{"title":"Let us not forget postpartum manic or mixed episodes","authors":"Verinder Sharma","doi":"10.1111/bdi.13479","DOIUrl":null,"url":null,"abstract":"<p>In the nineteenth century, the estimated prevalence of puerperal mania varied from 1 in 80–800 deliveries.<span><sup>1</sup></span> The literature from this era is replete with clinical accounts of puerperal mania and melancholia in women admitted to Victorian asylums. Changes in the nosology and interpretation of postpartum psychiatric disorder in the 20th century have produced lower rates of postpartum mania. For example, some cases of puerperal mania would be diagnosed as delirium or a toxic confusional state in today's terminology. Other factors have contributed to waning interest in puerperal mania. Coinciding with the deinstitutionalization process of replacing long-stay psychiatric hospitals with community mental health services, the research focus shifted from the study of severe psychopathology to commonly encountered conditions in the community such as baby blues and postpartum depression. The term third-day depression after childbirth, also known as the baby blues, was first described in 1952 but has a larger share of literature than postpartum mania. An ‘unofficial’ but popular nomenclature includes baby blues, postpartum depression, and postpartum psychosis but makes no direct mention of manic or mixed episodes. Postpartum psychosis denotes disparate conditions including brief psychotic disorder, manic or mixed episodes with or without psychotic features, and major depressive episodes with psychosis.<span><sup>2</sup></span> The usurping of manic and mixed episodes by postpartum psychosis likely led to a lack of interest in the study of postpartum mania as shown in Figure 1.</p><p>Of mood and anxiety disorders, bipolar disorder carries the highest risk of recurrence in the postpartum period. Studies over the last few decades have demonstrated that postpartum bipolar disorder is common in community and clinical settings. A study of 10.000 women from the US found that approximately 14% of women screened positive for postpartum depression. Of those who screened positively, 23% had bipolar disorder, the most common type being bipolar I disorder (49.7%).<span><sup>3</sup></span> This means that approximately 1.6% of women in the community have a bipolar I mood episode after delivery. A recent study estimated that 39% of women with bipolar I disorder have a postpartum relapse. Of those with a postpartum relapse, 38% had a manic or mixed episode yielding an estimated prevalence of 14.82% among women with bipolar I disorder.<span><sup>4</sup></span> This is likely an underestimate because mania can occur spontaneously in the absence of psychiatric illness. As a comparison, the global prevalence of postpartum psychosis is only 0.089 to 2.6 per 1000 births.<span><sup>5</sup></span></p><p>Detecting, diagnosing, and treating manic or mixed episodes in the postpartum period is challenging. Owing to their onset typically within the first few weeks following childbirth, and the lack of information about the timing of the onset of “postpartum” episodes, early identification of manic or mixed episodes poses difficulties. These episodes may begin during pregnancy but may be difficult to detect until after delivery due to the overlap of symptoms of pregnancy with symptoms of the disorder. For example, sleep disruption is common in pregnancy, but decreased sleep requirement is also an early symptom of impending manic or mixed episodes. Further, even though childbirth is considered a potent trigger of manic and mixed episodes, it is difficult to predict the polarity of the recurrence.</p><p>Over the last few years, professional bodies have issued guidelines for the detection of manic symptoms during and after pregnancy. The Canadian Network for Mood and Anxiety Treatments and International Society for Bipolar Disorders guidelines recommend that <i>all</i> women with depressive symptoms during or after pregnancy be screened with the Mood Disorder Questionnaire alone, or in combination with the Edinburgh Postnatal Depression Scale. The American College of Obstetrics and Gynecology has made the same recommendation emphasizing that bipolar disorder should be ruled out before trying an antidepressant for a depressive episode before or after delivery. Unfortunately, screening for bipolar disorder, an illness that is associated with an increased risk of psychiatric hospitalization and safety concerns for the mother and her child remains uncommon.</p><p>The lack of treatment studies poses a further challenge. The randomized controlled data on pharmacotherapy of bipolar disorder is limited to a single-blind trial of 26 participants (including 16 with type I disorder) that found divalproex was not significantly more effective than monitoring without medication for the prevention of episodes of bipolar disorder after delivery. Lithium is commonly recommended for acute and preventative treatment of postpartum psychosis; however, it has not been systematically studied in women with bipolar I disorder. Similarly, there is no controlled data on quetiapine or olanzapine. Manic or mixed episodes should be easily preventable given the proximity of these episodes to delivery, the circumscribed nature of the risk period, and knowledge of putative risk factors including sleep loss.</p><p>Studies have demonstrated a lower risk of postpartum recurrence among women receiving medication versus those without; however, the lack of details on the specifics of treatment makes it difficult to apply this information at the individual level. In most studies, patients were treated with polypharmacy including antidepressants, anxiolytics, and mood stabilizers. The randomized controlled data on pharmacotherapy is limited to a single-blind trial that found divalproex was not significantly more effective than monitoring without medication for the prevention of episodes of bipolar disorder after delivery. Lithium is commonly recommended for acute and preventative treatment of postpartum psychosis; however, it has not been systematically studied in women with postpartum manic or mixed episodes. A small study found olanzapine alone or in combination with other medications (antidepressants and or mood stabilizers), was effective in preventing psychotic and mood episodes in women with bipolar disorder. There is preliminary evidence that quetiapine may be effective in the acute or preventative treatment of bipolar disorder.</p><p>In conclusion, postpartum manic and mixed episodes are common but appear to be overlooked. Lack of awareness of their prevalence and the consequent scarcity of postpartum screening for manic symptoms may contribute to their delayed diagnosis and occasional tragic consequences. A targeted treatment approach to prevent the postpartum recurrence of manic or mixed episodes might be more effective and economical than focusing on the prevention of postpartum psychosis. In general, it is easier to prevent manic or mixed episodes than periods of depression. Also, prevention of manic or mixed episodes might prevent depression in women with a mania-depression interval course. More research is necessary to clarify the phenotype of postpartum mania, including the prodromal symptoms, the timing of onset, and its relationship with postpartum bipolar depression. Due to the pathoplastic effect of childbirth, mixed symptoms are more common during the postpartum versus non-postpartum episodes. Another important area of inquiry is the determination of predominant polarity among women with bipolar I disorder who have a preponderance of manic or mixed episodes postpartum. Studies are urgently needed to assess the efficacy of medication and psychotherapy in the prevention of bipolar mood episodes in the postpartum period.</p><p>The author has no conflicts of interest to disclose.</p>","PeriodicalId":8959,"journal":{"name":"Bipolar Disorders","volume":"26 6","pages":"529-531"},"PeriodicalIF":4.5000,"publicationDate":"2024-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/bdi.13479","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bipolar Disorders","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/bdi.13479","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
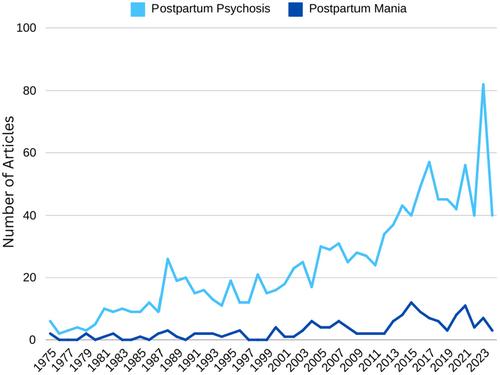
In the nineteenth century, the estimated prevalence of puerperal mania varied from 1 in 80–800 deliveries.1 The literature from this era is replete with clinical accounts of puerperal mania and melancholia in women admitted to Victorian asylums. Changes in the nosology and interpretation of postpartum psychiatric disorder in the 20th century have produced lower rates of postpartum mania. For example, some cases of puerperal mania would be diagnosed as delirium or a toxic confusional state in today's terminology. Other factors have contributed to waning interest in puerperal mania. Coinciding with the deinstitutionalization process of replacing long-stay psychiatric hospitals with community mental health services, the research focus shifted from the study of severe psychopathology to commonly encountered conditions in the community such as baby blues and postpartum depression. The term third-day depression after childbirth, also known as the baby blues, was first described in 1952 but has a larger share of literature than postpartum mania. An ‘unofficial’ but popular nomenclature includes baby blues, postpartum depression, and postpartum psychosis but makes no direct mention of manic or mixed episodes. Postpartum psychosis denotes disparate conditions including brief psychotic disorder, manic or mixed episodes with or without psychotic features, and major depressive episodes with psychosis.2 The usurping of manic and mixed episodes by postpartum psychosis likely led to a lack of interest in the study of postpartum mania as shown in Figure 1.
Of mood and anxiety disorders, bipolar disorder carries the highest risk of recurrence in the postpartum period. Studies over the last few decades have demonstrated that postpartum bipolar disorder is common in community and clinical settings. A study of 10.000 women from the US found that approximately 14% of women screened positive for postpartum depression. Of those who screened positively, 23% had bipolar disorder, the most common type being bipolar I disorder (49.7%).3 This means that approximately 1.6% of women in the community have a bipolar I mood episode after delivery. A recent study estimated that 39% of women with bipolar I disorder have a postpartum relapse. Of those with a postpartum relapse, 38% had a manic or mixed episode yielding an estimated prevalence of 14.82% among women with bipolar I disorder.4 This is likely an underestimate because mania can occur spontaneously in the absence of psychiatric illness. As a comparison, the global prevalence of postpartum psychosis is only 0.089 to 2.6 per 1000 births.5
Detecting, diagnosing, and treating manic or mixed episodes in the postpartum period is challenging. Owing to their onset typically within the first few weeks following childbirth, and the lack of information about the timing of the onset of “postpartum” episodes, early identification of manic or mixed episodes poses difficulties. These episodes may begin during pregnancy but may be difficult to detect until after delivery due to the overlap of symptoms of pregnancy with symptoms of the disorder. For example, sleep disruption is common in pregnancy, but decreased sleep requirement is also an early symptom of impending manic or mixed episodes. Further, even though childbirth is considered a potent trigger of manic and mixed episodes, it is difficult to predict the polarity of the recurrence.
Over the last few years, professional bodies have issued guidelines for the detection of manic symptoms during and after pregnancy. The Canadian Network for Mood and Anxiety Treatments and International Society for Bipolar Disorders guidelines recommend that all women with depressive symptoms during or after pregnancy be screened with the Mood Disorder Questionnaire alone, or in combination with the Edinburgh Postnatal Depression Scale. The American College of Obstetrics and Gynecology has made the same recommendation emphasizing that bipolar disorder should be ruled out before trying an antidepressant for a depressive episode before or after delivery. Unfortunately, screening for bipolar disorder, an illness that is associated with an increased risk of psychiatric hospitalization and safety concerns for the mother and her child remains uncommon.
The lack of treatment studies poses a further challenge. The randomized controlled data on pharmacotherapy of bipolar disorder is limited to a single-blind trial of 26 participants (including 16 with type I disorder) that found divalproex was not significantly more effective than monitoring without medication for the prevention of episodes of bipolar disorder after delivery. Lithium is commonly recommended for acute and preventative treatment of postpartum psychosis; however, it has not been systematically studied in women with bipolar I disorder. Similarly, there is no controlled data on quetiapine or olanzapine. Manic or mixed episodes should be easily preventable given the proximity of these episodes to delivery, the circumscribed nature of the risk period, and knowledge of putative risk factors including sleep loss.
Studies have demonstrated a lower risk of postpartum recurrence among women receiving medication versus those without; however, the lack of details on the specifics of treatment makes it difficult to apply this information at the individual level. In most studies, patients were treated with polypharmacy including antidepressants, anxiolytics, and mood stabilizers. The randomized controlled data on pharmacotherapy is limited to a single-blind trial that found divalproex was not significantly more effective than monitoring without medication for the prevention of episodes of bipolar disorder after delivery. Lithium is commonly recommended for acute and preventative treatment of postpartum psychosis; however, it has not been systematically studied in women with postpartum manic or mixed episodes. A small study found olanzapine alone or in combination with other medications (antidepressants and or mood stabilizers), was effective in preventing psychotic and mood episodes in women with bipolar disorder. There is preliminary evidence that quetiapine may be effective in the acute or preventative treatment of bipolar disorder.
In conclusion, postpartum manic and mixed episodes are common but appear to be overlooked. Lack of awareness of their prevalence and the consequent scarcity of postpartum screening for manic symptoms may contribute to their delayed diagnosis and occasional tragic consequences. A targeted treatment approach to prevent the postpartum recurrence of manic or mixed episodes might be more effective and economical than focusing on the prevention of postpartum psychosis. In general, it is easier to prevent manic or mixed episodes than periods of depression. Also, prevention of manic or mixed episodes might prevent depression in women with a mania-depression interval course. More research is necessary to clarify the phenotype of postpartum mania, including the prodromal symptoms, the timing of onset, and its relationship with postpartum bipolar depression. Due to the pathoplastic effect of childbirth, mixed symptoms are more common during the postpartum versus non-postpartum episodes. Another important area of inquiry is the determination of predominant polarity among women with bipolar I disorder who have a preponderance of manic or mixed episodes postpartum. Studies are urgently needed to assess the efficacy of medication and psychotherapy in the prevention of bipolar mood episodes in the postpartum period.
The author has no conflicts of interest to disclose.
期刊介绍:
Bipolar Disorders is an international journal that publishes all research of relevance for the basic mechanisms, clinical aspects, or treatment of bipolar disorders and related illnesses. It intends to provide a single international outlet for new research in this area and covers research in the following areas:
biochemistry
physiology
neuropsychopharmacology
neuroanatomy
neuropathology
genetics
brain imaging
epidemiology
phenomenology
clinical aspects
and therapeutics of bipolar disorders
Bipolar Disorders also contains papers that form the development of new therapeutic strategies for these disorders as well as papers on the topics of schizoaffective disorders, and depressive disorders as these can be cyclic disorders with areas of overlap with bipolar disorders.
The journal will consider for publication submissions within the domain of: Perspectives, Research Articles, Correspondence, Clinical Corner, and Reflections. Within these there are a number of types of articles: invited editorials, debates, review articles, original articles, commentaries, letters to the editors, clinical conundrums, clinical curiosities, clinical care, and musings.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


