Melissa Blanco, Chiara Monopoli-Roca, Marta Álvarez de Linera-Alperi, Pablo Menéndez Fernández-Miranda, Bárbara Molina, Angel Batuecas-Caletrío, Nicolás Pérez-Fernández
{"title":"Visual Fixation of Skull-Vibration-Induced Nystagmus in Patients with Peripheral Vestibulopathy.","authors":"Melissa Blanco, Chiara Monopoli-Roca, Marta Álvarez de Linera-Alperi, Pablo Menéndez Fernández-Miranda, Bárbara Molina, Angel Batuecas-Caletrío, Nicolás Pérez-Fernández","doi":"10.3390/audiolres14040047","DOIUrl":null,"url":null,"abstract":"<p><p>Nystagmus induced by applying an intense vibratory stimulus to the skull (SVIN) indicates vestibular functional asymmetry. In unilateral vestibular loss, a 100 Hz bone-conducted vibration given to either mastoid immediately causes a primarily horizontal nystagmus. The test is performed in darkness to avoid visual fixation (VF) but there are no data about how much VF affects the often-intense SVIN. The aim is to analyze the amount of reduction in SVIN when VF is allowed during testing. Thus, all patients seen in a tertiary hospital for vertigo or dizziness with positive SVIN were included. SVIN was recorded for 10 s for each condition: without VF (aSVINwo) and with VF (aSVINw). We obtained an aSVINwo and an aSVINw as average slow-phase velocities (SPV) without and with VF. VF index (FI<sub>SVIN</sub>) was calculated as the ratio of SPV. Among the 124 patients included, spontaneous nystagmus (SN) was found in 25% and the median slow phase velocity (mSPV) (without VF) of SN was 2.6 ± 2.4°/s. Mean FI<sub>SVIN</sub> was 0.27 ± 0.29. FI<sub>SVIN</sub> was 0 in 42 patients, and FI<sub>SVIN</sub> between 0 and 1 was found in 82 (mean FI<sub>SVIN</sub> 0.39 ± 0.02). Fixation suppression was found in all patients with SVIN in cases of peripheral vestibulopathy. FI<sub>SVIN</sub> clearly delineates two populations of patients: with or without a complete visual reduction in nystagmus.</p>","PeriodicalId":44133,"journal":{"name":"Audiology Research","volume":"14 4","pages":"562-571"},"PeriodicalIF":1.8000,"publicationDate":"2024-06-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11270166/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Audiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/audiolres14040047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"AUDIOLOGY & SPEECH-LANGUAGE PATHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
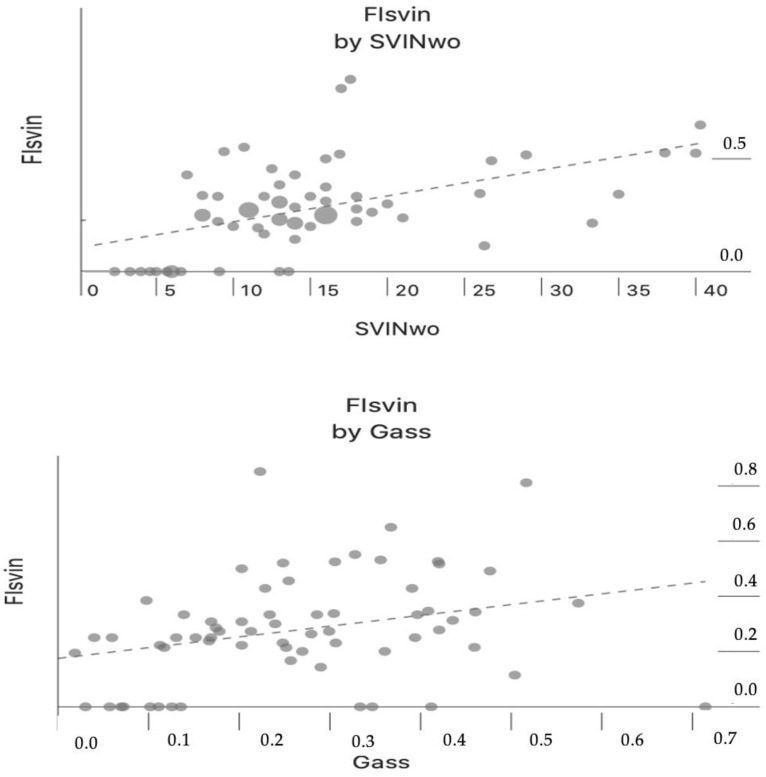
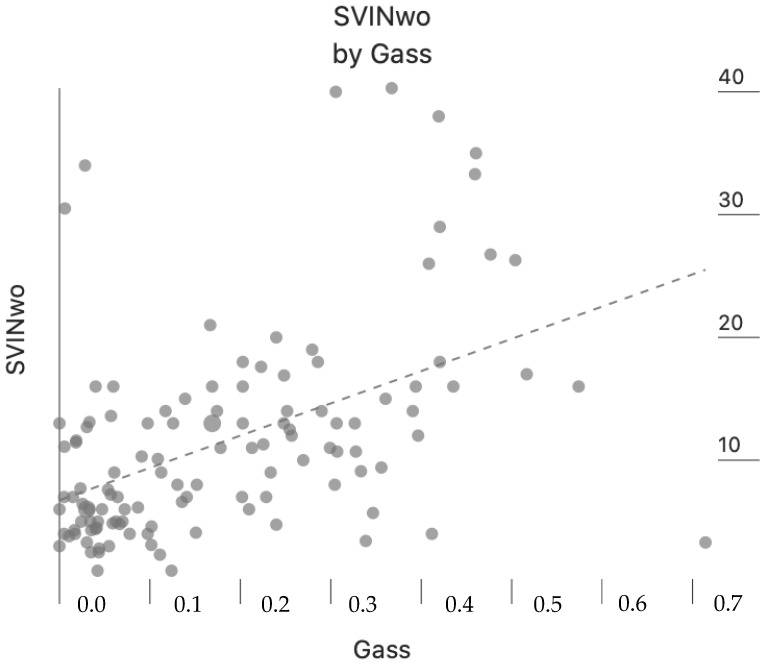
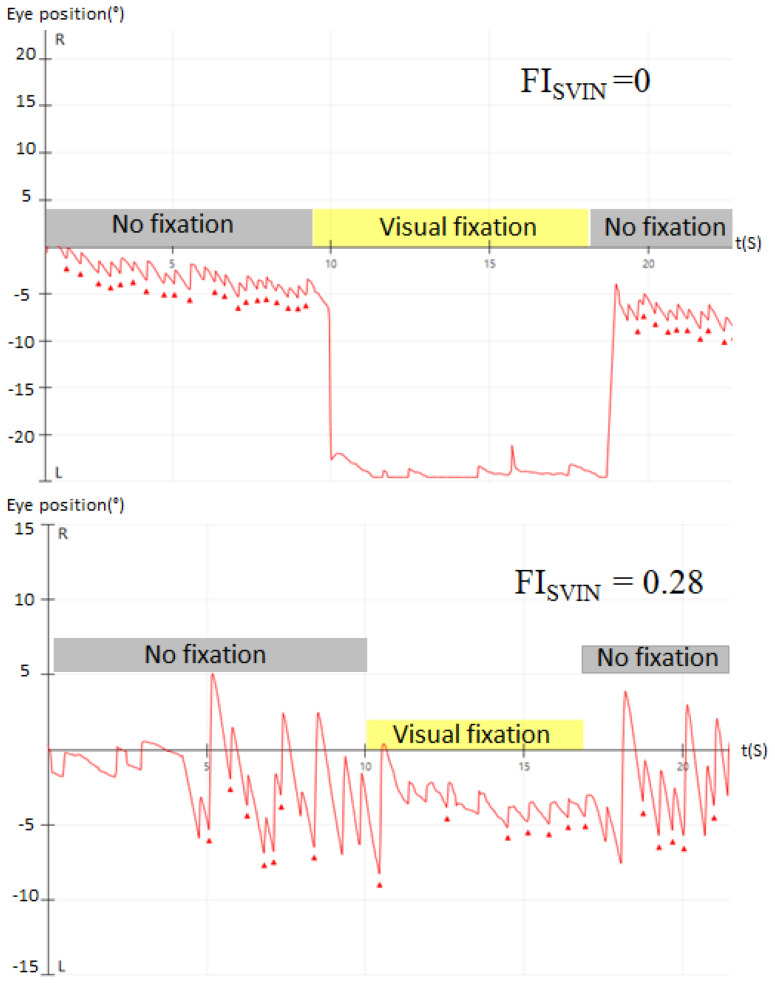
Nystagmus induced by applying an intense vibratory stimulus to the skull (SVIN) indicates vestibular functional asymmetry. In unilateral vestibular loss, a 100 Hz bone-conducted vibration given to either mastoid immediately causes a primarily horizontal nystagmus. The test is performed in darkness to avoid visual fixation (VF) but there are no data about how much VF affects the often-intense SVIN. The aim is to analyze the amount of reduction in SVIN when VF is allowed during testing. Thus, all patients seen in a tertiary hospital for vertigo or dizziness with positive SVIN were included. SVIN was recorded for 10 s for each condition: without VF (aSVINwo) and with VF (aSVINw). We obtained an aSVINwo and an aSVINw as average slow-phase velocities (SPV) without and with VF. VF index (FISVIN) was calculated as the ratio of SPV. Among the 124 patients included, spontaneous nystagmus (SN) was found in 25% and the median slow phase velocity (mSPV) (without VF) of SN was 2.6 ± 2.4°/s. Mean FISVIN was 0.27 ± 0.29. FISVIN was 0 in 42 patients, and FISVIN between 0 and 1 was found in 82 (mean FISVIN 0.39 ± 0.02). Fixation suppression was found in all patients with SVIN in cases of peripheral vestibulopathy. FISVIN clearly delineates two populations of patients: with or without a complete visual reduction in nystagmus.
期刊介绍:
The mission of Audiology Research is to publish contemporary, ethical, clinically relevant scientific researches related to the basic science and clinical aspects of the auditory and vestibular system and diseases of the ear that can be used by clinicians, scientists and specialists to improve understanding and treatment of patients with audiological and neurotological disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


