Successful Application of Tocilizumab in a Patient With Neoadjuvant Immunochemotherapy-Induced Cytokine Release Syndrome
Abstract
Background
The expansion of preoperative immunochemotherapy has led to an increase in the number of patients with lung cancer receiving immune checkpoint inhibitors (ICIs). Therefore, oncologists should manage a variety of immune-related adverse events (irAEs). One of the rare, life-threatening, and recently proposed irAEs is cytokine release syndrome (CRS). Although the standard treatment of irAE is systemic administration of steroids, it has been suggested that tocilizumab may be an effective treatment option for CRS.
Case
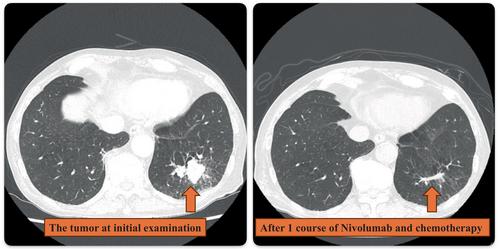
This case describes a 69-year-old man with stage IIIA lung adenocarcinoma who received chemotherapy and nivolumab, which is an ICI, as neoadjuvant immunochemotherapy. After the first administration, the patient developed severe skin rash, fever, and arthralgia. We suspected irAEs and administered systemic steroids. However, fever and arthralgia did not improve, although the skin rash disappeared. These were also significant challenges for surgery. Noting the elevated levels of inflammatory cytokines, we consulted a rheumatologist. Finally, we decided to terminate neoadjuvant therapy after one cycle and administer tocilizumab. Tocilizumab dramatically improved the patient's symptoms and allowed him to undergo radical surgery. Pathological findings revealed that the patient achieved a major pathological response.
Conclusion
This indicates the potential effectiveness of early tocilizumab administration for ICI-induced CRS, even in mild cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


