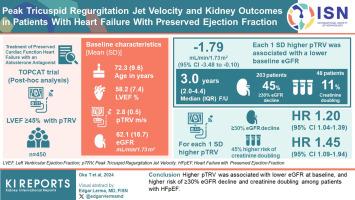
Peak Tricuspid Regurgitation Jet Velocity and Kidney Outcomes in Patients With Heart Failure With Preserved Ejection Fraction
IF 5.7
2区 医学
Q1 UROLOGY & NEPHROLOGY
引用次数: 0
Abstract
Introduction
Although venous congestion secondary to elevated pulmonary artery pressure (PAP) has been hypothesized to worsen kidney function, the association of peak tricuspid regurgitation jet velocity (pTRV), a surrogate of PAP, with kidney outcomes remains uncertain in heart failure (HF) with preserved ejection fraction (HFpEF).
Methods
This post hoc analysis of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial analyzed participants with a left ventricular ejection fraction (LVEF) of ≥45% who had pTRV measured by echocardiography at baseline. For the cross-sectional analysis, the association of baseline pTRV with baseline estimated glomerular filtration rate (eGFR) was assessed using linear regression. For the longitudinal analysis, the association of baseline pTRV with decline in eGFR of ≥30% and doubling of serum creatinine was assessed using Cox proportional hazards models.
Results
Among 450 participants, the mean (SD) baseline age, LVEF, pTRV, and eGFR were 72.3 (9.6) years, 58.2% (7.4%), 2.8 (0.5) m/s, and 62.1 (18.7) ml/min per 1.73 m2, respectively. Each 1 SD higher pTRV was associated with a lower baseline eGFR (coefficient, −1.79; 95% confidence interval [CI], −3.48 to −0.10 ml/min per 1.73 m2). Over a median (interquartile range) follow-up of 3.0 (2.0–4.4) years, 203 (45%) patients experienced ≥30% eGFR decline, and 48 (11%) experienced creatinine doubling. Each 1 SD higher pTRV was associated with a 20% higher risk of ≥30% eGFR decline (hazard ratio [HR], 1.20; 95% CI, 1.04–1.39) and a 45% higher risk of creatinine doubling (HR, 1.45; 95% CI, 1.09–1.94).
Conclusions
Higher pTRV was associated with lower eGFR at baseline, and higher risk of ≥30% eGFR decline and creatinine doubling among patients with HFpEF.
射血分数保留型心力衰竭患者的三尖瓣反流射流速度峰值与肾脏预后
导言尽管肺动脉压(PAP)升高引起的静脉充血被认为会恶化肾功能,但在射血分数保留型心力衰竭(HFpEF)患者中,三尖瓣反流喷射速度峰值(pTRV)(PAP的替代指标)与肾脏预后的关系仍不确定。方法这项醛固酮拮抗剂治疗保留心功能心衰(TOPCAT)试验的事后分析分析了左室射血分数(LVEF)≥45%、基线时通过超声心动图测量 pTRV 的参与者。在横断面分析中,使用线性回归评估了基线 pTRV 与基线肾小球滤过率(eGFR)的关系。结果 450 名参与者的平均(标度)基线年龄、LVEF、pTRV 和 eGFR 分别为 72.3 (9.6) 岁、58.2% (7.4%)、2.8 (0.5) m/s 和 62.1 (18.7) ml/min per 1.73 m2。pTRV 每升高 1 SD,基线 eGFR 就降低(系数,-1.79;95% 置信区间 [CI],-3.48 至-0.10 ml/min per 1.73 m2)。在 3.0 (2.0-4.4) 年的中位(四分位数间距)随访期间,203 名(45%)患者的 eGFR 下降了≥30%,48 名(11%)患者的肌酐翻了一番。pTRV 每增加 1 SD,eGFR 下降≥30% 的风险就增加 20%(危险比 [HR],1.20;95% CI,1.04-1.39),肌酐翻倍的风险增加 45%(HR,1.45;95% CI,1.09-1.94)。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊
Kidney International Reports
Medicine-Nephrology
CiteScore
7.70
自引率
3.30%
发文量
1578
审稿时长
8 weeks
期刊介绍:
Kidney International Reports, an official journal of the International Society of Nephrology, is a peer-reviewed, open access journal devoted to the publication of leading research and developments related to kidney disease. With the primary aim of contributing to improved care of patients with kidney disease, the journal will publish original clinical and select translational articles and educational content related to the pathogenesis, evaluation and management of acute and chronic kidney disease, end stage renal disease (including transplantation), acid-base, fluid and electrolyte disturbances and hypertension. Of particular interest are submissions related to clinical trials, epidemiology, systematic reviews (including meta-analyses) and outcomes research. The journal will also provide a platform for wider dissemination of national and regional guidelines as well as consensus meeting reports.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


