{"title":"Endobronchial Infection and Bacterial Lymphadenitis by <i>Gemella morbillorum</i> Leading to Airway Perforation and a Bronchopleural Fistula.","authors":"Kaitlin N DePrez, John Ferguson","doi":"10.1155/2024/8850287","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction:</b> Necrotizing bronchial infection with severe infectious lymphadenitis is infrequently encountered and most commonly ascribed to <i>Aspergillus</i>, <i>Histoplasma</i>, and <i>Mycobacterium</i> species. We present a unique cause of severe airway destruction with lymphadenitis and bronchopleural fistula formation by the bacterium <i>Gemella morbillorum</i>. <b>Case:</b> A 24-year-old man presented with acute symptoms of vomiting, fever, and shoulder pain. A CT of the chest demonstrated a large subcarinal mass encasing the central bronchi. The workup for malignant, fungal, and granulomatous etiologies was unrevealing, while blood cultures identified <i>G. morbillorum</i>. Fiberoptic bronchoscopy revealed a perforation of the right middle lobar bronchus and the formation of a bronchopleural fistula, resulting in a large hydropneumothorax with empyema. Despite antibiotic therapy, surgical intervention to repair the fistula, and ventilatory support, the progression of the bronchopleural fistula led to fatal respiratory failure. <b>Conclusion:</b> In cases of severe mediastinal adenopathy in a young patient, bacterial lymphadenitis should be considered in the differential diagnosis with lymphoma, germ cell tumor, granulomatosis with polyangiitis, sarcoidosis, histoplasmosis, and inflammatory myofibroblastic tumor.</p>","PeriodicalId":52364,"journal":{"name":"Case Reports in Pulmonology","volume":"2024 ","pages":"8850287"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11268966/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pulmonology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/8850287","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
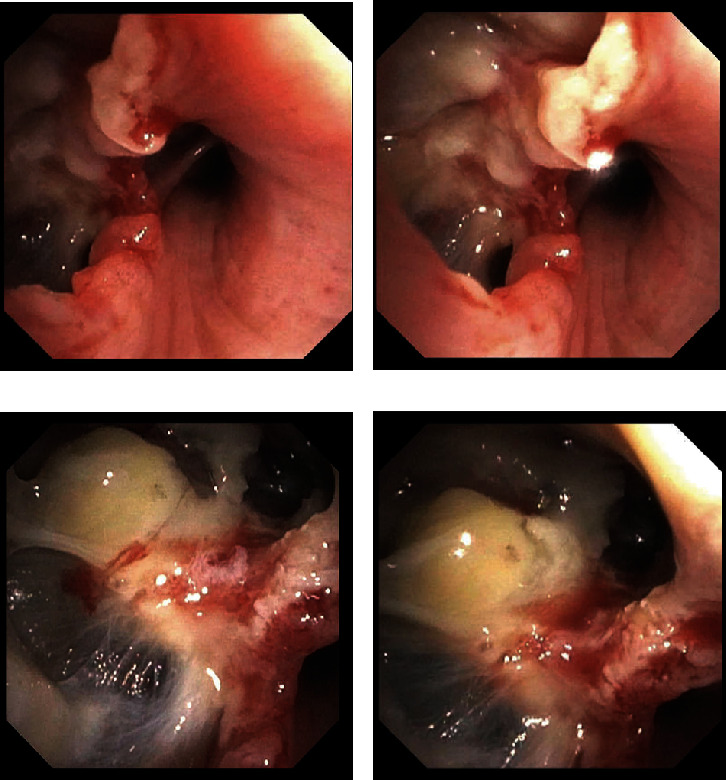
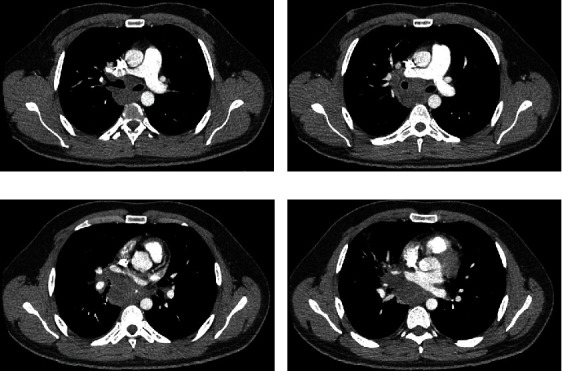
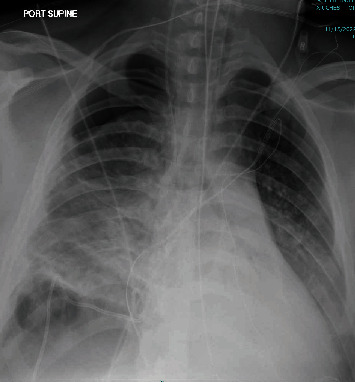
Introduction: Necrotizing bronchial infection with severe infectious lymphadenitis is infrequently encountered and most commonly ascribed to Aspergillus, Histoplasma, and Mycobacterium species. We present a unique cause of severe airway destruction with lymphadenitis and bronchopleural fistula formation by the bacterium Gemella morbillorum. Case: A 24-year-old man presented with acute symptoms of vomiting, fever, and shoulder pain. A CT of the chest demonstrated a large subcarinal mass encasing the central bronchi. The workup for malignant, fungal, and granulomatous etiologies was unrevealing, while blood cultures identified G. morbillorum. Fiberoptic bronchoscopy revealed a perforation of the right middle lobar bronchus and the formation of a bronchopleural fistula, resulting in a large hydropneumothorax with empyema. Despite antibiotic therapy, surgical intervention to repair the fistula, and ventilatory support, the progression of the bronchopleural fistula led to fatal respiratory failure. Conclusion: In cases of severe mediastinal adenopathy in a young patient, bacterial lymphadenitis should be considered in the differential diagnosis with lymphoma, germ cell tumor, granulomatosis with polyangiitis, sarcoidosis, histoplasmosis, and inflammatory myofibroblastic tumor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


