{"title":"Clinical Experience with Dimethyl Fumarate and Natalizumab in Pregnant Women with Multiple Sclerosis: A Four-Patient Case Series.","authors":"Satoshi Saito, Ryotaro Ikeguchi, Kazuo Kitagawa, Yuko Shimizu","doi":"10.1155/2024/7808140","DOIUrl":null,"url":null,"abstract":"<p><p>Interferon <i>β</i> and glatiramer acetate are the disease-modifying drugs (DMDs) considered relatively safe for use in pregnant women with multiple sclerosis (MS); however, the safety profile of dimethyl fumarate (DMF) and natalizumab (NTZ) in this population remains inconclusive. Here, we present four cases of pregnant women with MS who were treated with DMF and NTZ (<i>n</i> = 2 patients, each) during their pregnancy and discuss our observations with the use of these drugs and the clinical courses of the patients. We retrospectively examined relapse of MS during pregnancy and after delivery; duration of exposure to DMDs; maternal, fetal, and neonatal adverse events; breastfeeding; and timing of resumption of DMDs. The two patients treated with DMF discontinued treatment 5 or 6 weeks after the discovery of pregnancy. DMF was resumed 1 week postpartum, and mixed breastfeeding was initiated. Brain magnetic resonance imaging in one patient 9 months after delivery revealed a new lesion; however, it was not classified as a clinical relapse. In two patients treated with NTZ, the dosing interval was extended to 6 weeks after the discovery of pregnancy. One patient discontinued NTZ at 30 weeks and the other at 25 weeks of gestation, as a slight restriction in fetal growth was observed owing to hyperemesis gravidarum. Both patients opted for formula feeding, and no relapse was observed within 1 year postpartum. Additionally, no abnormalities were observed in any of the patients during the perinatal period, and their development was normal. Investigation of drug safety in pregnant and parturient women primarily relies on registries, postmarketing surveillance, and case reports due to ethical limitations on conducting randomized controlled trials. Our findings demonstrated that DMF and NTZ were not contraindicated during pregnancy or the perinatal period in women with MS; nevertheless, vigilant monitoring is essential to ensure the safety of these drugs.</p>","PeriodicalId":9615,"journal":{"name":"Case Reports in Neurological Medicine","volume":"2024 ","pages":"7808140"},"PeriodicalIF":0.9000,"publicationDate":"2024-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11265946/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurological Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/7808140","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
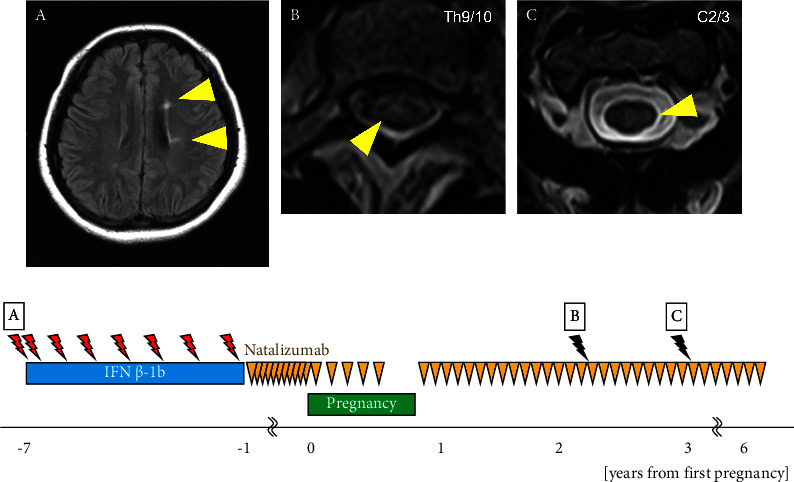
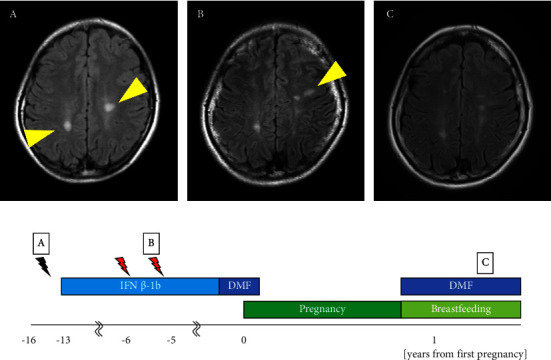
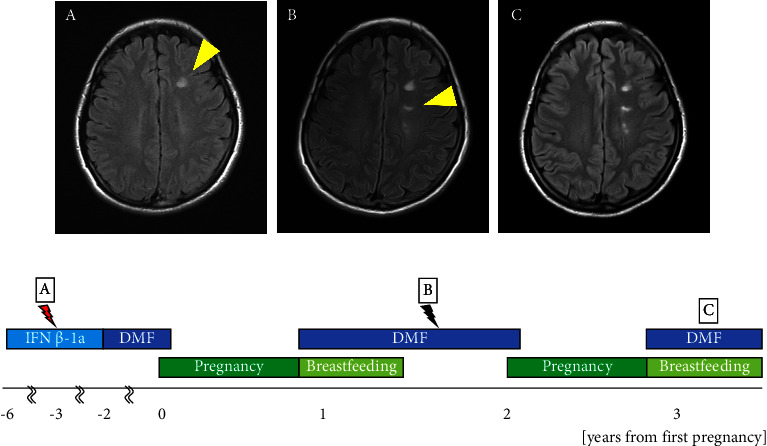
Interferon β and glatiramer acetate are the disease-modifying drugs (DMDs) considered relatively safe for use in pregnant women with multiple sclerosis (MS); however, the safety profile of dimethyl fumarate (DMF) and natalizumab (NTZ) in this population remains inconclusive. Here, we present four cases of pregnant women with MS who were treated with DMF and NTZ (n = 2 patients, each) during their pregnancy and discuss our observations with the use of these drugs and the clinical courses of the patients. We retrospectively examined relapse of MS during pregnancy and after delivery; duration of exposure to DMDs; maternal, fetal, and neonatal adverse events; breastfeeding; and timing of resumption of DMDs. The two patients treated with DMF discontinued treatment 5 or 6 weeks after the discovery of pregnancy. DMF was resumed 1 week postpartum, and mixed breastfeeding was initiated. Brain magnetic resonance imaging in one patient 9 months after delivery revealed a new lesion; however, it was not classified as a clinical relapse. In two patients treated with NTZ, the dosing interval was extended to 6 weeks after the discovery of pregnancy. One patient discontinued NTZ at 30 weeks and the other at 25 weeks of gestation, as a slight restriction in fetal growth was observed owing to hyperemesis gravidarum. Both patients opted for formula feeding, and no relapse was observed within 1 year postpartum. Additionally, no abnormalities were observed in any of the patients during the perinatal period, and their development was normal. Investigation of drug safety in pregnant and parturient women primarily relies on registries, postmarketing surveillance, and case reports due to ethical limitations on conducting randomized controlled trials. Our findings demonstrated that DMF and NTZ were not contraindicated during pregnancy or the perinatal period in women with MS; nevertheless, vigilant monitoring is essential to ensure the safety of these drugs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


