Abdul-Hamid Bazarbachi, Divaya Bhutani, Jai Radhakrishnan, Markus Mapara, Mathew S. Maurer, Suzanne Lentzsch, Rajshekhar Chakraborty
{"title":"Timing and outcomes of second-line therapy in the era of daratumumab-based frontline therapy in AL amyloidosis","authors":"Abdul-Hamid Bazarbachi, Divaya Bhutani, Jai Radhakrishnan, Markus Mapara, Mathew S. Maurer, Suzanne Lentzsch, Rajshekhar Chakraborty","doi":"10.1002/ajh.27450","DOIUrl":null,"url":null,"abstract":"<p>The therapeutic goal in immunoglobulin light-chain amyloidosis (AL) is to eradicate the plasma cell (PC) clone producing misfolded amyloid fibrils. Therapies for AL often draw inspiration from successful treatments in multiple myeloma (MM). However, the field faced a challenge when second-generation proteasome inhibitors and immunomodulatory drugs (IMiDs) used for MM proved poorly tolerated by AL patients, creating a significant treatment gap between the two diseases. The ANDROMEDA trial marked a turning point by combining daratumumab, a CD38-directed monoclonal antibody, with the previous standard of care—bortezomib, cyclophosphamide, and dexamethasone (VCd). This combination dramatically improved response rates, with approximately 80% of patients achieving a “≥” very good partial response (VGPR), compared to 50% with VCd alone.<span><sup>1</sup></span></p><p>Before the ANDROMEDA trial, approximately one-third of AL patients eventually required a second line of treatment (2nd LoT), often due to an unsatisfactory hematologic response (less than partial response [PR]), hematologic progression/relapse, and lack of organ response.<span><sup>2</sup></span> The landscape of 2nd LoT in the daratumumab era and the outcomes of such treatments are poorly characterized. Our study addresses this knowledge gap by examining the real-world outcomes of 100 consecutive patients with newly diagnosed AL who received upfront daratumumab-based therapy between January 2018 and December 2023.</p><p>The median age was 67.6 years [39.6–91.1]; 60% of patients were male; and the majority were White (67.3%) (Table S1). NYHA Class was III/IV in 44.3% at diagnosis. Most had lambda light chain involvement (76%), and median dFLC was 229 mg/L [2–9069]. Median NT-proBNP was 3317 ng/L [22–70 000], 26.9% ≥8500 ng/L. Median HS troponin-T was 64 ng/L [10–405]. Median BMPC percentage was 15% [2–70]. Regarding cytogenetics, 46% had <i>t</i>(11;14), 39.4% had del(13q), 40% had 1q gain/amplification, 28.6% had hyperdiploidy, and 13.4% had high-risk myeloma abnormalities. Most patients had modified Mayo 2004 stage IIIA (39.2%) or IIIB (24.7%) and renal stage II (46.3%). The most common frontline regimen was Dara-VCd (91%), followed by Dara-Vd/Dara-ixazomib-d (4%), Dara-d (4%), and Dara-Cd (1%), and 13% underwent ASCT consolidation. Comparing baseline characteristics between patients who received 2nd LoT versus those who did not, significant differences were noted in dFLC and %BMPC, with dFLC >180 mg/L in 78.8% versus 51.5% respectively (<i>p</i> = .005) and BMPC >15% in 67.6% versus 40.7% respectively (<i>p</i> = .02).</p><p>Median follow-up after 1st LoT was 22.3 months [2–69.7], with hematologic response evaluable for 84/100 patients. Most achieved either CR (46.4%), low-dFLC-PR (3.6%), or VGPR (21.4%) (Table S2). Twenty-three patients had either a PR (13.1%) or no response (NR) (15.5%) and received 2nd LoT. Overall, 34% required a 2nd LoT. Three patients who did not respond to frontline treatment did not receive subsequent therapy: two died shortly after diagnosis (massive ischemic stroke, cardiac arrest), and one opted for watchful waiting due to treatment intolerance. Other reasons for initiating subsequent treatments included hematologic relapse or progression in seven patients and minimal residual disease positivity in 4 patients (one with additional organ progression and one with rising BMPCs to 15%). Cardiac response was evaluable in 66 patients, with 51.5% achieving a response; renal response was evaluable in 29, with 62.1% achieving a response; liver response was evaluable in 11, with 45.5% achieving a response.</p><p>At the initiation of 2nd LoT, median dFLC was 91.5 mg/L [2–1853], 26.5% ≥180 (Table S3). Median NT-proBNP was 2456 ng/L [29.4–33 078], 21.2% ≥8500. Median HS troponin was 57 ng/L [9–221], and median 24-h urine protein was 1.47 g [0.18–13.45]. Most patients had modified Mayo 2004 stage II (34.4%) or IIIA (37.5%), and 12.5% had stage IIIB. The majority initially diagnosed with stage IIIB were downgraded to stage II or IIIA at 2nd LoT initiation (Figure S1). The most common 2nd LoT regimen was venetoclax-based (52.9%), followed by daratumumab-based (32.4%), ASCT (11.8%), and bendamustine-dex (2.9%) (Table S4). Patients treated with Dara-VCd, Dara-Vd, or Dara-Cd as 2nd LoT had achieved a CR or low-dFLC-PR to 1st LoT and experienced late (≥1 year) disease progression/relapse (median TTNT 22.6 months [11.9–51.2]). Patients treated with daratumumab plus an IMiD had a suboptimal response to frontline therapy (Figure 1A).</p><p>Hematologic response to 2nd LoT was evaluable for 33/34 patients. At a median follow-up of 17.8 months from 2nd LoT initiation [0.3–49], 45.5% achieved a CR, 3% a low dFLC-PR, 18.2% a VGPR, 3% a PR, and 30.3% had NR. Cardiac response was evaluable in 21/34 patients, with 52.4% achieving a response. One-third (32.4%) required a 3rd LoT, mainly due to suboptimal 2nd LoT response. Hematologic ≥VGPR rates were 30% for daratumumab-based combinations, 77.8% for venetoclax-based regimens, and 100% for other groups (<i>p</i> = .02, Figure 1A). For daratumumab-based regimens as 2nd LoT, patients with late disease progression/relapse achieved a ≥VGPR rate of 50%, and those with suboptimal 1st LoT response achieved a ≥VGPR rate of 16.7%. Cardiac response rates were 11.1% for daratumumab-based 2nd LoT. Most patients on daratumumab-based combinations needed a 3rd LoT (63.6%) compared to 22.2% in the venetoclax-based group and 0% in other groups (<i>p</i> = .03).</p><p>The one- and three-year TTNT from diagnosis were 71% (95% CI 62–81) and 61% (95% CI 50–74) (median 49.5 months). The one- and three-year OS from diagnosis were 87% (95% CI 81–94) and 72% (95% CI 62–84) (median not reached) (Figure S2, Table S5). Baseline characteristics significantly affecting TTNT were dFLC ≥180 mg/L (HR = 3.52, 95% CI 1.52–8.15, <i>p</i> = .003) (Figure 1B) and BMPC ≥15% (HR = 2.67, 95% CI 1.29–5.53, <i>p</i> = .008) (Figure 1C), and on multivariate analysis, baseline dFLC ≥180 had a significant negative effect on TTNT, with an adjusted HR of 2.75 (95% CI 1.13–6.7, <i>p</i> = .026) (Table S6). Baseline dFLC ≥180 also significantly affected OS on multivariate analysis (HR = 7.15, 95% CI 1.8–28.5, <i>p</i> = .0053), adjusting for NYHA class IV (HR = 10, 95% CI 3.22–31.2, <i>p</i> < .001), NT-proBNP ≥8500 (HR = 3.21, 95% CI 1.18–8.76, <i>p</i> = .022), number of organs involved (3+ vs. 1, HR = 3.1, 95% CI 1.18–8.19, <i>p</i> = .022), and BMPC ≥15% (HR = 0.168, 95% CI 0.0537–0.525, <i>p</i> = .0022).</p><p>Median EFS and OS after 2nd LoT were not reached. At 2 years, EFS was 52.1% (95% CI 35.9–75.6) and OS was 88% (95% CI 77.4–99.8). EFS after 2nd LoT was significantly worse in patients without <i>t</i>(11;14) (<i>p</i> = .0077) (Figure 1D). There were 21 deaths in total (Table S7), 4 of which occurred after 2nd LoT (2 in the daratumumab group and 2 in the venetoclax group) due to failure to thrive (50%), sepsis (25%), and unknown causes (25%).</p><p>Our study on AL amyloidosis with frontline daratumumab includes the largest cohort needing subsequent therapies. At ~2 years median follow-up, a third required 2nd LoT, predicted by high BMPCs and dFLC at diagnosis. Promising responses were seen with venetoclax-based 2nd LoT in <i>t</i>(11;14) patients.</p><p>Our results are comparable to ANDROMEDA, with 71.4% achieving ≥VGPR versus 78.5%, despite a higher proportion of stage IIIB patients at diagnosis versus 2% in ANDROMEDA.<span><sup>1</sup></span> Organ responses were similarly encouraging, with half showing a cardiac response and nearly two-thirds a renal response, compared to 41.5% and 53% in ANDROMEDA, respectively. This suggests that despite advanced disease in some patients, daratumumab can significantly improve organ function, crucial for improving patient outcomes. Palladini et al. previously reported AL outcomes in the 2nd line setting in the pre-daratumumab era.<span><sup>2</sup></span> Their study focused on patients who responded to initial therapy and later progressed, excluding those with suboptimal frontline responses. About 35% required a 2nd LoT after a median follow-up of 49 months. In contrast, most of our patients needed a 2nd LoT due to inadequate 1st LoT responses, with only seven due to hematologic progression or relapse. Zanwar et al. recently published their experience with frontline Dara-VCd, noting that after a median follow-up of 29 months, 24% of patients required subsequent therapy, primarily due to suboptimal response (79%), hematologic progression (11%), or rising sFLC from VGPR (7%).<span><sup>3</sup></span> Additional follow-up is needed to determine the proportion of patients who will experience hematologic progression/relapse after the initial response and whether responses with daratumumab are higher and more durable.</p><p>In our study, baseline BMPC percentage significantly affected TTNT, and baseline dFLC of ≥180 mg/L predicted both the need for a subsequent LoT and adverse impact on OS. Patients with elevated baseline dFLC were less likely to respond to upfront treatment and had worse outcomes even when other high-risk features were adjusted for in the multivariate analysis. Palladini et al. similarly observed that an FLC ratio of 6 at diagnosis was significant (<i>p</i> = .027).</p><p>Zanwar et al. noted a trend toward an increased incidence of gain/amp(1q) in patients requiring 2nd LoT versus those who didn't (36% vs. 18%; <i>p</i> = .06). However, cytogenetics did not predict 2nd LoT initiation in our study. Conversely, <i>t</i>(11;14) shows promise in the 2nd line setting. Our group and others have previously reported the efficacy of venetoclax in relapsed/refractory AL patients,<span><sup>4, 5</sup></span> a finding reaffirmed in this study. Alternative treatments with either bendamustine or rescue ASCT also hold promise.<span><sup>6</sup></span> However, retreatment with daratumumab, whether as a rescue with an IMiD for suboptimal responses or for late progressions/relapses, yielded subpar responses. Zanwar et al. similarly reported a 10% CR rate with subsequent daratumumab.</p><p>Patient outcomes after 2nd LoT were favorable in terms of hematologic and organ response rates as well as OS. Survival following the initiation of 2nd LoT was comparable to that observed with frontline therapy, indicating that patients could still be rescued with subsequent treatments. Similar findings were reported by Ravichandran et al. in the pre-daratumumab era, where durable treatment responses and depth of response were crucial predictors of outcomes across treatment lines despite multiple relapses up to the 4th line.<span><sup>7</sup></span></p><p>Several factors influence OS without affecting TTNT, including poor baseline performance status, advanced disease, and the extent of organ involvement, highlighting the unsalvageable organ damage caused by fibril deposition despite hematologic responses. Novel fibril-directed therapies, such as anselamimab and birtamimab, which bind to amyloid fibrils and promote resorption, offer promising avenues and are currently under development.<span><sup>8-10</sup></span></p><p>This study's limitations include its retrospective nature, limited sample size, and short follow-up. The non-randomized allocation for 2nd LoT limits definitive conclusions about the efficacies of different therapies, and variability in institutional practices due to a lack of standardized criteria for initiating 2nd LoT challenges the generalizability and reproducibility of our findings across different centers.</p><p>A.H.B. and R.C. designed/performed the research, collected the data, analyzed/interpreted the data, performed the statistical analysis, and wrote the manuscript. D.B., J.R., M.M., M.M., S.L., and R.C. proofread the manuscript and provided expert input.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":7724,"journal":{"name":"American Journal of Hematology","volume":"99 11","pages":"2225-2228"},"PeriodicalIF":10.1000,"publicationDate":"2024-08-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.27450","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Hematology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajh.27450","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
The therapeutic goal in immunoglobulin light-chain amyloidosis (AL) is to eradicate the plasma cell (PC) clone producing misfolded amyloid fibrils. Therapies for AL often draw inspiration from successful treatments in multiple myeloma (MM). However, the field faced a challenge when second-generation proteasome inhibitors and immunomodulatory drugs (IMiDs) used for MM proved poorly tolerated by AL patients, creating a significant treatment gap between the two diseases. The ANDROMEDA trial marked a turning point by combining daratumumab, a CD38-directed monoclonal antibody, with the previous standard of care—bortezomib, cyclophosphamide, and dexamethasone (VCd). This combination dramatically improved response rates, with approximately 80% of patients achieving a “≥” very good partial response (VGPR), compared to 50% with VCd alone.1
Before the ANDROMEDA trial, approximately one-third of AL patients eventually required a second line of treatment (2nd LoT), often due to an unsatisfactory hematologic response (less than partial response [PR]), hematologic progression/relapse, and lack of organ response.2 The landscape of 2nd LoT in the daratumumab era and the outcomes of such treatments are poorly characterized. Our study addresses this knowledge gap by examining the real-world outcomes of 100 consecutive patients with newly diagnosed AL who received upfront daratumumab-based therapy between January 2018 and December 2023.
The median age was 67.6 years [39.6–91.1]; 60% of patients were male; and the majority were White (67.3%) (Table S1). NYHA Class was III/IV in 44.3% at diagnosis. Most had lambda light chain involvement (76%), and median dFLC was 229 mg/L [2–9069]. Median NT-proBNP was 3317 ng/L [22–70 000], 26.9% ≥8500 ng/L. Median HS troponin-T was 64 ng/L [10–405]. Median BMPC percentage was 15% [2–70]. Regarding cytogenetics, 46% had t(11;14), 39.4% had del(13q), 40% had 1q gain/amplification, 28.6% had hyperdiploidy, and 13.4% had high-risk myeloma abnormalities. Most patients had modified Mayo 2004 stage IIIA (39.2%) or IIIB (24.7%) and renal stage II (46.3%). The most common frontline regimen was Dara-VCd (91%), followed by Dara-Vd/Dara-ixazomib-d (4%), Dara-d (4%), and Dara-Cd (1%), and 13% underwent ASCT consolidation. Comparing baseline characteristics between patients who received 2nd LoT versus those who did not, significant differences were noted in dFLC and %BMPC, with dFLC >180 mg/L in 78.8% versus 51.5% respectively (p = .005) and BMPC >15% in 67.6% versus 40.7% respectively (p = .02).
Median follow-up after 1st LoT was 22.3 months [2–69.7], with hematologic response evaluable for 84/100 patients. Most achieved either CR (46.4%), low-dFLC-PR (3.6%), or VGPR (21.4%) (Table S2). Twenty-three patients had either a PR (13.1%) or no response (NR) (15.5%) and received 2nd LoT. Overall, 34% required a 2nd LoT. Three patients who did not respond to frontline treatment did not receive subsequent therapy: two died shortly after diagnosis (massive ischemic stroke, cardiac arrest), and one opted for watchful waiting due to treatment intolerance. Other reasons for initiating subsequent treatments included hematologic relapse or progression in seven patients and minimal residual disease positivity in 4 patients (one with additional organ progression and one with rising BMPCs to 15%). Cardiac response was evaluable in 66 patients, with 51.5% achieving a response; renal response was evaluable in 29, with 62.1% achieving a response; liver response was evaluable in 11, with 45.5% achieving a response.
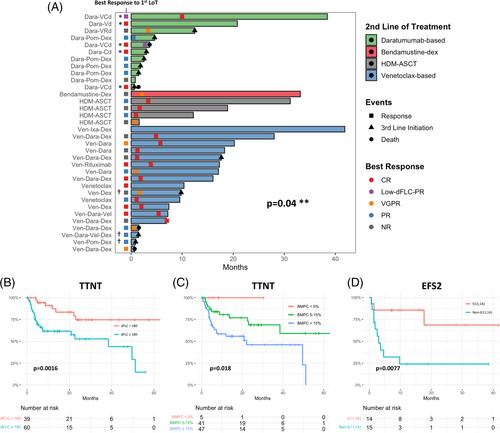
At the initiation of 2nd LoT, median dFLC was 91.5 mg/L [2–1853], 26.5% ≥180 (Table S3). Median NT-proBNP was 2456 ng/L [29.4–33 078], 21.2% ≥8500. Median HS troponin was 57 ng/L [9–221], and median 24-h urine protein was 1.47 g [0.18–13.45]. Most patients had modified Mayo 2004 stage II (34.4%) or IIIA (37.5%), and 12.5% had stage IIIB. The majority initially diagnosed with stage IIIB were downgraded to stage II or IIIA at 2nd LoT initiation (Figure S1). The most common 2nd LoT regimen was venetoclax-based (52.9%), followed by daratumumab-based (32.4%), ASCT (11.8%), and bendamustine-dex (2.9%) (Table S4). Patients treated with Dara-VCd, Dara-Vd, or Dara-Cd as 2nd LoT had achieved a CR or low-dFLC-PR to 1st LoT and experienced late (≥1 year) disease progression/relapse (median TTNT 22.6 months [11.9–51.2]). Patients treated with daratumumab plus an IMiD had a suboptimal response to frontline therapy (Figure 1A).
Hematologic response to 2nd LoT was evaluable for 33/34 patients. At a median follow-up of 17.8 months from 2nd LoT initiation [0.3–49], 45.5% achieved a CR, 3% a low dFLC-PR, 18.2% a VGPR, 3% a PR, and 30.3% had NR. Cardiac response was evaluable in 21/34 patients, with 52.4% achieving a response. One-third (32.4%) required a 3rd LoT, mainly due to suboptimal 2nd LoT response. Hematologic ≥VGPR rates were 30% for daratumumab-based combinations, 77.8% for venetoclax-based regimens, and 100% for other groups (p = .02, Figure 1A). For daratumumab-based regimens as 2nd LoT, patients with late disease progression/relapse achieved a ≥VGPR rate of 50%, and those with suboptimal 1st LoT response achieved a ≥VGPR rate of 16.7%. Cardiac response rates were 11.1% for daratumumab-based 2nd LoT. Most patients on daratumumab-based combinations needed a 3rd LoT (63.6%) compared to 22.2% in the venetoclax-based group and 0% in other groups (p = .03).
The one- and three-year TTNT from diagnosis were 71% (95% CI 62–81) and 61% (95% CI 50–74) (median 49.5 months). The one- and three-year OS from diagnosis were 87% (95% CI 81–94) and 72% (95% CI 62–84) (median not reached) (Figure S2, Table S5). Baseline characteristics significantly affecting TTNT were dFLC ≥180 mg/L (HR = 3.52, 95% CI 1.52–8.15, p = .003) (Figure 1B) and BMPC ≥15% (HR = 2.67, 95% CI 1.29–5.53, p = .008) (Figure 1C), and on multivariate analysis, baseline dFLC ≥180 had a significant negative effect on TTNT, with an adjusted HR of 2.75 (95% CI 1.13–6.7, p = .026) (Table S6). Baseline dFLC ≥180 also significantly affected OS on multivariate analysis (HR = 7.15, 95% CI 1.8–28.5, p = .0053), adjusting for NYHA class IV (HR = 10, 95% CI 3.22–31.2, p < .001), NT-proBNP ≥8500 (HR = 3.21, 95% CI 1.18–8.76, p = .022), number of organs involved (3+ vs. 1, HR = 3.1, 95% CI 1.18–8.19, p = .022), and BMPC ≥15% (HR = 0.168, 95% CI 0.0537–0.525, p = .0022).
Median EFS and OS after 2nd LoT were not reached. At 2 years, EFS was 52.1% (95% CI 35.9–75.6) and OS was 88% (95% CI 77.4–99.8). EFS after 2nd LoT was significantly worse in patients without t(11;14) (p = .0077) (Figure 1D). There were 21 deaths in total (Table S7), 4 of which occurred after 2nd LoT (2 in the daratumumab group and 2 in the venetoclax group) due to failure to thrive (50%), sepsis (25%), and unknown causes (25%).
Our study on AL amyloidosis with frontline daratumumab includes the largest cohort needing subsequent therapies. At ~2 years median follow-up, a third required 2nd LoT, predicted by high BMPCs and dFLC at diagnosis. Promising responses were seen with venetoclax-based 2nd LoT in t(11;14) patients.
Our results are comparable to ANDROMEDA, with 71.4% achieving ≥VGPR versus 78.5%, despite a higher proportion of stage IIIB patients at diagnosis versus 2% in ANDROMEDA.1 Organ responses were similarly encouraging, with half showing a cardiac response and nearly two-thirds a renal response, compared to 41.5% and 53% in ANDROMEDA, respectively. This suggests that despite advanced disease in some patients, daratumumab can significantly improve organ function, crucial for improving patient outcomes. Palladini et al. previously reported AL outcomes in the 2nd line setting in the pre-daratumumab era.2 Their study focused on patients who responded to initial therapy and later progressed, excluding those with suboptimal frontline responses. About 35% required a 2nd LoT after a median follow-up of 49 months. In contrast, most of our patients needed a 2nd LoT due to inadequate 1st LoT responses, with only seven due to hematologic progression or relapse. Zanwar et al. recently published their experience with frontline Dara-VCd, noting that after a median follow-up of 29 months, 24% of patients required subsequent therapy, primarily due to suboptimal response (79%), hematologic progression (11%), or rising sFLC from VGPR (7%).3 Additional follow-up is needed to determine the proportion of patients who will experience hematologic progression/relapse after the initial response and whether responses with daratumumab are higher and more durable.
In our study, baseline BMPC percentage significantly affected TTNT, and baseline dFLC of ≥180 mg/L predicted both the need for a subsequent LoT and adverse impact on OS. Patients with elevated baseline dFLC were less likely to respond to upfront treatment and had worse outcomes even when other high-risk features were adjusted for in the multivariate analysis. Palladini et al. similarly observed that an FLC ratio of 6 at diagnosis was significant (p = .027).
Zanwar et al. noted a trend toward an increased incidence of gain/amp(1q) in patients requiring 2nd LoT versus those who didn't (36% vs. 18%; p = .06). However, cytogenetics did not predict 2nd LoT initiation in our study. Conversely, t(11;14) shows promise in the 2nd line setting. Our group and others have previously reported the efficacy of venetoclax in relapsed/refractory AL patients,4, 5 a finding reaffirmed in this study. Alternative treatments with either bendamustine or rescue ASCT also hold promise.6 However, retreatment with daratumumab, whether as a rescue with an IMiD for suboptimal responses or for late progressions/relapses, yielded subpar responses. Zanwar et al. similarly reported a 10% CR rate with subsequent daratumumab.
Patient outcomes after 2nd LoT were favorable in terms of hematologic and organ response rates as well as OS. Survival following the initiation of 2nd LoT was comparable to that observed with frontline therapy, indicating that patients could still be rescued with subsequent treatments. Similar findings were reported by Ravichandran et al. in the pre-daratumumab era, where durable treatment responses and depth of response were crucial predictors of outcomes across treatment lines despite multiple relapses up to the 4th line.7
Several factors influence OS without affecting TTNT, including poor baseline performance status, advanced disease, and the extent of organ involvement, highlighting the unsalvageable organ damage caused by fibril deposition despite hematologic responses. Novel fibril-directed therapies, such as anselamimab and birtamimab, which bind to amyloid fibrils and promote resorption, offer promising avenues and are currently under development.8-10
This study's limitations include its retrospective nature, limited sample size, and short follow-up. The non-randomized allocation for 2nd LoT limits definitive conclusions about the efficacies of different therapies, and variability in institutional practices due to a lack of standardized criteria for initiating 2nd LoT challenges the generalizability and reproducibility of our findings across different centers.
A.H.B. and R.C. designed/performed the research, collected the data, analyzed/interpreted the data, performed the statistical analysis, and wrote the manuscript. D.B., J.R., M.M., M.M., S.L., and R.C. proofread the manuscript and provided expert input.
期刊介绍:
The American Journal of Hematology offers extensive coverage of experimental and clinical aspects of blood diseases in humans and animal models. The journal publishes original contributions in both non-malignant and malignant hematological diseases, encompassing clinical and basic studies in areas such as hemostasis, thrombosis, immunology, blood banking, and stem cell biology. Clinical translational reports highlighting innovative therapeutic approaches for the diagnosis and treatment of hematological diseases are actively encouraged.The American Journal of Hematology features regular original laboratory and clinical research articles, brief research reports, critical reviews, images in hematology, as well as letters and correspondence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


