Use of proton pump inhibitors after laparoscopic gastric bypass and sleeve gastrectomy: a nationwide register-based cohort study
IF 4.2
2区 医学
Q1 ENDOCRINOLOGY & METABOLISM
引用次数: 0
Abstract
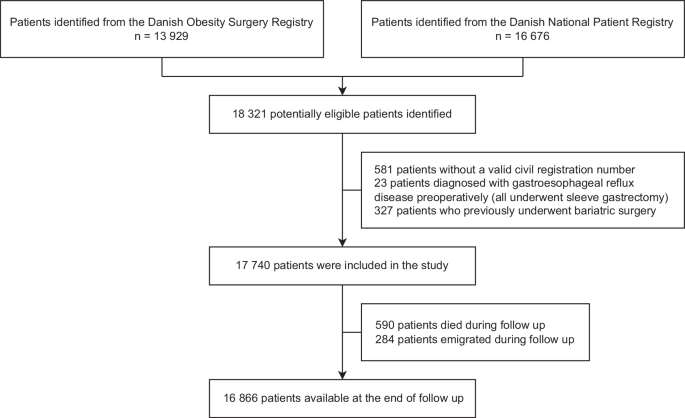
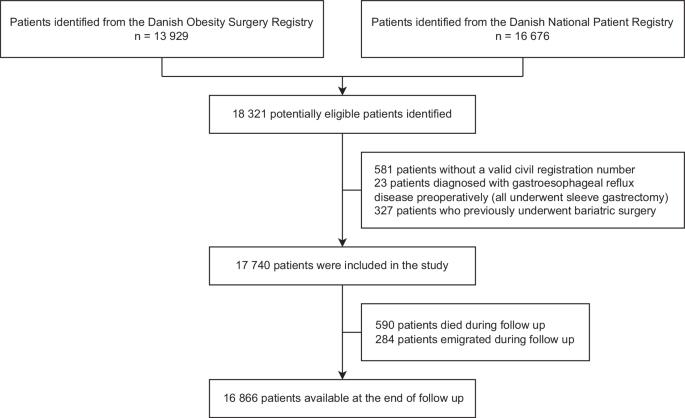
L-RYGB and L-SG are the dominant bariatric procedures worldwide. While L-RYGB is an effective treatment of coexisting gastroesophageal reflux disease (GERD), L-SG is associated with an increased risk of de-novo or worsening of GERD. The study aimed to evaluate the long-term use of proton pump inhibitors (PPI) following laparoscopic Roux-en-Y gastric bypass (L-RYGB) and sleeve gastrectomy (L-SG). This nationwide register-based study included all patients undergoing L-RYGB or L-SG in Denmark between 2008 and 2018. In total, 17,740 patients were included in the study, with 16,096 and 1671 undergoing L-RYGB and L-SG, respectively. The median follow up was 11 years after L-RYGB and 4 years after L-SG. Data were collected through Danish nationwide health registries. The development in PPI use was assessed through postoperative redeemed prescriptions. GERD development was defined by a relevant diagnosis code associated with gastroscopy, 24 h pH measurement, revisional surgery or anti-reflux surgery. The risk of initiation of PPI treatment or GERD diagnosis was evaluated using Kaplan–Meier plots and COX regression models. The risk of continuous PPI treatment was examined using logistic regression modeling. The risk of initiating PPI treatment was significantly higher after L-SG compared with L-RYGB (HR 7.06, 95% CI 6.42–7.77, p < 0.0001). The risk of continuous PPI treatment was likewise significantly higher after L-SG (OR 1.45, 95% CI 1.36–1.54, p < 0.0001). The utilization of PPI consistently increased after both procedures. The risk of GERD diagnosis was also significantly higher after L-SG compared with L-RYGB (HR 1.93, 95% CI 1.27–2.93, p < 0.0001). The risk of initiating and continuing PPI treatment was significantly higher after L-SG compared with L-RYGB, and a continuous increase in the utilization of PPI was observed after both procedures.
腹腔镜胃旁路术和袖状胃切除术后质子泵抑制剂的使用:一项基于全国登记的队列研究。
背景/目的:L-RYGB和L-SG是全球最主要的减肥手术。L-RYGB 可有效治疗并存的胃食管反流病(GERD),而 L-SG 则会增加胃食管反流病复发或恶化的风险。该研究旨在评估腹腔镜鲁氏胃旁路术(L-RYGB)和袖状胃切除术(L-SG)后质子泵抑制剂(PPI)的长期使用情况:这项基于登记的全国性研究纳入了2008年至2018年间在丹麦接受L-RYGB或L-SG手术的所有患者。共有17740名患者参与研究,其中16096人和1671人分别接受了L-RYGB和L-SG手术。L-RYGB术后的中位随访时间为11年,L-SG术后的中位随访时间为4年。数据通过丹麦全国健康登记处收集。PPI使用情况通过术后兑换处方进行评估。胃食管反流病的发展是通过与胃镜检查、24 小时 pH 值测量、翻修手术或抗反流手术相关的诊断代码来定义的。使用 Kaplan-Meier 图和 COX 回归模型评估了开始 PPI 治疗或确诊胃食管反流病的风险。使用逻辑回归模型对持续使用 PPI 治疗的风险进行了研究:结果:与 L-RYGB 相比,L-SG 术后开始 PPI 治疗的风险明显更高(HR 7.06,95% CI 6.42-7.77,P 结论:L-SG 术后开始 PPI 治疗的风险明显高于 L-RYGB:与 L-RYGB 相比,L-SG 术后开始和继续使用 PPI 治疗的风险明显更高,而且两种手术后使用 PPI 的情况都持续增加。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

International Journal of Obesity
医学-内分泌学与代谢
CiteScore
10.00
自引率
2.00%
发文量
221
审稿时长
3 months
期刊介绍:
The International Journal of Obesity is a multi-disciplinary forum for research describing basic, clinical and applied studies in biochemistry, physiology, genetics and nutrition, molecular, metabolic, psychological and epidemiological aspects of obesity and related disorders.
We publish a range of content types including original research articles, technical reports, reviews, correspondence and brief communications that elaborate on significant advances in the field and cover topical issues.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


