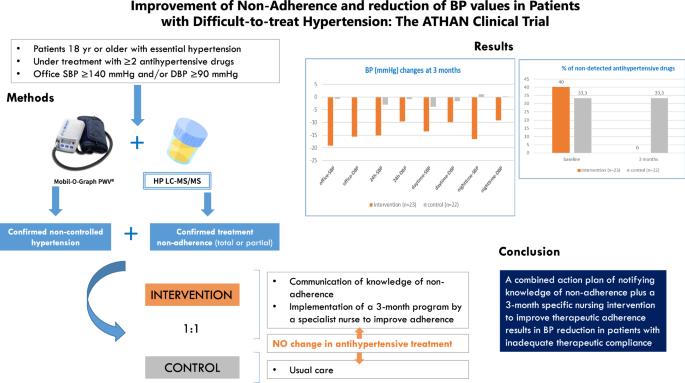
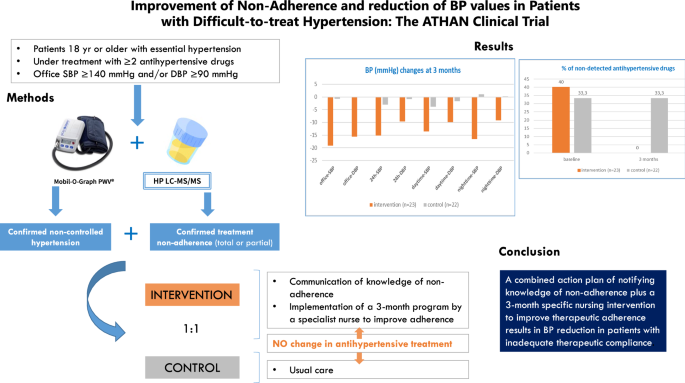
Improvement of non-adherence and reduction of BP values in patients with difficult-to-treat hypertension: the ATHAN clinical trial
IF 4.3
2区 医学
Q1 PERIPHERAL VASCULAR DISEASE
引用次数: 0
Abstract
Hypertension treatment and blood pressure (BP) control reduce cardiovascular disease burden. However, prevalence of controlled BP is overall insufficient and lack of adherence to treatment is a suggested major contributor. This prospective, randomized clinical trial was designed to evaluate whether a specific 3-month (m) action plan to improve therapeutic adherence results in a decrease in BP. Patients with ambulatory 24 h-BP ≥ 130/80 mmHg despite receiving ≥2 antihypertensive drugs and with therapeutic non-compliance confirmed by antihypertensive drugs analyzed in urine were randomized (1:1) to receive a specific 3 m program to improve adherence (INT = intervention) or routine follow-up (C = control). Antihypertensive treatment was not modified and knowledge of non-adherence was only notified to patients randomized to the intervention group. Before randomization and at 3 m all patients underwent urinary screening for antihypertensive drugs and 24 h-ambulatory-BP monitoring. Forty-five patients (36% women, mean age: 58 ± 13 yr) were randomized. At 3 m, mean (95% CI) BP differences (INT vs. C) were 12.2 mmHg (4.3–20.8), adjusted-p = 0.032 and 8.7 mmHg (2.5–14.8), adjusted-p = 0.018 for 24 h-systolic and 24 h-diastolic BP, respectively. Differences (INT vs. C) for office SBP and DBP were 18.4 mmHg (6.8–30.1), adjusted-p = 0.005 and 15.7 mmHg (7.2–24.2), adjusted-p < 0.001. Non-detected antihypertensive drugs were median [IQR]: 40% [25–100] and 0% [0–20] at baseline and 3 m, respectively, in the INT group, and 33.3% [25–63.7] and 33.3% [23.8–57.9], in the C group (p < 0.001 for the 3-month between-group comparison). A combined action plan of notifying knowledge of non-adherence plus a 3-month specific nursing intervention to improve therapeutic adherence results in BP reduction in patients with inadequate therapeutic compliance.
改善难以治疗的高血压患者的不依从性并降低血压值:ATHAN 临床试验。
高血压治疗和血压(BP)控制可减轻心血管疾病负担。然而,总体而言,血压控制的普及率还不够高,而缺乏对治疗的依从性是一个主要原因。这项前瞻性随机临床试验旨在评估一项为期 3 个月(m)的具体行动计划是否能提高治疗依从性,从而降低血压。在接受了≥2 种降压药物治疗后,24 小时动态血压仍≥ 130/80 mmHg,并通过尿液中的降压药物分析确认治疗不依从性的患者被随机(1:1)分配到接受特定的 3 个月计划以提高依从性(INT = 干预)或常规随访(C = 对照)。抗高血压治疗不做任何调整,只有被随机分配到干预组的患者才会了解到不坚持治疗的情况。在随机分组前和分组 3 米时,所有患者都接受了抗高血压药物尿检和 24 小时卧床血压监测。45 名患者(36% 为女性,平均年龄:58 ± 13 岁)被随机分组。3 米时,24 小时收缩压和 24 小时舒张压的平均值(95% CI)差异(INT 与 C)分别为 12.2 mmHg (4.3-20.8),调整后 P = 0.032 和 8.7 mmHg (2.5-14.8),调整后 P = 0.018。诊室收缩压和舒张压的差异(INT 与 C)分别为 18.4 mmHg(6.8-30.1)和 15.7 mmHg(7.2-24.2),调整后 p = 0.005。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Hypertension Research
医学-外周血管病
CiteScore
7.40
自引率
16.70%
发文量
249
审稿时长
3-8 weeks
期刊介绍:
Hypertension Research is the official publication of the Japanese Society of Hypertension. The journal publishes papers reporting original clinical and experimental research that contribute to the advancement of knowledge in the field of hypertension and related cardiovascular diseases. The journal publishes Review Articles, Articles, Correspondence and Comments.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


