under age 50 years, and only slightly higher for the 50–60 years and 60–70 years deciles (26 n/mL vs. 22 ng/mL; 31 mg/mL vs. 26 ng/mL, respectively). In all age deciles, the ferritin reference interval lower limit for males was higher, although the male/female difference decreased after age 50 years. There were too few females remaining in the 70–80 years decile for analysis. Full results are shown in Table S6.</p><p>To approach this same question from the perspective that differences in the hemoglobin and hematocrit reference interval lower limits for females and males could be a consequence of an increased incidence of iron deficiency (and hence lower ferritin values) in females, the hemoglobin and hematocrit distributions were calculated for individuals with serum ferritin greater than 50 ng/mL. The value of 50 ng/mL was selected because it approximates the median inflection point identified for the parameters studied. It is also consistent with reports that physiologic indicators of iron deficiency such as increased gastrointestinal absorption of iron<span><sup>4</sup></span> or increased serum soluble transferrin receptor concentrations and decreased serum hepcidin concentrations<span><sup>5</sup></span> begin to appear at a serum ferritin concentration of approximately 50 ng/mL. A difference in the lower limits of the hemoglobin and hematocrit distributions between males and females persists in all age deciles. The differences remain fairly consistent (1.0–1.6 g/dL hemoglobin, 2.5%–4.0% hematocrit) for all age deciles. This range of differences encompasses the differences between the male and female reference ranges used to exclude individuals from this analysis (1.5 g/dL hemoglobin, 3.5% hematocrit). Full results are shown in Table S7.</p><p>If a serum ferritin concentration of 50 ng/mL were used as the cutoff for iron deficiency in both males and females, 49.7% of females and 14.3% of males in this study population would be defined as iron deficient. When examined by age deciles, 71.5% of females in the 18–30 years category and 64.6% in the 30–40 years decile would be classified as iron deficient. The frequency of iron deficiency in females then decreases with age until it reaches 25.9% in the eighth decade of life. For males, the frequency of iron deficiency by this criterion remains between 13.3% and 14.3% until the seventh and eighth decades, when it increases slightly to 17.4% and 17.9%, respectively. Full results are shown in Table S8.</p><p>There is ongoing debate about the level of ferritin that defines iron deficiency and whether absence of marrow iron stores—the traditional definition of iron deficiency—is required for evidence of functional or tissue iron deficiency. A 2017 meta-analysis by Daru et al. reported that a stainable iron score of zero corresponded to a serum ferritin of 15 ng/mL or below, while reduced iron stores (stainable iron score 1+) represented a serum ferritin of approximately 70 ng/mL.<span><sup>6</sup></span> The present report suggests that changes in hemoglobin, hematocrit, RBC concentration, and RBC indices that could indicate early iron deficiency at a cellular level (decreasing MCV, MCH, MCHC, and increasing RDW) begin to appear at serum ferritin levels reported to indicate stainable iron stores that are reduced but not yet absent.</p><p>RTM: Affinergy LLC (consultant). CB, EW, LAB: Quest Diagnostic, Inc. (full-time employees). MJM: Quest Diagnostics, Inc. (consultant/medical director).</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 10","pages":"2047-2049"},"PeriodicalIF":10.1000,"publicationDate":"2024-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27444","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27444","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Iron deficiency anemia is recognized as one of the most important contributors to the worldwide burden of illness. It has a particularly high incidence in children and females of childbearing years in both the developed and less-developed world. It is generally recognized that serum ferritin concentration is the single most useful laboratory test in the diagnosis of iron deficiency.1 However, it has significant limitations. Ferritin is an acute phase reactant and can be increased out of proportion to iron stores when inflammation is present and even without inflammation the specific ferritin concentration that represents iron deficiency is not clearly established, particularly in females.1, 2
The authors reviewed anonymized data from 28,134 Quest Diagnostics employees participating in the Quest Blueprint For Wellness (BFW) screening program to evaluate age-specific ferritin reference intervals in a population of adults aged 18–80 years without anemia or other red cell abnormalities. In addition, changes in red cell indices in relation to serum ferritin concentrations (mean corpuscular volume (MCV); mean corpuscular hemoglobin (MCH); mean corpuscular hemoglobin concentration (MCHC); and the coefficient of variation of the red blood cell distribution width (RDW)) as well as the hemoglobin concentration, red blood cell concentration (RBC), and the hematocrit were analyzed in order to identify a more physiologic ferritin cutoff at which changes suggestive of iron deficiency may begin to appear. Individuals with values outside the Quest reference intervals for hemoglobin concentration, hematocrit, RBC, MCV, MCH, MCHC, and RDW (reference values shown in Table S2); serum total iron binding capacity (TIBC) saturation <20%; or an International Classification of Diseases-10 (ICD 10) code indicating an anemia diagnosis or a self-reported history of anemia on their BFW health questionnaire were excluded. To exclude individuals whose serum ferritin concentrations might be elevated out of proportion to iron stores by inflammation, individuals with high sensitivity C-reactive protein (hsCRP) >3 mg/L were excluded. Data from the remaining 24 812 individuals (55% female) were analyzed as presented below. Specific details of the study population including racial/ethnic and geographic demographics are shown in Table S1 and Figure S1.
The statistical technique multimodal decomposition was utilized to determine the reference ranges for serum ferritin concentrations in the final study population. Results were expressed by age deciles, with the lower limit representing the 2.5% confidence interval of population distribution for the individuals studied. A detailed description of methodology is provided in Supplemental Methods.
The ferritin reference interval lower limits for females 50 years of age or younger ranged between 11 and 13 ng/mL and were substantially lower than the lower limits for males in the same age ranges (39–41 ng/mL). However, for individuals over the age of 50, the lower limits of ferritin reference intervals for females increased, approaching but not equaling or exceeding the lower limit values observed for males until age greater than 70 years (increasing from 22 to 38 ng/mL). In contrast, the lower limit for males increased for ages 18 to 30 and 30 to 40 years but then declined and by the eighth decade was lower than the lower limit for females of the same age (28 ng/mL males vs. 38 ng/mL females). To evaluate whether the TIBC saturation cutoff at 20% was appropriate for excluding potentially iron deficient patients compared to a higher TIBC saturation cutoff, the lower limits of the ferritin reference interval for age deciles in males and females were evaluated at TIBC saturations ranging from greater than or equal to 20% to greater than or equal to 25%. There were no significant increases or decreases in ferritin reference interval lower limits. Full data are shown in Table S3.
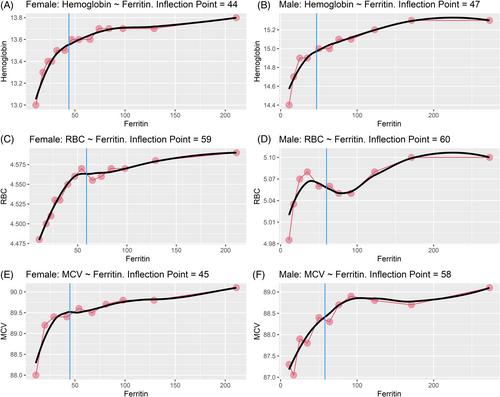
Correlations between serum ferritin concentration and red cell parameters were statistically significant. The relationship between serum ferritin concentration and hemoglobin concentration, RBC, and MCV is shown in Figure 1. The nonparametric method LOESS (LOcally Estimated Scatterplot Smoothing) was utilized to fit a smooth curve and an inflection point was estimated for each curve by finding the lowest ferritin concentration where the LOESS curve started to plateau or where the rate of change on the y-axis was minimal. (Correlation values and LOESS curves/inflection points for all parameters are shown as Figures S2, S3 and in Tables S4 and S5). Changes in parameters that would be consistent with the development of iron deficiency (decreases in hemoglobin, hematocrit, RBC, MCV, MCH, and MCHC, and an increase in RDW) began to appear at serum ferritin concentrations less than 100 ng/mL. The ferritin concentrations at the inflection points for these changes were between 44 and 65 ng/mL. Ferritin concentrations at the curve inflection points in males were higher than those observed for females for all parameters, with a median difference of 10 ng/mL (95% confidence interval 2–24 ng/mL). Male/female inflection point differences were smallest for hemoglobin concentration and hematocrit (3 and 2 ng/mL, respectively), with male/female inflection point differences for other parameters studied between 9 and 21 ng/mL. Full results are shown in Table S5.
It has been suggested that, while the upper limits of the hemoglobin, hematocrit, and RBC concentration reference intervals may be intrinsically higher in males because of testosterone production, the reference interval lower limits for these parameters in healthy females may not be determined by intrinsic male/female differences but by a higher incidence of iron deficiency in females.3 We examined this possibility in two ways. Ferritin reference intervals for females were recalculated after excluding individuals whose hemoglobin, hematocrit, and RBC values were below the cutoff value for males. This excluded 68% of the females in the original study population. However, the ferritin reference interval lower limits were essentially identical to those of the original study population for females under age 50 years, and only slightly higher for the 50–60 years and 60–70 years deciles (26 n/mL vs. 22 ng/mL; 31 mg/mL vs. 26 ng/mL, respectively). In all age deciles, the ferritin reference interval lower limit for males was higher, although the male/female difference decreased after age 50 years. There were too few females remaining in the 70–80 years decile for analysis. Full results are shown in Table S6.
To approach this same question from the perspective that differences in the hemoglobin and hematocrit reference interval lower limits for females and males could be a consequence of an increased incidence of iron deficiency (and hence lower ferritin values) in females, the hemoglobin and hematocrit distributions were calculated for individuals with serum ferritin greater than 50 ng/mL. The value of 50 ng/mL was selected because it approximates the median inflection point identified for the parameters studied. It is also consistent with reports that physiologic indicators of iron deficiency such as increased gastrointestinal absorption of iron4 or increased serum soluble transferrin receptor concentrations and decreased serum hepcidin concentrations5 begin to appear at a serum ferritin concentration of approximately 50 ng/mL. A difference in the lower limits of the hemoglobin and hematocrit distributions between males and females persists in all age deciles. The differences remain fairly consistent (1.0–1.6 g/dL hemoglobin, 2.5%–4.0% hematocrit) for all age deciles. This range of differences encompasses the differences between the male and female reference ranges used to exclude individuals from this analysis (1.5 g/dL hemoglobin, 3.5% hematocrit). Full results are shown in Table S7.
If a serum ferritin concentration of 50 ng/mL were used as the cutoff for iron deficiency in both males and females, 49.7% of females and 14.3% of males in this study population would be defined as iron deficient. When examined by age deciles, 71.5% of females in the 18–30 years category and 64.6% in the 30–40 years decile would be classified as iron deficient. The frequency of iron deficiency in females then decreases with age until it reaches 25.9% in the eighth decade of life. For males, the frequency of iron deficiency by this criterion remains between 13.3% and 14.3% until the seventh and eighth decades, when it increases slightly to 17.4% and 17.9%, respectively. Full results are shown in Table S8.
There is ongoing debate about the level of ferritin that defines iron deficiency and whether absence of marrow iron stores—the traditional definition of iron deficiency—is required for evidence of functional or tissue iron deficiency. A 2017 meta-analysis by Daru et al. reported that a stainable iron score of zero corresponded to a serum ferritin of 15 ng/mL or below, while reduced iron stores (stainable iron score 1+) represented a serum ferritin of approximately 70 ng/mL.6 The present report suggests that changes in hemoglobin, hematocrit, RBC concentration, and RBC indices that could indicate early iron deficiency at a cellular level (decreasing MCV, MCH, MCHC, and increasing RDW) begin to appear at serum ferritin levels reported to indicate stainable iron stores that are reduced but not yet absent.
RTM: Affinergy LLC (consultant). CB, EW, LAB: Quest Diagnostic, Inc. (full-time employees). MJM: Quest Diagnostics, Inc. (consultant/medical director).
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


