Preoperative CT findings predict the development of metachronous contralateral inguinal hernia after unilateral inguinal hernia repair: a single-center retrospective cohort study.
Hang Yu, Jiajie Qian, Yang Dong, Tang Yu, Ying Zeng, Qianyun Shen
{"title":"Preoperative CT findings predict the development of metachronous contralateral inguinal hernia after unilateral inguinal hernia repair: a single-center retrospective cohort study.","authors":"Hang Yu, Jiajie Qian, Yang Dong, Tang Yu, Ying Zeng, Qianyun Shen","doi":"10.1007/s10029-024-03123-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To identify potential clinical and preoperative CT risk factors that can predict the development of metachronous contralateral inguinal hernia (MCIH) after unilateral inguinal hernia repair (IHR).</p><p><strong>Methods: </strong>This study included unilateral inguinal hernia patients seen from 2016 to 2019 who underwent CT and subsequent IHR and had at least five years of follow-up. Preoperative CT scans were retrospectively reviewed for the presence of asymmetric spermatic cord fat and weakness of the transversalis fascia. The correlations of each CT feature and other clinical characteristics with the development of MCIH were calculated. The Kaplan-Meier model and multiple logistic regression were used to evaluate the associations among CT features, clinical variables and MCIH.</p><p><strong>Results: </strong>A total of 677 male patients aged > 40 years were included in the study cohort. After more than 5 years of follow-up, 162 patients developed MCIH, representing an incidence of 23.9%. Patients with radical prostatectomy or peritoneal dialysis [P < 0.0001, HR 4.189 (95% CI 2.369 to 7.406)], primary left-sided IHR [P = 0.0032, HR 1.626 (95% CI 1.177 to 2.244)], and direct, femoral or pantaloon hernias were predisposed to MCIH. Asymmetric spermatic cord fat [P = 0.0002, HR 1.203 (95% CI 0.8785 to 1.648)] and weakness of the transversalis fascia [P < 0.0001, HR 7.914 (95% CI 5.666 to 11.05)] on preoperative CT were also identified as risk facts and demonstrated to be independent predictive factors for MCIH development.</p><p><strong>Conclusion: </strong>Asymmetric spermatic cord fat and weakness of the transversalis fascia were predictive factors for MCIH development. For decision making regarding prophylactic contralateral IHR at the time of index surgery, preoperative CT findings as well as clinical characteristics should be considered.</p>","PeriodicalId":13168,"journal":{"name":"Hernia","volume":" ","pages":"1925-1934"},"PeriodicalIF":2.6000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hernia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10029-024-03123-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/31 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To identify potential clinical and preoperative CT risk factors that can predict the development of metachronous contralateral inguinal hernia (MCIH) after unilateral inguinal hernia repair (IHR).
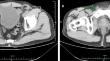
Methods: This study included unilateral inguinal hernia patients seen from 2016 to 2019 who underwent CT and subsequent IHR and had at least five years of follow-up. Preoperative CT scans were retrospectively reviewed for the presence of asymmetric spermatic cord fat and weakness of the transversalis fascia. The correlations of each CT feature and other clinical characteristics with the development of MCIH were calculated. The Kaplan-Meier model and multiple logistic regression were used to evaluate the associations among CT features, clinical variables and MCIH.
Results: A total of 677 male patients aged > 40 years were included in the study cohort. After more than 5 years of follow-up, 162 patients developed MCIH, representing an incidence of 23.9%. Patients with radical prostatectomy or peritoneal dialysis [P < 0.0001, HR 4.189 (95% CI 2.369 to 7.406)], primary left-sided IHR [P = 0.0032, HR 1.626 (95% CI 1.177 to 2.244)], and direct, femoral or pantaloon hernias were predisposed to MCIH. Asymmetric spermatic cord fat [P = 0.0002, HR 1.203 (95% CI 0.8785 to 1.648)] and weakness of the transversalis fascia [P < 0.0001, HR 7.914 (95% CI 5.666 to 11.05)] on preoperative CT were also identified as risk facts and demonstrated to be independent predictive factors for MCIH development.
Conclusion: Asymmetric spermatic cord fat and weakness of the transversalis fascia were predictive factors for MCIH development. For decision making regarding prophylactic contralateral IHR at the time of index surgery, preoperative CT findings as well as clinical characteristics should be considered.
期刊介绍:
Hernia was founded in 1997 by Jean P. Chevrel with the purpose of promoting clinical studies and basic research as they apply to groin hernias and the abdominal wall . Since that time, a true revolution in the field of hernia studies has transformed the field from a ”simple” disease to one that is very specialized. While the majority of surgeries for primary inguinal and abdominal wall hernia are performed in hospitals worldwide, complex situations such as multi recurrences, complications, abdominal wall reconstructions and others are being studied and treated in specialist centers. As a result, major institutions and societies are creating specific parameters and criteria to better address the complexities of hernia surgery.
Hernia is a journal written by surgeons who have made abdominal wall surgery their specific field of interest, but we will consider publishing content from any surgeon who wishes to improve the science of this field. The Journal aims to ensure that hernia surgery is safer and easier for surgeons as well as patients, and provides a forum to all surgeons in the exchange of new ideas, results, and important research that is the basis of professional activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


