Gabriel Marinheiro, Beatriz Araújo, André Rivera, Gabriel de Almeida Monteiro, Laís Silva Santana, Marianna Leite, Antonio Mutarelli, Agostinho C Pinheiro, Eberval Gadelha Figueiredo, João Paulo Mota Telles
{"title":"Direct oral anticoagulants in embolic stroke of undetermined source: an updated meta-analysis.","authors":"Gabriel Marinheiro, Beatriz Araújo, André Rivera, Gabriel de Almeida Monteiro, Laís Silva Santana, Marianna Leite, Antonio Mutarelli, Agostinho C Pinheiro, Eberval Gadelha Figueiredo, João Paulo Mota Telles","doi":"10.1007/s11239-024-03017-7","DOIUrl":null,"url":null,"abstract":"<p><p>The efficacy and safety of direct oral anticoagulants (DOAC) in patients with embolic stroke of undetermined source (ESUS) remains unclear. We systematically searched PubMed, Embase, and Cochrane Library for randomized controlled trials (RCT) comparing DOACs versus aspirin in patients with ESUS. Risk ratios (RR) and 95% confidence intervals (CI) were computed for binary endpoints. Four RCTs comprising 13,970 patients were included. Compared with aspirin, DOACs showed no significant reduction of recurrent stroke (RR 0.95; 95% CI 0.84-1.09; p = 0.50; I<sup>2</sup> = 0%), ischemic stroke or systemic embolism (RR 0.97; 95% CI 0.80-1.17; p = 0.72; I<sup>2</sup> = 0%), ischemic stroke (RR 0.92; 95% CI 0.79-1.06; p = 0.23; I<sup>2</sup> = 0%), and all-cause mortality (RR 1.11; 95% CI 0.87-1.42; p = 0.39; I<sup>2</sup> = 0%). DOACs increased the risk of clinically relevant non-major bleeding (CRNB) (RR 1.52; 95% CI 1.20-1.93; p < 0.01; I<sup>2</sup> = 7%) compared with aspirin, while no significant difference was observed in major bleeding between groups (RR 1.57; 95% CI 0.87-2.83; p = 0.14; I<sup>2</sup> = 63%). In a subanalysis of patients with non-major risk factors for cardioembolism, there is no difference in recurrent stroke (RR 0.98; 95% CI 0.67-1.42; p = 0.90; I<sup>2</sup> = 0%), all-cause mortality (RR 1.24; 95% CI 0.58-2.66; p = 0.57; I<sup>2</sup> = 0%), and major bleeding (RR 1.00, 95% CI 0.32-3.08; p = 1.00; I<sup>2</sup> = 0%) between groups. In patients with ESUS, DOACs did not reduce the risk of recurrent stroke, ischemic stroke or systemic embolism, or all-cause mortality. Although there was a significant increase in clinically relevant non-major bleeding, major bleeding was similar between DOACs and aspirin.</p>","PeriodicalId":17546,"journal":{"name":"Journal of Thrombosis and Thrombolysis","volume":" ","pages":"1163-1171"},"PeriodicalIF":2.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thrombosis and Thrombolysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11239-024-03017-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
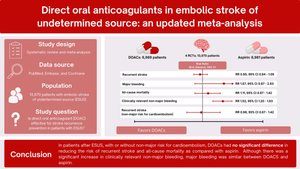
The efficacy and safety of direct oral anticoagulants (DOAC) in patients with embolic stroke of undetermined source (ESUS) remains unclear. We systematically searched PubMed, Embase, and Cochrane Library for randomized controlled trials (RCT) comparing DOACs versus aspirin in patients with ESUS. Risk ratios (RR) and 95% confidence intervals (CI) were computed for binary endpoints. Four RCTs comprising 13,970 patients were included. Compared with aspirin, DOACs showed no significant reduction of recurrent stroke (RR 0.95; 95% CI 0.84-1.09; p = 0.50; I2 = 0%), ischemic stroke or systemic embolism (RR 0.97; 95% CI 0.80-1.17; p = 0.72; I2 = 0%), ischemic stroke (RR 0.92; 95% CI 0.79-1.06; p = 0.23; I2 = 0%), and all-cause mortality (RR 1.11; 95% CI 0.87-1.42; p = 0.39; I2 = 0%). DOACs increased the risk of clinically relevant non-major bleeding (CRNB) (RR 1.52; 95% CI 1.20-1.93; p < 0.01; I2 = 7%) compared with aspirin, while no significant difference was observed in major bleeding between groups (RR 1.57; 95% CI 0.87-2.83; p = 0.14; I2 = 63%). In a subanalysis of patients with non-major risk factors for cardioembolism, there is no difference in recurrent stroke (RR 0.98; 95% CI 0.67-1.42; p = 0.90; I2 = 0%), all-cause mortality (RR 1.24; 95% CI 0.58-2.66; p = 0.57; I2 = 0%), and major bleeding (RR 1.00, 95% CI 0.32-3.08; p = 1.00; I2 = 0%) between groups. In patients with ESUS, DOACs did not reduce the risk of recurrent stroke, ischemic stroke or systemic embolism, or all-cause mortality. Although there was a significant increase in clinically relevant non-major bleeding, major bleeding was similar between DOACs and aspirin.
期刊介绍:
The Journal of Thrombosis and Thrombolysis is a long-awaited resource for contemporary cardiologists, hematologists, vascular medicine specialists and clinician-scientists actively involved in treatment decisions and clinical investigation of thrombotic disorders involving the cardiovascular and cerebrovascular systems. The principal focus of the Journal centers on the pathobiology of thrombosis and vascular disorders and the use of anticoagulants, platelet antagonists, cell-based therapies and interventions in scientific investigation, clinical-translational research and patient care.
The Journal will publish original work which emphasizes the interface between fundamental scientific principles and clinical investigation, stimulating an interdisciplinary and scholarly dialogue in thrombosis and vascular science. Published works will also define platforms for translational research, drug development, clinical trials and patient-directed applications. The Journal of Thrombosis and Thrombolysis'' integrated format will expand the reader''s knowledge base and provide important insights for both the investigation and direct clinical application of the most rapidly growing fields in medicine-thrombosis and vascular science.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


