Development and validation of an individualized nomogram for gastric cancer patients treated with perioperative chemotherapy followed by radical surgery.
Yan Wang, Shilong Zhang, Bowen Ding, Zhaoqing Tang, Yuan Ji, Yiyi Yu, Yuehong Cui, Xuefei Wang, Yihong Sun, Tianshu Liu
{"title":"Development and validation of an individualized nomogram for gastric cancer patients treated with perioperative chemotherapy followed by radical surgery.","authors":"Yan Wang, Shilong Zhang, Bowen Ding, Zhaoqing Tang, Yuan Ji, Yiyi Yu, Yuehong Cui, Xuefei Wang, Yihong Sun, Tianshu Liu","doi":"10.21037/tgh-23-75","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prognostic factors are complicated and changeable for locally advanced gastric cancer (GC) patients. This study aimed to perform a novel prognostic model on survival for locally advanced GC patients who have received neoadjuvant chemotherapy and radical surgery.</p><p><strong>Methods: </strong>The locally advanced GC patients with neoadjuvant chemotherapy were included in this study from Zhongshan Hospital, Fudan University. A nomogram was developed based on independent prognostic factors identified through a multivariable Cox regression model. Model performance was evaluated in training and independent external cohorts in terms of calibration, discrimination, and clinical usefulness.</p><p><strong>Results: </strong>A total of 273 patients received radical resections. The median progression-free survival (PFS) and overall survival (OS) for all patients were 43.8 and 61.2 months, respectively. Nomogram showed that Lauren type made the greatest contribution to prognosis, followed by ypN. The prognostic nomogram had excellent discriminative ability, with a C-index of 0.689 [95% confidence interval (CI): 0.661-0.716], and an area under the receiver operating characteristic (ROC) curve (AUC) of 0.778, 0.746, and 0.725 for 3-, 5- and 10-year OS, respectively. Similar results were obtained in the external validation cohort. Based on the nomogram, the whole cohort was divided into high-risk and low-risk groups. And risk group classification was significantly associated with clinical characteristics, and produced an AUC value of 0.781, 0.748, and 0.727 for 3-, 5- and 10-year OS, respectively. Furthermore, compared with the tumor-node-metastasis (TNM) staging system (8th edition), Japanese criteria, and German criteria, the decision curve analysis (DCA) graphically demonstrated that the new model had more optimal net benefits in predicting the 3-, 5-, and 10-year OS for GC patients. Both C-index and time-dependent ROC curve demonstrated that the nomogram had a stronger capability for accurately predicting prognosis compared with the other staging system.</p><p><strong>Conclusions: </strong>The nomogram model is an effective support tool to predict OS in GC patients undergoing perioperative chemotherapy followed by radical surgery.</p>","PeriodicalId":94362,"journal":{"name":"Translational gastroenterology and hepatology","volume":"9 ","pages":"39"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11292059/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational gastroenterology and hepatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/tgh-23-75","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prognostic factors are complicated and changeable for locally advanced gastric cancer (GC) patients. This study aimed to perform a novel prognostic model on survival for locally advanced GC patients who have received neoadjuvant chemotherapy and radical surgery.
Methods: The locally advanced GC patients with neoadjuvant chemotherapy were included in this study from Zhongshan Hospital, Fudan University. A nomogram was developed based on independent prognostic factors identified through a multivariable Cox regression model. Model performance was evaluated in training and independent external cohorts in terms of calibration, discrimination, and clinical usefulness.
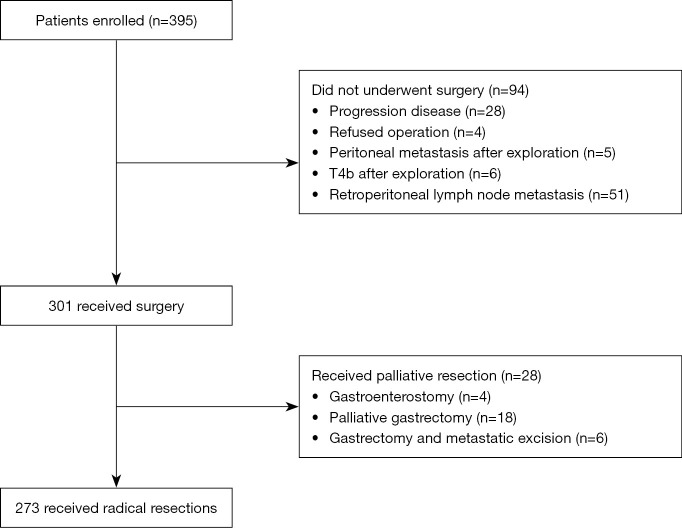
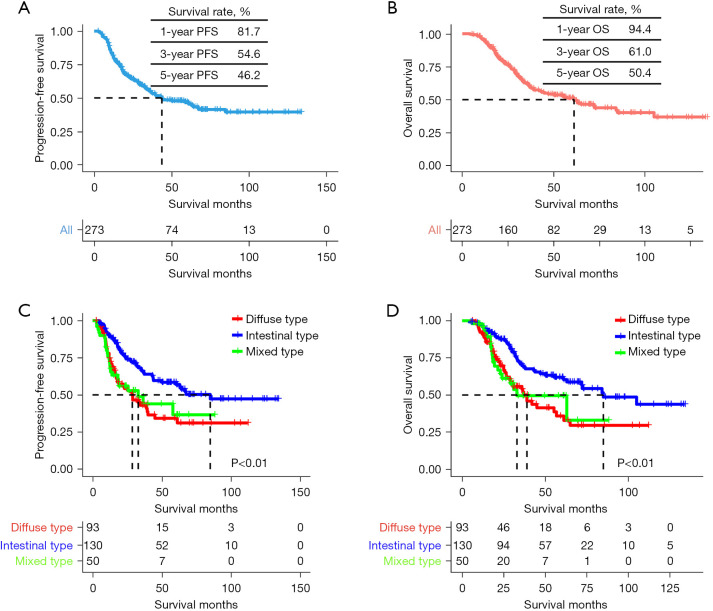
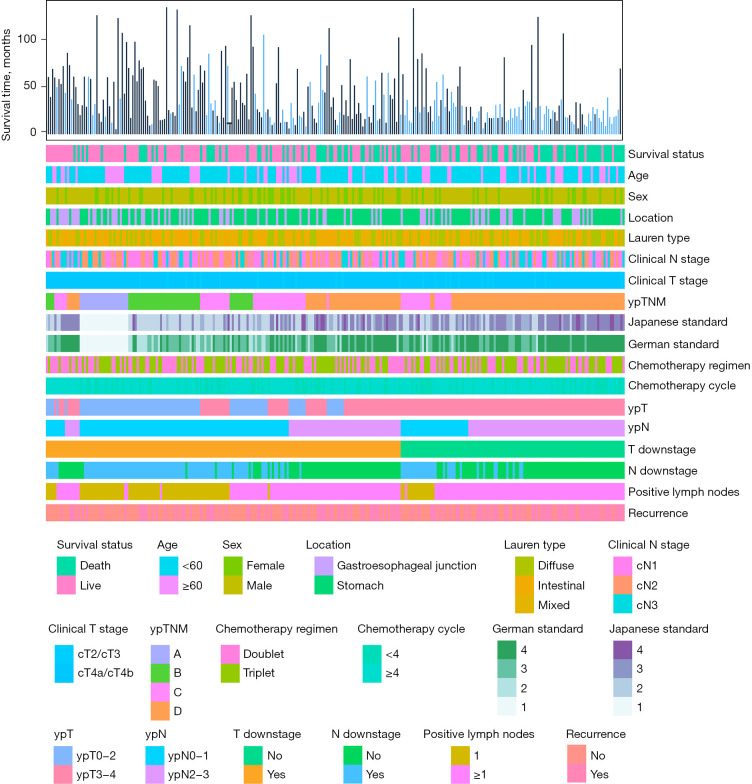
Results: A total of 273 patients received radical resections. The median progression-free survival (PFS) and overall survival (OS) for all patients were 43.8 and 61.2 months, respectively. Nomogram showed that Lauren type made the greatest contribution to prognosis, followed by ypN. The prognostic nomogram had excellent discriminative ability, with a C-index of 0.689 [95% confidence interval (CI): 0.661-0.716], and an area under the receiver operating characteristic (ROC) curve (AUC) of 0.778, 0.746, and 0.725 for 3-, 5- and 10-year OS, respectively. Similar results were obtained in the external validation cohort. Based on the nomogram, the whole cohort was divided into high-risk and low-risk groups. And risk group classification was significantly associated with clinical characteristics, and produced an AUC value of 0.781, 0.748, and 0.727 for 3-, 5- and 10-year OS, respectively. Furthermore, compared with the tumor-node-metastasis (TNM) staging system (8th edition), Japanese criteria, and German criteria, the decision curve analysis (DCA) graphically demonstrated that the new model had more optimal net benefits in predicting the 3-, 5-, and 10-year OS for GC patients. Both C-index and time-dependent ROC curve demonstrated that the nomogram had a stronger capability for accurately predicting prognosis compared with the other staging system.
Conclusions: The nomogram model is an effective support tool to predict OS in GC patients undergoing perioperative chemotherapy followed by radical surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


