Frédéric Martino, Milan Trainel, Jessica Guillaume, Aurélien Schaffar, Simon Escalard, Adrien Pons, Nicolas Engrand
{"title":"Outcome of Aneurysmal Subarachnoid Hemorrhage Not Altered With Transatlantic Airplane Transfer: A Bicentric Matched Case-control Study.","authors":"Frédéric Martino, Milan Trainel, Jessica Guillaume, Aurélien Schaffar, Simon Escalard, Adrien Pons, Nicolas Engrand","doi":"10.1097/ANA.0000000000000984","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>It is recommended that ruptured cerebral aneurysms are treated in a high-volume center within 72 hours of ictus. We assessed the impact of long-distance aeromedical evacuation in patients presenting aSAH.</p><p><strong>Methods: </strong>This case-control study compared patients with aneurysmal subarachnoid hemorrhage (aSAH) who had a 6750 km air transfer from Guadeloupe (a Caribbean island) to Paris, France, for neurointerventional management in a tertiary center with a matched cohort from Paris region treated in the same center over a 10-year period (2010 to 2019). The 2 populations were matched on age, sex, World Federation of Neurological Surgeons score, and Fisher score. The primary outcome was a 1-year modified Rankin Scale score ≤3. Secondary outcomes included time from diagnosis to securing aneurysm, 1-year mortality, and a cost analysis.</p><p><strong>Results: </strong>Among 128 consecutive aSAH transferred from Guadeloupe, 93 were matched with 93 patients from the Paris area. The proportion of patients with 1-year modified Rankin Scale ≤3 (75% vs 82%, respectively; P = 0.5) and 1-year mortality (18% vs 14%, respectively; P = 0.2) was similar in the Guadeloupe and Paris groups. The median (interquartile range: Q1, Q3) time from diagnosis to securing the aneurysm was higher in the patients from Guadeloupe than those from Paris (48 [30, 63] h vs 23 [12, 24] h, respectively; P < 0.001). Guadeloupean patients received mechanical ventilation (58% vs 38%; P < 0.001) and external ventricular drainage (55% vs 39%; P = 0.005) more often than those from Paris. The additional cost of treating a Guadeloupe patient in Paris was estimated at 7580 Euros or 17% of the estimated cost in Guadeloupe.</p><p><strong>Conclusions: </strong>Long-distance aeromedical evacuation of patients with aSAH from Guadeloupe to Paris resulted in a 25-hour increase in time to aneurysm coiling embolization time but did not impact 1-year functional outcomes or mortality.</p>","PeriodicalId":16550,"journal":{"name":"Journal of neurosurgical anesthesiology","volume":" ","pages":"279-287"},"PeriodicalIF":2.4000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12147728/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgical anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/ANA.0000000000000984","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/24 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: It is recommended that ruptured cerebral aneurysms are treated in a high-volume center within 72 hours of ictus. We assessed the impact of long-distance aeromedical evacuation in patients presenting aSAH.
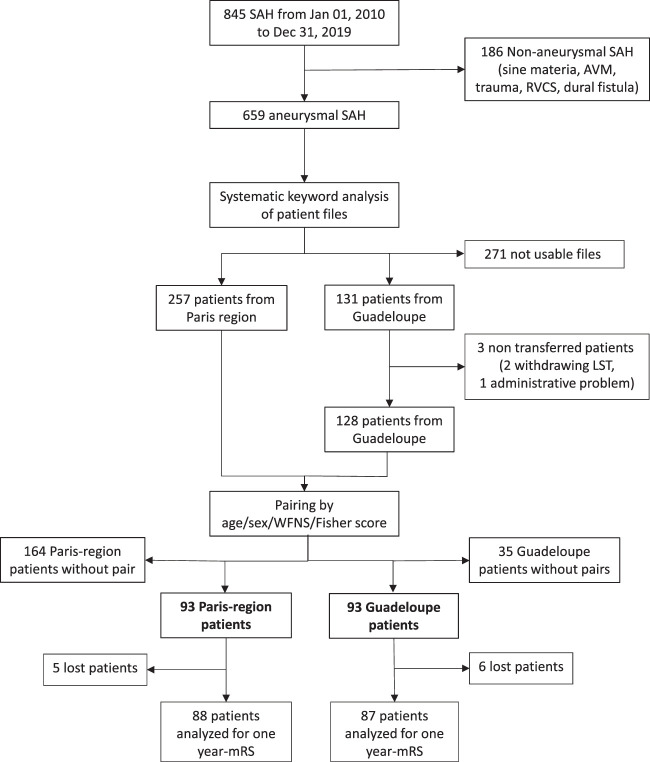
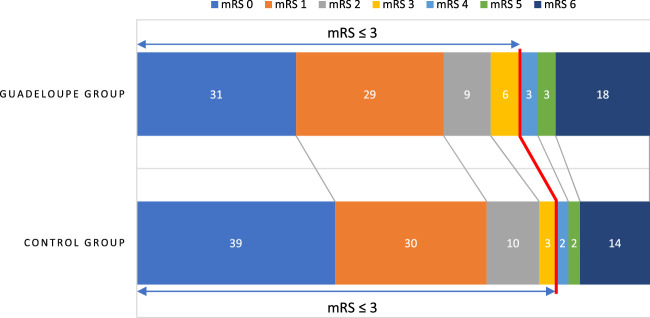
Methods: This case-control study compared patients with aneurysmal subarachnoid hemorrhage (aSAH) who had a 6750 km air transfer from Guadeloupe (a Caribbean island) to Paris, France, for neurointerventional management in a tertiary center with a matched cohort from Paris region treated in the same center over a 10-year period (2010 to 2019). The 2 populations were matched on age, sex, World Federation of Neurological Surgeons score, and Fisher score. The primary outcome was a 1-year modified Rankin Scale score ≤3. Secondary outcomes included time from diagnosis to securing aneurysm, 1-year mortality, and a cost analysis.
Results: Among 128 consecutive aSAH transferred from Guadeloupe, 93 were matched with 93 patients from the Paris area. The proportion of patients with 1-year modified Rankin Scale ≤3 (75% vs 82%, respectively; P = 0.5) and 1-year mortality (18% vs 14%, respectively; P = 0.2) was similar in the Guadeloupe and Paris groups. The median (interquartile range: Q1, Q3) time from diagnosis to securing the aneurysm was higher in the patients from Guadeloupe than those from Paris (48 [30, 63] h vs 23 [12, 24] h, respectively; P < 0.001). Guadeloupean patients received mechanical ventilation (58% vs 38%; P < 0.001) and external ventricular drainage (55% vs 39%; P = 0.005) more often than those from Paris. The additional cost of treating a Guadeloupe patient in Paris was estimated at 7580 Euros or 17% of the estimated cost in Guadeloupe.
Conclusions: Long-distance aeromedical evacuation of patients with aSAH from Guadeloupe to Paris resulted in a 25-hour increase in time to aneurysm coiling embolization time but did not impact 1-year functional outcomes or mortality.
目的:建议脑动脉瘤破裂患者在发病后 72 小时内到高流量中心接受治疗。我们评估了长途航空医疗后送对蛛网膜下腔出血患者的影响:这项病例对照研究比较了从瓜德罗普岛(加勒比海岛屿)空运6750公里到法国巴黎的动脉瘤性蛛网膜下腔出血(aSAH)患者与巴黎地区在同一中心接受神经介入治疗的匹配队列,后者在10年间(2010年至2019年)接受了治疗。两组患者的年龄、性别、世界神经外科医师联合会评分和费舍尔评分均匹配。主要结果是1年改良Rankin量表评分≤3分。次要结果包括从诊断到确保动脉瘤形成的时间、1年死亡率和成本分析:结果:从瓜德罗普岛转来的128例连续性动脉瘤并发症患者中,有93例与巴黎地区的93例患者相匹配。瓜德罗普和巴黎两组患者的1年改良Rankin量表≤3的比例(分别为75% vs 82%;P= 0.5)和1年死亡率(分别为18% vs 14%;P= 0.2)相似。瓜德罗普患者从诊断到固定动脉瘤的中位时间(四分位数间距:Q1,Q3)高于巴黎患者(分别为48 [30, 63] h vs 23 [12, 24] h;P< 0.001)。瓜德罗普患者接受机械通气(58% vs 38%;P< 0.001)和心室外引流(55% vs 39%;P= 0.005)的频率高于巴黎患者。在巴黎治疗一名瓜德罗普岛患者的额外费用估计为7580欧元,占瓜德罗普岛估计费用的17%:结论:将瓜德罗普岛脑梗死患者长途空运至巴黎会导致动脉瘤夹闭栓塞时间增加 25 小时,但不会影响 1 年的功能预后或死亡率。
期刊介绍:
The Journal of Neurosurgical Anesthesiology (JNA) is a peer-reviewed publication directed to an audience of neuroanesthesiologists, neurosurgeons, neurosurgical monitoring specialists, neurosurgical support staff, and Neurosurgical Intensive Care Unit personnel. The journal publishes original peer-reviewed studies in the form of Clinical Investigations, Laboratory Investigations, Clinical Reports, Review Articles, Journal Club synopses of current literature from related journals, presentation of Points of View on controversial issues, Book Reviews, Correspondence, and Abstracts from affiliated neuroanesthesiology societies.
JNA is the Official Journal of the Society for Neuroscience in Anesthesiology and Critical Care, the Neuroanaesthesia and Critical Care Society of Great Britain and Ireland, the Association de Neuro-Anesthésiologie Réanimation de langue Française, the Wissenschaftlicher Arbeitskreis Neuroanästhesie der Deutschen Gesellschaft fur Anästhesiologie und Intensivmedizen, the Arbeitsgemeinschaft Deutschsprachiger Neuroanästhesisten und Neuro-Intensivmediziner, the Korean Society of Neuroanesthesia, the Japanese Society of Neuroanesthesia and Critical Care, the Neuroanesthesiology Chapter of the Colegio Mexicano de Anesthesiología, the Indian Society of Neuroanesthesiology and Critical Care, and the Thai Society for Neuroanesthesia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


