Sex and the Relationship Between Cardiometabolic Risk Factors and Estimated GFR Decline: A Population-Based Cohort Study
IF 9.4
1区 医学
Q1 UROLOGY & NEPHROLOGY
引用次数: 0
Abstract
Rationale & Objective
Females have a higher prevalence of chronic kidney disease (CKD) than males but are less likely to be treated with kidney replacement therapy (KRT). We studied the interaction between sex and the association of cardiometabolic risk factors for the decline in kidney function over time.
Study Design
A population-based cohort study.
Setting & Participants
1,127,731 adults living in Wales, United Kingdom, within the Secure Anonymised Information Linkage Databank.
Exposure
Sex and risk factors including age, estimated glomerular filtration rate (eGFR), cardiometabolic conditions, smoking, and socioeconomic deprivation. These risk factors were defined using primary care records.
Outcome
The yearly declines in eGFR and the risk of incident kidney failure defined as long-term KRT and/or sustained eGFR < 15 mL/min/1.73 m2.
Analytical Approach
Linear mixed effects models and Cox proportional hazards analysis.
Results
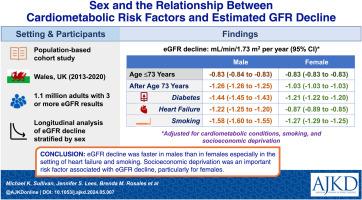
The average decline in eGFR at age ≤73 years was equal in males and females. After age 73 years, eGFR decline was faster in males than females, particularly for males with heart failure (males −1.22 mL/min/1.73 m2 per year [95% CI, −1.25 to −1.20] vs females −0.87 mL/min/1.73 m2 per year [95% CI, −0.89 to −0.85]) and current smokers (males −1.58 mL/min/1.73 m2 per year [95% CI, −1.60 to −1.55] vs females −1.27 mL/min/1.73 m2 per year [95% CI, −1.29 to −1.25]). Socioeconomic deprivation was one of the most impactful risk factors on eGFR decline among females aged >73 years, whereas cardiometabolic risk factors were more important among males. Older females at baseline were less likely to develop incident kidney failure than older males (P for age < 0.001).
Limitations
Study of people who were almost exclusively White and who had blood laboratory test data. Reliance on creatinine-based eGFR. Albuminuria and body mass index data were incomplete.
Conclusions
The eGFR decline was faster in males than in females, especially in the setting of heart failure and smoking. Socioeconomic deprivation was an important risk factor associated with eGFR decline, particularly for females. further work is required to explore less well-recognized risk factors, but these findings may inform clinical management strategies of CKD overall and within sex-specific groups.
Plain-Language Summary
Kidney function is known to decline at a faster rate among males than females. This study incorporated blood laboratory test results from the routine care of 1.1 million adults living in the United Kingdom and found that the decline in kidney function associated with risk factors varied by sex. Before and at the age of 73 years, the decline in kidney function was similar between males and females. After age 73, cardiometabolic risk factors were associated with faster decline in kidney function among males than females, specifically heart failure and smoking. Socioeconomic deprivation was also associated with the decline in kidney function for both sexes, but it was a stronger risk factor among females. These findings may inform the management of kidney disease overall and within sex-specific groups.
性别与心脏代谢风险因素和估计 GFR 下降之间的关系:一项基于人群的队列研究。
理由和目标:女性慢性肾脏病(CKD)的发病率高于男性,但接受肾脏替代治疗(KRT)的可能性较低。我们研究了随着时间的推移,肾功能下降与性别和心脏代谢风险因素之间的相互作用:基于人群的队列研究:1,127,731 名居住在英国威尔士的成年人,均在安全匿名信息链接数据库中:性别和风险因素,包括年龄、估计肾小球滤过率(eGFR)、心脏代谢疾病、吸烟和社会经济贫困程度。这些风险因素是通过初级保健记录确定的:结果:eGFR 的年下降率和发生肾衰竭的风险(定义为长期 KRT 和/或持续 eGFR2):分析方法:线性混合效应模型和考克斯比例危险分析:结果:年龄≤73岁的男性和女性的eGFR平均下降率相同。73 岁以后,男性的 eGFR 下降速度快于女性,尤其是患有心力衰竭的男性(男性为每年 -1.22 mL/min/1.73m2 ,95% 置信区间 (CI)):95%置信区间(CI)-1.25 至 -1.20,而女性为 -0.87mL/min/1.73m2:CI-0.89至-0.85)和当前吸烟者(男性-1.58 mL/min/1.73m2 per year:CI-1.60至-1.55,女性-1.27毫升/分钟/1.73平方米:CI-1.29至-1.25)。在年龄大于 73 岁的女性中,社会经济贫困是对 eGFR 下降影响最大的风险因素之一,而在男性中,心脏代谢风险因素则更为重要。与老年男性相比,基线年龄较大的女性发生肾衰竭的可能性较小(年龄的 p 值限制:研究对象几乎全部为白人,且拥有血液化验数据。依赖基于肌酐的 eGFR。结论:男性的 eGFR 下降速度快于女性,尤其是在心力衰竭和吸烟的情况下。社会经济贫困是与 eGFR 下降相关的重要风险因素,尤其是对女性而言。虽然还需要进一步研究较少被认可的风险因素,但这些研究结果可能会为整个慢性肾功能衰竭和特定性别群体的临床管理策略提供参考。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

American Journal of Kidney Diseases
医学-泌尿学与肾脏学
CiteScore
20.40
自引率
2.30%
发文量
732
审稿时长
3-8 weeks
期刊介绍:
The American Journal of Kidney Diseases (AJKD), the National Kidney Foundation's official journal, is globally recognized for its leadership in clinical nephrology content. Monthly, AJKD publishes original investigations on kidney diseases, hypertension, dialysis therapies, and kidney transplantation. Rigorous peer-review, statistical scrutiny, and a structured format characterize the publication process. Each issue includes case reports unveiling new diseases and potential therapeutic strategies.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


